
Abstract
Background
Rare primary headaches are mainly included in Chapters 3, Trigeminal autonomic cephalalgias, and 4, Other primary headache disorders, Part One of the International Classification of Headache Disorders 3rd edition. Epidemiological data are scarce, mostly emerging from case series or small studies, with the exception of cluster headache. In order to overcome the knowledge gap about rare primary headaches, the RegistRare Network was launched in 2017 to promote research in the field.
Methods
A retrospective cohort study including patients who, from April 30, 2014 to May 1, 2017, visited seven Italian tertiary Headache Centres, was undertaken to estimate in that clinical setting prevalence and incidence of headaches included in Chapters 3 and 4, Part One of the International Classification of Headache Disorders 3rd edition. Prevalent headache is defined as a headache recorded within the study timeframe, regardless of when the diagnosis was made. Incident headache is defined as a headache diagnosed for the first time in the patient during the study period.
Results
Twenty thousand and eighty-three patients visited the participating centres, and 822 (4.1%) prevalent cases, of which 461 (2.3%) were incident cases, were registered. Headaches listed in Chapter 3 affected 668 patients, representing 81.3% of the total number of prevalent cases. Headaches listed in Chapter 4 affected 154 patients and represent 18.7% of the total number of prevalent cases. Cluster headaches represent the most frequently diagnosed rare headaches (70.4%). For 13 entities out of 20, no cases were registered in more than 50% (n ≥ 4) of the centres, and for 14 entities more than 50% of diagnoses were incident.
Conclusions
This large, multicentre study gives the first wide-ranging snapshot of the burden in clinical practice of rare headaches and confirms that cooperative networks are necessary to study rare headaches, as their prevalence is often very low. The launch of a disease registry by the RegistRare Network will favour research in this neglected population of headache patients.
Trial registration
NCT03416114.
Keywords
Introduction
According to the European Council (1), diseases are considered rare when fewer than 50 persons in 100,000 people are affected; however, in common clinical practice, for rare headache disorders the prevalence threshold is set at 1% (2). Notably, headaches whose prevalence is unknown, but which are regarded as uncommon, are also considered rare (2). According to the abovementioned criteria, rare primary headaches are mainly included in Chapter 3, Trigeminal autonomic cephalalgias (TACs) (3–6) and Chapter 4, Other primary headache disorders (7–15) of Part One of the International Classification of Headache Disorders 3rd edition (ICHD-3) (16). In ICHD-3, Chapter 3 and 4 of Part One have been quite relevantly modified in comparison to previous versions of the ICHD. First, hemicrania continua has been included in Chapter 3, since its clinical and pathophysiological features are typical of TACs (17). Second, the group of short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) (18) has been split into SUNCT and short-lasting neuralgiform headache attacks with cranial autonomic features (SUNA), according to the number of autonomic symptoms accompanying headache attacks (19). Third, the nummular headache, from the appendix of the previous classification (20), has been moved to Chapter 4, as an increasing number of case series suggested that it should be regarded as a primary headache (21,22). Finally, and similar to nummular headache, cold stimulus headache (23) and external-pressure headache (24), which were previously part of secondary headache disorders (20) were reclassified in Chapter 4.
Epidemiological data on headaches coded in Part One, Chapter 3 and 4, of ICHD-3, are scant, and most evidence concerns cluster headache, which, notwithstanding its higher prevalence in comparison to other conditions (25–28) and its exclusion from the list released by the National Institute of Health (29), may still be regarded as a rare headache (2). In a meta-analysis of 16 population-based epidemiological studies (11 from Europe, three from the US, one from Africa, and one from Asia), the pooled lifetime prevalence of cluster headache was 124 per 100,000 (0.1%), the 1-year prevalence was 53 per 100,000 and the 1-year incidence, reported only in three studies, was 2–10 per 100,000, with an overall ratio of episodic versus chronic cluster headache of 6.0 (30). Due to the paucity of data, most of which come from case reports or small cohort studies, prevalence and incidence of both TACS that differ from cluster headache and other primary headaches are not accurately estimated (2), and the Italian population is no exception. In accordance with the presumably low number of patients, which makes data collection more difficult, especially when promoted by a single centre or small research groups, evidence-based recommendations for diagnosis and therapy are lacking for the vast majority of rare headaches.
In order to overcome the knowledge gap about rare primary headaches, we launched the RegistRare Network in 2017. The RegistRare Network is a collaborative group of Italian tertiary Headache Centres (31) aimed both at collecting epidemiological data about rare headaches and starting and maintaining a disease registry. The present study has kick-started the RegistRare Network research initiatives that, by means of the systematic collection of clinical data about rare headaches, will, on the one hand, increase our knowledge about them and, on the other hand, favour research opportunities in this population.
Here, we report initial findings of the RegistRare Network initiative, emerging from a retrospective survey on specific and overall prevalence and incidence of rare primary headaches (Part One, Chapter 3 and Chapter 4, ICHD-3) in patients referred to Italian tertiary Headache Centres during a 3-year period.
Methods
We performed a retrospective cohort study including patients who, from 1 May 2014 to 30 April 2017, visited seven Italian tertiary Headache Centres. Each participating centre received the approval of the competent Ethics Committee (for the Coordinating Centre, Careggi Hospital Headache Centre, Florence, approval #10976 of the Area Vasta Centro Section of the Tuscany Region Ethics Committee) before commencing any procedures. In each centre, at least two investigators performed a single-blinded review of medical records of patients who had been examined as either a first or a follow-up visit during the study period, in order to identify eligible subjects. Patients were coded in the study through the Italian Health System unique identifier, to avoid duplications of patients that referred to more than one centre. Eligible subjects were those who, in the study period, were registered with a diagnosis of TACs and/or other primary headaches according to the diagnostic criteria detailed in Chapter 3 and Chapter 4 of the Part One of the ICHD-3 (16). Despite its higher prevalence and consequent uncertainty about its definition as a rare headache, we included cluster headache in the present study also because epidemiological data are available for it and we were interested in comparing our findings with previous results. Eligible subjects were informed by phone or during follow-up visits about the study objectives and were asked to give their consent to participate in the study, in accordance with Italian laws (32). Prevalent headache is defined as a headache recorded within the study timeframe, regardless of when the diagnosis was made. Incident headache is defined as a headache diagnosed for the first time in a patient during the study period. It is noteworthy that in some cases the diagnosis may have been delayed in comparison to the onset of the headache, because of the time lag of the patient’s referral to the headache centre. Data about overall and specific prevalence and incidence of TACs or other primary headaches were collected by means of a web-based open source platform (i.e. SurveyMonkey).
According to the aim of the study, no formal sample size calculation has been performed. Data were analysed by descriptive statistics, including proportions and percentages for quantitative and categorical variables. No formal statistical comparison among centres has been performed. In order to estimate prevalence and incidence (specific and overall) of rare primary headache disorders, the population of patients referred to the study centres in the period from 30 April 2014 to 1 May 2017 was considered as the “general population”. Each patient, independent of the number of visits performed during the study period, counted as one, according to her/his diagnosis (prevalent or incident) of a rare headache. For patients who visited more than one centre, in the case of equivalent diagnoses, the diagnosis was attributed to the first centre she/he visited. In case of patients that received more than one diagnosis, regardless of whether the same centre or different centres diagnosed the conditions, each diagnosis counted as one. For analysis purposes, diagnoses of probable other primary headaches (i.e. probable primary cough headache; probable primary exercise headache; probable primary headache associated with sexual activity; probable cold-stimulus headache; probable external-pressure headache; probable external-compression headache; probable external-traction headache; probable primary stabbing headache; probable nummular headache; probable hypnic headache; probable new daily persistent headache) have been grouped as “Probable other primary headaches”.
Results
Seven nationwide distributed tertiary Headache Centres collected data by means of evaluation of paper and/or electronic medical charts or the database used in routine clinical practice according to local procedures. Details about location and characteristics of the centres are reported in Figure 1 and Table 1. According to data available on the internet (see Supplementary materials for details about information search and data retrieval), there are 75 tertiary headache centres in Italy; consequently, the RegistRare retrospective study included 9.3% of them.
Location and size of the centres participating in the RegistRare retrospective survey. The map represents participating centres in Italy, showing their nationwide distribution. Each centre is identified with a different colour and a number, which also identifies the centres in Tables 3 and 4. The area of the circles representing the centres is scaled according to the number of patients visiting each centre in the study period. Characteristics of participating tertiarya Headache Centres. According to the EHF/LTB standard (31).

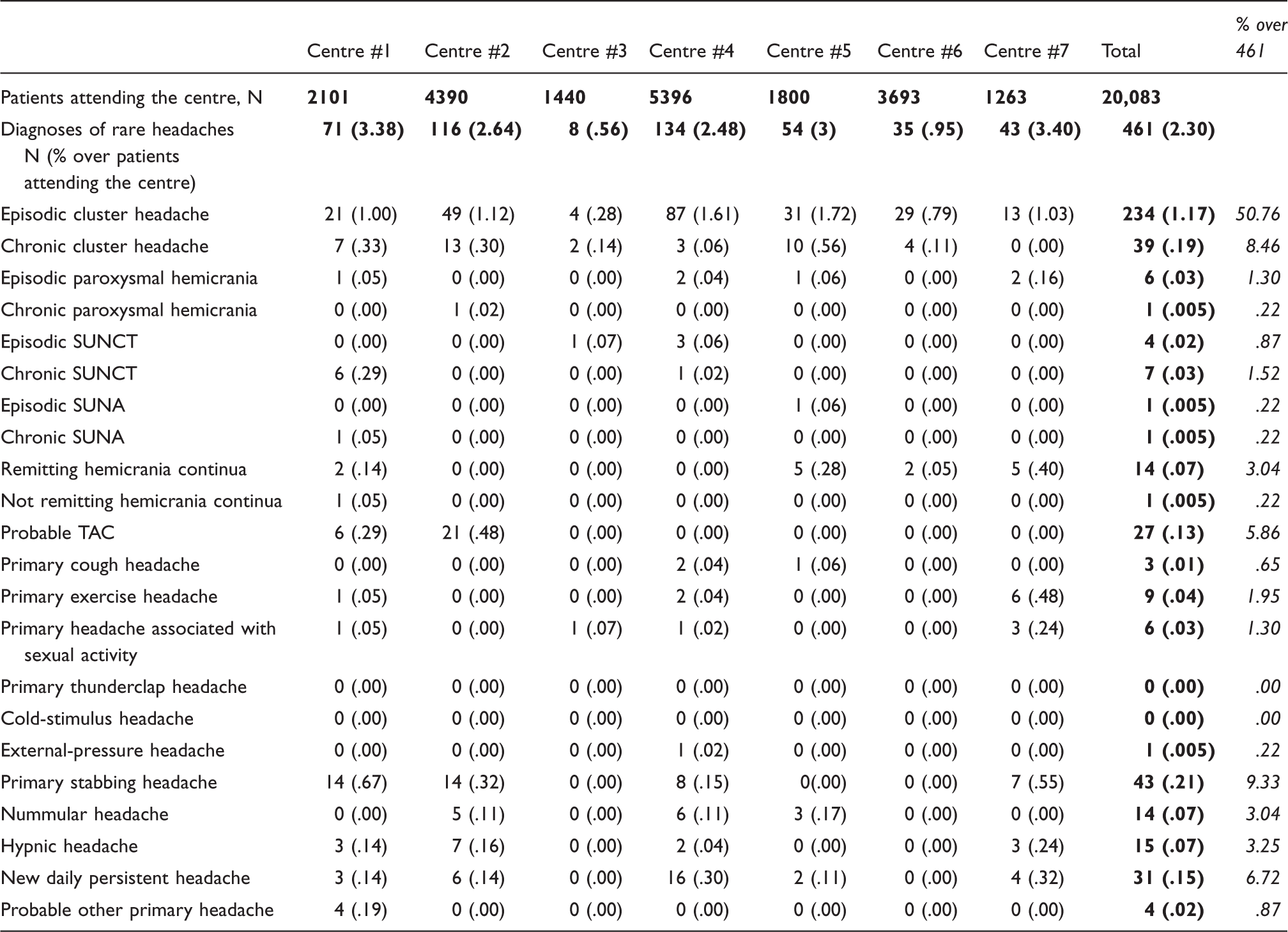
Prevalent diagnoses of rare headaches between 1 May 2014 and 30 April 2017.

Note: In bold the centre population, the total number of rare headache diagnoses for each centre and percentage over centre population (columns) and the total number of patients diagnosed with a rare headache and percentage over the overall study population (rows). In italics the percentage of patients diagnosed with each type rare headache over the overall number of patients diagnosed with rare headaches.
Incident diagnoses of rare headaches between 1 May 2014 and 30 April 2017.
Note: In bold the centre population, the total number of rare headache diagnoses for each centre and percentage over centre population (columns) and the total number of patients diagnosed with a rare headache and percentage over the overall study population (rows). In italics the percentage of patients diagnosed with each type rare headache over the overall number of patients diagnosed with rare headaches.
Prevalence of rare headaches
During the study period, 816 (4.1%) out of 20,083 patients who visited the centres had a past or a new diagnosis of the headaches described in Chapter 3 and Chapter 4 of Part One of the ICHD-3, for a total of 822 diagnoses (six patients had a double diagnosis; for details see Supplementary materials, Table 1). Detailed overall prevalence for each centre is reported in Table 3. Six-hundred and sixty-eight (81.3%) and 154 (18.7%) out of 822 diagnoses were of headaches included in Chapter 3 and Chapter 4 of Part One of the ICHD-3, respectively. Cluster headaches represent by far the most numerous diagnosed conditions, as they accounted for 70.4% of the rare headaches diagnoses (Figure 2, panel (a)).
Distribution of prevalent and incident diagnoses of rare headaches. (a) Distribution of different entities over the 822 prevalent diagnoses of rare headaches. The five most represented conditions are graphed separately; all the remaining conditions are graphed as “Others”. For detailed numerical data see Table 3. (b) Distribution of different entities over the 461 incident diagnoses of rare headaches. The five most represented conditions are graphed separately; all the remaining conditions are graphed as “Others”. For detailed numerical data see Table 4.
Four hundred and eighty-eight (2.4%) out of 20,083 patients visiting the centres had a past or a new diagnosis of episodic cluster headache, while 91 (0.4%) had a past or a new diagnosis of chronic cluster headache. In our population, the ratio of episodic versus chronic cluster headache was 5.36. Among other TACs, the most frequent entities diagnosed were probable TAC (34 diagnoses out of 20,083 patients, 0.2%), SUNCT (chronic: 12 diagnoses, 0.1%; episodic: 10 diagnoses, 0.1%), and hemicrania continua (remitting: 15 diagnoses, 0.07%; not remitting: three diagnoses, 0.02%). Episodic and chronic paroxysmal hemicranias counted only seven (0.03%) and six (0.03%) diagnoses, respectively. Among other primary headaches, primary stabbing headache (50 diagnoses out of 20,083 patients, 0.3%) and new daily persistent headache (44 diagnoses, 0.2%) were the most frequent, as they accounted for 6.1% and 5.4%, respectively, of the rare headaches diagnoses (Figure 2, panel (a)). Hypnic headache and nummular headache follow, accounting for 16 (0.1%) and 15 (0.1%) diagnoses, respectively, of the 20,083 patients that visited the centres during the study period. Notably, for the cold stimulus headache, no cases were registered in any centres during the study period (Table 2).
A certain dishomogeneity has been registered among centres, independent of the number of patients visiting them, for many conditions (Table 2), including: episodic and chronic cluster headache, episodic paroxysmal headache, episodic SUNCT, remitting hemicrania continua, primary headache associated with sexual activity, primary stabbing headache, hypnic headache, new daily persistent headache (Figure 3). Finally, some diagnoses (e.g. probable TAC, external pressure headache) are relatively highly represented only in one or two centres (Table 2).
Prevalence of rare headaches in participating centres. Number of diagnoses for each rare headache in each centre is plotted against the number of patients visiting the same centre in the study period. The area of the circles representing the centres is scaled according to the prevalence of the rare headache in the Centre, in order to highlight the dishomogeneity among centres. Only headaches for which at least one diagnosis has been reported in at least four centres have been plotted. Rare headaches are in order according to the number of diagnoses registered.
Incidence of rare headaches
In the study period, 461 (2.3%) out of 20,083 patients visiting the centres received a new diagnosis of the headaches described in Chapter 3 or Chapter 4 of Part One of the ICHD-3. Detailed overall incidence for each centre is reported in Table 3. Three-hundred and thirty-five (72.7%) and 126 (27.3%) out of 461 diagnoses were of headaches included in Chapter 3 and Chapter 4 of Part One of the ICHD-3, respectively. Similar to prevalence findings, cluster headaches represent by far the most frequently diagnosed condition, as they account for 59.2% of the incident rare headaches (Figure 2, panel (b)). Two hundred and thirty-four (1.2%) out of 20,083 patients visiting the centres received a new diagnosis of episodic cluster headache. Thirty-nine (0.2%) patients received a new diagnosis of chronic cluster headache. Among other TACs, the most frequent incident entities were probable TAC (27 diagnoses out of 20,083 patients, 0.1%) and hemicrania continua (15 diagnoses, 0.1%, of which 14 for remitting hemicrania continua). Number of new diagnoses for paroxysmal hemicranias (episodic, six diagnoses, 0.03%; chronic, one diagnosis, 0.01%), SUNCT (episodic, four diagnoses, 0.02%; chronic, seven diagnoses, 0.03%), and SUNA (episodic, one diagnosis, 0.01%; chronic, one diagnosis, 0.01%) was remarkably low. Not surprisingly, also for other primary headaches, results are superimposable to findings about prevalence: primary stabbing headache (43 diagnoses out of 20,083 patients, 0.2%), new daily persistent headache (31 diagnoses, 0.2%), hypnic headache (15 diagnoses, 0.1%) and nummular headache (14 diagnoses, 0.1%) were the most frequent entities. For primary thunderclap headache and cold stimulus headache no new diagnoses have been registered in any of the centres during the study period (Table 3).
Notably, for many clinical entities, a large portion of diagnoses, though not all, were new diagnoses (Figure 4). Similar to what has been observed for prevalence, for some clinical entities (e.g. chronic SUNCT, probable TAC, primary exercise headache, primary headache associated with sexual activity), a certain dishomogeneity has been registered among centres (Table 3).
Incident diagnoses over prevalent diagnoses of rare headaches. Bars represent the percentage of incident diagnoses over prevalent diagnoses for each rare headache. Headaches for which incident diagnoses represent at least 50% (red line) of prevalent diagnoses are represented by grey bars.
Discussion
Our results shed new light about multiple aspects concerning the epidemiology of rare headaches. The first relevant finding is that, as a whole, headaches described in Chapter 3 and Chapter 4, Part One, of ICHD-3 affect 4.1% of all patients who visited the participating tertiary Headache Centres during the 3-year period. It is noteworthy that the present results are the first showing the burden of rare headaches in clinical practice. Importantly, five clinical entities (i.e. episodic cluster headache, chronic cluster headache, probable TAC, primary stabbing headache, new daily persistent headache) represent 86.0% of the total number of rare headaches (Figure 2, panel (a)). It is likely that the recent diagnostic recognition or reclassification of some clinical entities in comparison to long-standing coded entities (e.g. cluster headache) may have some impact on this result. In addition, the recent release of the ICHD-3 (16) has probably contributed to the presence of a high number of rare headaches with a large portion of incident diagnoses (Figure 4), which for some conditions represent the totality, indeed. Not surprisingly, cluster headache, either episodic or chronic, represented by far the most frequent condition (70.4% of the prevalent rare headaches, Figure 2, panel (a)). Similar to what has been reported in literature (30) in our population, the ratio of episodic versus chronic cluster headache was 5.36. This finding is quite remarkable, as it suggests the representativeness of our population, even if our data cannot be generalized to the general population.
Notably, episodic cluster headache is the only condition for which cases have been registered in all participating centres, while for 13 (chronic paroxysmal hemicrania, chronic SUNCT, episodic SUNA, chronic SUNA, not remitting hemicrania continua, probable TAC, primary cough headache, primary exercise headache, primary thunderclap headache, cold-stimulus headache, external-pressure headache, nummular headache, probable other primary headaches) of the 20 clinical entities encompassed by Chapter 3 and Chapter 4, Part One, of ICHD-3, plus the “probable other primary headaches” category we added, no cases were diagnosed during the study period in more than a half (≥4 out of 7) of the participating centres, independent of the number of patients visiting them (Figure 5). This quite impressive result may have several explanations. First, the population – notwithstanding its size as a whole – was not sufficient to observe any cases of those conditions in most of the centres. If this were to be the case, we could hypothesize that the prevalence of these 13 conditions in the general population is far lower than their prevalence in our population (mean value 0.04%) and, accordingly, it is likely that, even in the future, evidence should preferentially come from single case reports or case series. Second, the candidate headaches have a small burden in the life of patients (e.g. episodic conditions) who, consequently, do not look for medical attention at tertiary centres. If this were to be the case, we should consider performing future studies in the general population or at the general practice level. However, clinical experience with the disability suffered by these patients, even in the case of episodic headaches, discourages this interpretation. Third, the diagnosis has not been made in patients actually affected. Notwithstanding the recent modification of ICHD, missed diagnoses do not seem likely as the centres involved have a high level of expertise in the field of headaches and the diagnostic process is strictly consistent with ICHD. These initial data may contribute to begin reflecting about some entities coded in the ICHD-3 and their relevance in clinical practice.
Rare headaches across participating centres. Bars represent the number of centres where at least one diagnosis has been made for each rare headache. Headaches for which a diagnosis has been registered in less than four centres (50%, red line), are represented by grey bars.
The dishomogeneity in the frequency of some conditions among different centres (Figure 3) may have various explanations. First, it may be attributable to the very low number of patients for some conditions (i.e. episodic SUNCT, primary headache associated with sexual activity, episodic paroxysmal hemicranias), together with the different numbers of patients visiting different centres. Second, because of differences in the Italian health system among various geographical-administrative areas that may affect patient management, some centres may be favoured for some diseases. Third, the dishomogeneity may be due to an increased attractiveness of some centres for patients affected by specific diseases. All these hypotheses may interplay and should be evaluated in a future study looking, for instance, at areas of origin of patients visiting the centres. Importantly, current data show that, in a period of three years, less than a handful of patients moved to different centres.
To the best of our knowledge, there are no other studies or initiatives dealing with rare headaches as a whole and using a nationwide perspective. In addition, it is noteworthy that for headaches listed in Chapter 4 of ICHD-3 there are no other epidemiological data at all, neither for single entities nor the group. The large population and the multicentre nature give us a first, wide-ranging snapshot of the burden of rare headaches in clinical practice, according to the ICHD version in force (Figure 6).
Heat map of rare headaches. (a) Prevalent cases across participating centres, represented by columns and identified by the centre numbers. The intensity of the colour represents the number of diagnoses for each condition, according to the scale above the graph. For detailed numerical data see Table 3. (b) Incident cases across participating centres, represented by columns and identified by the Centre numbers. The intensity of the colour represents the number of diagnoses for each condition, according to the scale above the graph. For detailed numerical data see Table 4.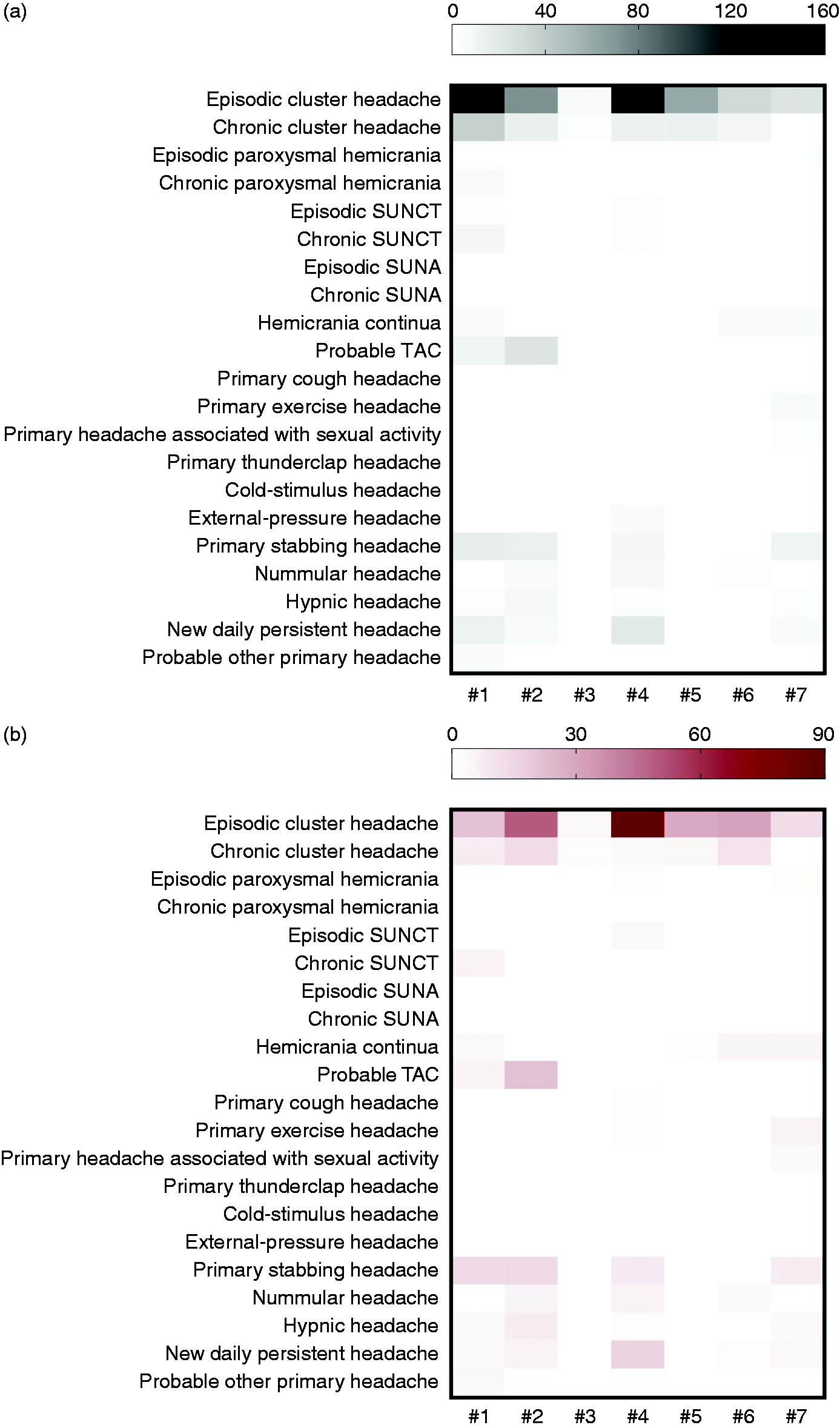
Some limitations affect the study and its findings. According to the retrospective design, the observation (i.e. misclassification) bias was unavoidable. However, according to the nature of data included in the study (i.e. the sole diagnosis), the bias is likely to have scarcely affected the results. It is worth noting that all participating centres have been making their diagnoses with strict observance of the ICHD criteria and that the study period started 1 year after the release of the ICHD-3 beta version (33), which is superimposable to ICHD-3 for Chapters 3 and 4, hence ensuring that the diagnostic criteria had fully entered the clinical practice, and the learning curve for ICHD use had already reached its plateau. Another drawback is represented by the fact that the centres are only a portion of the Italian tertiary Headache Centres. However, some of them are the largest on the national scene. In order to overcome this bias, the involvement of additional centres in the RegistRare Initiative will be strongly promoted and the data updated.
Conclusions
The present findings suggest that, even if with considerable differences among various entities, rare headaches represent a low, but not negligible, portion of patients visiting tertiary headache centres. The RegistRare Network, the first-ever reported nationwide initiative entirely devoted to rare headaches, is expected to have a doubly relevant impact in the field. First, it is the first initiative reporting results of the application of the diagnostic criteria of Part One, Chapter 3 and Chapter 4, of ICHD-3 in clinical practice in a large population. Second, the RegistRare registry will enormously favour observational studies (e.g. aimed at defining clinical characteristics of specific headaches, such as comorbidity with common primary headaches or other conditions), not limited to a single centre or small group of patients and explore – and hopefully boost – the feasibility of controlled clinical trials, which may take advantage of recent therapeutic advancements (i.e. CGRP antibodies) in the headache field (34). The possibility of making the RegistRare Initiative an international venture, as we hope, would change the entire scenario for rare headaches and their management in clinical practice.
Supplemental Material
Supplemental material for Rare primary headaches in Italian tertiary Headache Centres: Three year nationwide retrospective data from the RegistRare Network
Supplemental material for Rare primary headaches in Italian tertiary Headache Centres: Three year nationwide retrospective data from the RegistRare Network by Chiara Lupi, Luana Evangelista, Valentina Favoni, Antonio Granato, Andrea Negro, Lanfranco Pellesi, Raffaele Ornello, Antonio Russo, Sabina Cevoli, Simona Guerzoni and Silvia Benemei in Cephalalgia
Footnotes
Public health relevance
According to retrospective data, 4.1% of patients visiting seven Italian tertiary Headache Centres from 1 May 2014 to 30 April 2017 had a diagnosis of rare headache.
Cluster headache, either chronic or episodic, is by far the most represented condition, being around 70% of the rare headache diagnoses.
For many rare headaches, a large portion of diagnoses, if not their totality, are incident.
For some conditions (i.e. thunderclap headache and cold stimulus headache) no new diagnoses have been registered in any of the centres in the study period, and no diagnoses of cold stimulus headache have been registered.
Acknowledgements
We would like to acknowledge other members of the RegistRare Network: Dr Sara Bottiroli and Dr Roberto De Icco, University of Pavia; Dr Paola Di Fiore, University of Milan; Dr Edoardo Mampreso, Headache Centre, Euganea – Padova Health Unit; Dr Matteo Paolucci and Dr Martina Ulivi, Campus Bio-Medico University, Rome. We would also like to thank Dr Francesco De Cesaris, Careggi Hospital Headache Centre, Florence, for his valuable collaboration and expert advice, Dr Mary Lokken, Florence, for English-language editing, and Dr Cristian Cesarano, for data retrieval at the IRCCS Institute of Neurological Sciences of Bologna, Bologna.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.