
Abstract
Objective
To estimate the risk of miscarriage amongst pregnant women with migraine compared to pregnant women without migraine. To compare the odds of miscarriage in women taking medication for migraine to women with migraine who did not take medication and to explore this association with different types of medications.
Design
Matched cohort study and nested case-control.
Setting
Clinical Practice Research Datalink (CPRD) GOLD pregnancy register. All pregnancies meeting data quality requirements between 2000 and 2019 were eligible for inclusion.
Participants
Cohort study: 193,208 pregnancies of women with migraine were matched one-to-one to women without migraine. Nested case-control: 20,778 pregnancies of women with migraine that ended in miscarriage were matched to 40,122 pregnancies of women with migraine that did not end in miscarriage.
Main outcome measures
Cohort study: miscarriage recorded in primary care. Nested case-control: odds of miscarriage amongst migraineurs using migraine medication.
Results
Miscarriage occurred in 10% (n = 19,233) of women without migraine compared to 10.8% (n = 20,778) of women with migraine. Having migraine was associated with an 8% higher relative risk of miscarriage (risk ratio (RR) 1.08, 95% confidence interval (CI) 1.06–1.10, p < 0.001) and remained significant after adjustment for demographic factors, body mass index (BMI), smoking and comorbidities (aRR 1.06 95% CI [1.04–1.08][p = 0.001]).
Of the pregnancies ending in miscarriage, 719 (3.46%), 380 (1.83%), 173 (0.83%) and 733 (3.52%) were exposed to triptans, amitriptyline, beta-blockers and non-steroidal anti-inflammatory drugs (NSAIDs), respectively. Of the matched pregnancies that did not end in miscarriage, 1099 (2.74%), 542 (1.35%), 294 (0.73%) and 780 (1.94%) were exposed to these medications, respectively.
Exposure to triptans, amitriptyline and NSAIDs were associated with a significantly higher odds of miscarriage (aORs 1.24 [1.11–1.38][p < 0.001], 1.25 [1.08–1.45][p = 0.003] and 1.74 [1.57–1.93][p < 0.001] respectively). Beta-blockers were not associated with a higher risk of miscarriage.
Conclusions
Migraine and triptan, amitriptyline and NSAID exposure were all associated with higher risk of miscarriage. Further work is needed to understand the potential causative mechanisms.
Introduction
Migraine is one of the most common neurological disorders, especially among women of childbearing age with almost 30% experiencing migraine by the age of 45 years (1) meaning approximately 140,000 pregnancies are in women with migraine every year in UK (2–5). In addition to being a major cause of disability (5), migraine is also associated with a higher risk of cardiovascular disease and stroke (6,7), especially in pre-menopausal women (8). Multiple studies have also shown that pregnant women with migraine are at significantly greater risk of developing gestational hypertension and pre-eclampsia (9), supporting the view that migraine is a complex vascular disorder that can also affect systems outside the brain.
The association between migraine and miscarriage remains less clear. Recently, two large electronic health record database studies assessed the association between migraine and miscarriage. Results from a Danish pregnancy cohort study of 228,324 women showed an elevated risk of miscarriage in pregnant women with migraine (adjusted prevalence ratio 1.10 [95% confidence intervals (95% CI): 1.05–1.15]) (10); however, a much smaller, non-significant, association was found between migraine and miscarriage in a Norwegian study of 593,009 pregnant women (adjusted odds ratio 1.02 [95% CI: 0.98–1.05]) (11). These studies are limited by potential under-ascertainment of migraine diagnosis: both reported a prevalence of only 3–3.5% in their cohorts. This has the potential to bias the risk towards the null. A prospective cohort study following up women with migraine who were planning pregnancies showed similar findings to the Norwegian study (hazards ratio 1.03 [95% CI 0.91–1.06]), although this had a relatively low number of participants (n = 7,890) (12).
Common treatments used for migraine in pregnancy include headache-specific therapies such as triptans and other therapies such as non-steroidal anti-inflammatory drugs (NSAIDs), amitriptyline and propranolol (13,14). However, the effects of these treatments during pregnancy on the risk of miscarriage is even less well understood. Berard et al. (15) found an increase in the odds of miscarriage, by almost two thirds, in women taking triptans during pregnancy. However this study did not exclusively include women with migraine, thus overlooking potential confounding by indication (15). Other medications commonly used for migraine, such as non-steroidal anti-inflammatory drugs (NSAIDs), amitriptyline, and beta-blockers, have not been studied specifically in pregnant women with migraine. There are inconsistent findings around the association between NSAIDs and miscarriage; a systematic review and meta-analysis (of 207,341 studies) found a non-significant increased risk (OR = 1.37 95%CI 0.99–1.99) (16). Out of three studies (17–19) investigating the effect of tricyclic antidepressants on pregnancy outcomes, two (17,18) found an increased risk of miscarriage in studies of drugs used in the management of depression. No evidence of an association between beta-blockers and miscarriage has been found.
The aims of this study were to estimate the risk of miscarriage amongst pregnant women with migraine compared to those without and, in those women with migraine whose pregnancies ended in miscarriage, compare the risk of being prescribed common medications for the treatment of migraine to those whose pregnancies did not end in miscarriage.
Methods
Study population
This analysis includes two study designs; 1) a retrospective cohort study of pregnant women with migraine matched to pregnant women without migraine to assess the association of pre-pregnancy migraine with miscarriage; 2) a nested case-control study of pregnant women with migraine to compare the medication intake of those who had a miscarriage to those who did not have a miscarriage.
The Clinical Practice Research Datalink (CPRD) GOLD is an anonymised database of routinely collected primary care health records, which covers 7% of the UK population including almost 1000 GP practices. The database includes patient-level data on demographics (age, ethnicity, and social deprivation), symptoms, diagnoses, prescriptions and laboratory investigation results. Within this, an algorithm has been developed to identify pregnancy episodes, from which a validated pregnancy register has been created (20). This formed the source population for the study.
All women aged between 15 and 50 years with pregnancies that occurred between January 1, 2000, and December 31, 2019, were eligible for inclusion. Eligibility criteria also included 1) having an acceptable patient flag within CPRD GOLD (which indicates sufficient data quality) and 2) a minimum of one year of registration with a practice or one year of registration after the up-to-standard date of the registered practice, whichever was later.
A known issue with the CPRD pregnancy register is the presence of “uncertain” pregnancy episodes where one episode can overlap with another in the same woman, pregnancies with outcomes that are inconsistent with the length of gestation, or where no pregnancy outcome is documented (21). Where pregnancy episodes overlapped, pregnancies with more complete data were selected, whereas pregnancies with an implausible length of gestation were removed so that no overlapping pregnancies remained for the final analysis. The handling of pregnancy episodes with no recorded outcome is described in the statistical methods section.
Exposure and outcome definition for matched cohort study
For the matched cohort, the exposure, migraine, was defined by the presence of a Read code (a hierarchical clinical coding system to document patients’ symptoms, diagnoses and referrals) (22) for diagnosis of migraine or a single prescription of medications used exclusively in the management of migraine in UK practice (triptans, migraine combination treatments (Migraleve, Migravess, Femigraine), or calcitonin gene-related peptide (CGRP inhibitors) at any time prior to the pregnancy start date. For each pregnancy in women with migraine, one pregnancy in a woman without migraine was matched using exact matching for maternal age (±1 year) and year of pregnancy. To minimise misclassification, we excluded women with any recorded history of headaches from the unexposed group to ensure that the unexposed group included women without migraine or related symptoms. Each pregnancy episode within the pregnancy register was assigned an outcome by the algorithm. Miscarriage (the outcome of interest) was identified by the presence of a Read code in the primary care record. The methodology and codelists are described elsewhere (20).
Case definition and exposures for the nested case control study
For the nested case-control study, the pregnant women with migraine formed the source population. Cases were defined as pregnancies where the outcome was recorded as miscarriage in the CPRD pregnancy register. Each pregnancy ending in miscarriage was matched to two pregnancies that did not end in miscarriage. Exact matching was used, matching on maternal age (±1 year) and year of pregnancy. For the cases, the index date was assigned as the date of miscarriage. For controls, the index date was assigned to the date that corresponded to gestational age at the end of the matched case pregnancy. This was to ensure that the same window of exposure was considered for both cases and controls, hence avoiding time-window bias (23).
The exposure variables for the nested case-control study were defined as the presence of a prescription code for triptans, amitriptyline, beta-blockers, or NSAIDs during the exposure window (the period between the pregnancy start date and index date). The codelists for variables used in both studies are available in Online Supplementary Table 1.
Statistical methods
Data related to pregnancy timings and outcomes were obtained from the CPRD pregnancy register (20). Extraction of other demographic, lifestyle, diagnostic and prescription variables was facilitated using the data extraction for epidemiological research (DExtER) tool (24).
Covariates in the analysis included demographic and lifestyle factors derived from patient records. These included age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–50), latest body mass index (BMI) prior to conception (Underweight (<18.5), Normal weight (18.5–<25), Overweight (25–<30), Obese (≥30) and Missing), preconception smoking status (Non-smoker, Ex-smoker, Smoker and Missing), patient level Index of Multiple Deprivation quintiles (IMD;) and ethnicity (white, South Asian, Black, Other and Missing) and comorbidities defined by the presence of Read codes (depression, asthma, type 1 and type 2 diabetes, hypertension, hypothyroidism, hyperthyroidism, inflammatory bowel disease (IBD), endometriosis, systemic lupus erythematosus (SLE), chronic kidney disease (CKD) and polycystic ovary syndrome (PCOS); yes or no). These were derived from reviewing the literature for conditions associated with migraine, miscarriage, or both.
Baseline characteristics were described using appropriate summary statistics, mean and standard deviations for continuous variables, and frequencies and percentages for categorical and binary variables.
For the matched cohort study, log binomial regression was used to generate risk ratios and adjusted risk ratios to describe the relationship between migraine and risk of miscarriage. The model was adjusted for demographics, lifestyle factors and comorbidities. Pregnancies were used as the unit of analysis but as a woman could have multiple pregnancies, statistical inference from the log binomial regression model was based on cluster-robust standard errors to account for similarity of outcomes within a woman. Risk of early miscarriage (at 12 weeks or earlier) was also investigated as a secondary outcome.
For the nested case-control study, logistic regression was used to estimate odds ratios and 95% CI for the association between drugs used in the management of migraine and miscarriage. Drugs for migraine prescribed during the exposure window were examined alone and in combination. The regression model was adjusted for all the covariates and statistical inference from the logistic regression model was based on cluster-robust standard errors to account for similarity of outcomes within a woman. Prescription of drugs for migraine in the year before pregnancy were also included as covariate, as a proxy for disease severity, to mitigate any potential effect that the severity of migraine may have on the risk of miscarriage. The main analysis was repeated excluding pregnancies where the outcome was unknown. In another sensitivity analysis, to investigate the effect of selection bias in the controls, the main analysis was repeated using controls sampled as risk sets, allowing women to serve as controls for multiple cases and allowing women whose pregnancies resulted in miscarriage to serve as controls in the period before their miscarriage.
All analysis was performed in Stata IC version 15 (StataCorp). Two-sided p values < 0.05 were considered to be statistically significant.
Patient and public involvement
The patient and public involvement (PPI) advisory group for the MuM-PreDiCT consortium, a group working across all four nations of the UK studying multiple long-term conditions in pregnancy, were involved in the interpretation of the study findings and will be consulted when producing lay summaries of findings and dissemination of results.
Results
1,526,061 pregnancies in the CPRD pregnancy register that occurred between 2000 to 2019 met data eligibility requirements. Once “uncertain” pregnancy episodes were removed from the dataset, 1,410,329 pregnancies remained, representing 783,811 women. Of these, 147,576 were pregnancies in women with a coded diagnosis of migraine. An additional 45,632 pregnancies were in women who had been prescribed a drug for the exclusive management of migraine. Overall, 193,208 pregnancies were pregnancies of women with migraine, representing 108,897 women (Figure 1).

Study flow diagram.
Baseline characteristics
The distribution of demographic characteristics such as age and IMD were similar between the pregnancies of women with migraine and women without migraine. However, the prevalence of obesity, depression, asthma, hypertension, hypothyroidism, endometriosis and PCOS was higher in the pregnancies of women with migraine (Table 1).
Baseline characteristics for matched cohort of pregnancies according to exposed and unexposed to migraine.

BMI: Body Mass Index, CKD: Chronic Kidney Disease, DM: Diabetes Mellitus, IBD: Inflammatory Bowel Disease, IQR: Interquartile Range, IMD: Index of Multiple Deprivation, PCOS: Polycystic Ovary Syndrome, SLE: Systemic Lupus Erythematosus.
Similarly, the prevalence of obesity, depression, asthma, type 1 and 2 diabetes, hypertension, hypothyroidism, endometriosis and PCOS were higher in women with pregnancies that ended in miscarriage (Table 2).
Baseline characteristics of miscarriage cases and matched controls.

BMI: Body Mass Index, CKD: Chronic Kidney Disease, DM: Diabetes Mellitus, IBD: Inflammatory Bowel Disease, IQR: Interquartile Range, IMD: Index of Multiple Deprivation, PCOS: Polycystic Ovary Syndrome, SLE: Systemic Lupus Erythematosus.
Results of matched cohort
10.8% (20,778/193,208) of pregnancies of women with migraine, regardless of treatment, ended in miscarriage compared to 10.0% in those without migraine (19,233/193,208). Having migraine was associated with an 8% higher relative risk of miscarriage (risk ratio (RR) 1.08, 95% confidence interval (CI) 1.06–1.10, p < 0.001) and remained significant after adjustment for demographic factors, BMI, smoking and comorbidities (aRR 1.06 95% CI [1.04–1.08][p = 0.001]). The adjusted risk ratios were similar when restricting to early miscarriage (aRR 1.06 95% CI [1.04–1.09][p < 0.001]) (Table 3).
Risk ratio (RR) and 95% CI of miscarriage for pregnancies of women with or without migraine.
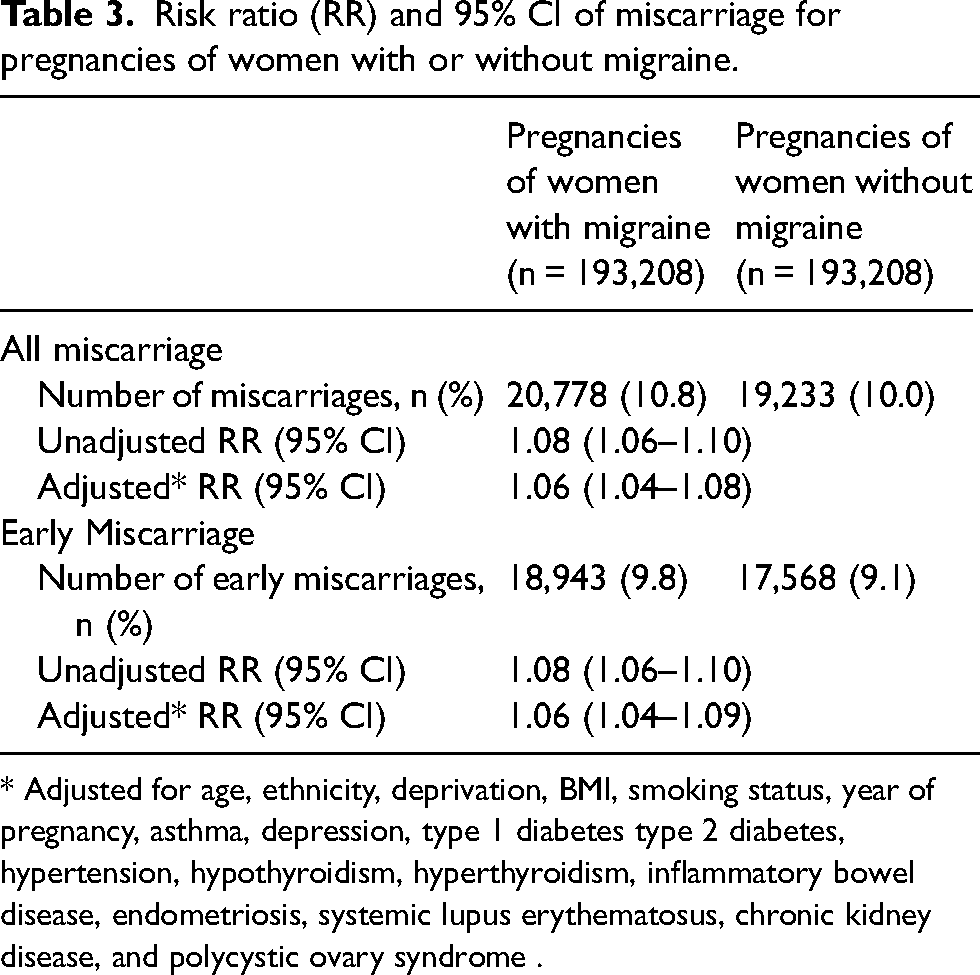
* Adjusted for age, ethnicity, deprivation, BMI, smoking status, year of pregnancy, asthma, depression, type 1 diabetes type 2 diabetes, hypertension, hypothyroidism, hyperthyroidism, inflammatory bowel disease, endometriosis, systemic lupus erythematosus, chronic kidney disease, and polycystic ovary syndrome .
Results of nested case-control
Of the 20,778 pregnancies ending in miscarriage, 719 (3.46%), 380 (1.83%), 173 (0.83%) and 733 (3.52%) were exposed to triptans, amitriptyline, beta-blockers and NSAIDs respectively. Of the 40,122 matched pregnancies that did not end in miscarriage 1099 (2.74%), 542 (1.35%), 294 (0.73%) and 780 (1.94%) were exposed to triptans, amitriptyline, beta-blockers and NSAIDs respectively.
Exposure to triptans, amitriptyline and NSAIDs were associated with a significantly higher odds of miscarriage (aORs 1.23 [1.11–1.37] [p < 0.001], 1.25 [1.08–1.45][p = 0.003] and 1.74 [1.57–1.93] [p < 0.001] respectively). Beta-blockers were not associated with a higher risk of miscarriage (aOR 1.02 [0.82–1.27]) (Table 4).
Odds ratios and 95% CI for miscarriage by type of medication used for migraine.

NSAIDs: Non-steroidal anti-inflammatories, CI: confidence intervals, OR: odds ratios.
* Adjusted for age, ethnicity, deprivation, BMI, smoking status, asthma, depression, year of pregnancy, type 1 diabetes type 2 diabetes, hypertension, hypothyroidism, hyperthyroidism, inflammatory bowel disease, endometriosis, systemic lupus erythematosus, chronic kidney disease, polycystic ovary syndrome and drugs (triptan, amitriptyline, beta-blockers and NSAIDs).
Similar results were seen for the sensitivity analyses for early miscarriage, risk set sample and when removing those with unknown pregnancy outcome (Online Supplementary Tables 2–4).
A higher percentage of pregnancies that ended in miscarriage had individual and combinations of prescriptions during pregnancy compared to pregnancies not ending in miscarriage; triptans (2.9% vs. 2.5%), amitriptyline (1.4% vs. 1.1%) and NSAIDs (3.0% vs. 1.7%) individually, triptans and amitriptyline (0.24 vs. 0.17%), triptans and NSAIDs (0.28 vs. 0.10%), amitriptyline and NSAIDs (0.19 vs. 0.09%) and all three in combination (numbers too small to report). Odds ratios for being prescribed combinations in women with miscarriage versus women without miscarriage were generally higher for combinations of medications than for medications prescribed individually (Figure 2).

Results of logistic regression of association between combinations of medications and miscarriage.
Similar results were seen for the sensitivity analyses for early miscarriage, risk set sample and outcome unknown (Online Supplementary Tables 5–7).
Discussion
Results from the matched cohort study showed a relatively small, but significant higher risk of miscarriage for pregnancies in women with migraine compared to those without. Findings from the nested case control analysis showed that women with migraine whose pregnancies ended in miscarriage had higher odds of having been prescribed triptans, amitriptyline and NSAIDs than women with migraine whose pregnancies did not end in miscarriage. Women whose pregnancies ended in miscarriage also had significantly higher odds of being prescribed triptans and NSAIDs in combination and amitriptyline and NSAIDs in combination.
Strengths and limitations
This study has several strengths. The inclusion of 193,208 women with migraine means this is one of the largest cohort studies to assess the association of pre-pregnancy migraine with risk of miscarriage. We used a validated pregnancy register from a large database that is representative of the UK (20), with patient demographics being comparable to the UK census in terms of age, sex and ethnicity (25). We captured migraine diagnosis using Read codes and prescriptions of drugs used exclusively in the management of migraine. A considerable number of conditions that were known to be more prevalent in patients with migraine or associated with miscarriage were adjusted for in the analysis.
The prevalence of migraine in this study was 13.7%, which is lower than the expected prevalence (∼20%), meaning that a small proportion of the comparator group in the cohort study likely also had migraine. While we excluded women with other headache disorders from the comparator group, some women with unrecorded migraine may have remained, potentially leading to an underestimation of the effect size. On the other hand, it is possible that we have selected women with more severe cases of migraine and, if severity of migraine is associated with an increased risk, the effect size for migraine and miscarriage may have been overestimated. Further to this, the reliance on diagnostic and prescription codes for migraine or migraine therapies, rather than validated criteria such as the International Classification of Headache Disorders (ICHD-3) introduces the possibility of misclassification bias. Some cases coded as migraine may not meet ICHD-3 criteria, and conversely, some true migraine cases may have been missed if not coded. As any misclassification is likely non-differential, this may have attenuated the associations in our analyses. The prevalence of miscarriage in the women eligible for inclusion in this study was 10%, again lower than the expected prevalence (26). This is likely to reflect early miscarriage that occurred before pregnancy was reported to the GP. This potentially means that the results cannot be applied to the risk of early miscarriage. However, it is unlikely there would be a difference in reporting of miscarriage between those with and without migraine or those who were or were not prescribed medications. Although there were a number of pregnancies without a recorded outcome, we took this into consideration by undertaking a sensitivity analysis excluding these pregnancies.
Conducting the case-control analyses in women with migraine will have mitigated any potential confounding by indication. However, it may be that the severity of migraine impacts on the risk of miscarriage and also increased the chance of medication, (and particularly combinations of medications), being prescribed. We attempted to account for this by adjusting for use of these medications in the year prior to pregnancy. However, there may still have been residual confounding. Data were not available for prior history of miscarriages, paternal age and alcohol intake which are known to be related to miscarriage. As alcohol is a common migraine trigger, it may be that the migraine population have a lower consumption. Not being able to adjust for alcohol in the analysis may have led to an underestimation of the risk ratio. It may also have been useful to consider the impact of the presence of aura on miscarriage, particularly as migraine with aura is associated with a higher vascular risk than migraine without aura (27) but only a small proportion of women with migraine had aura coded in the structured data. Reverse causality, whereby triptans or NSAIDs are taken in response to a miscarriage-associated migraine or miscarriage associated pain, must also be considered as a possible explanation. In addition, the decline in oestrogen associated with miscarriage (28) could be a potential trigger for a migraine episode (29). Although the results were adjusted for a number of comorbidities, residual confounding may still be present and could contribute to the observed increased risk of miscarriage in this group of women.
As only prescription data were considered in this analysis, this only indicates that a prescription was issued and not dispensed (or taken) resulting in an over- or underestimation of these associations with miscarriage. We were also unable to determine the frequency of use of medications. In addition to this, over the counter medication was not captured in this analysis. As some NSAIDs and triptans are available over the counter in the UK, this may have had a particular effect on these analyses, although it is likely that a pharmacist would recommend a pregnant woman with headaches consult her GP. If, however, NSAIDs were purchased over the counter, this, again, may lead to an under or overestimation of the association with miscarriage. Newer medications, such as CGRP inhibitors, were not prescribed in sufficient numbers during pregnancy to analyse their effects. In addition, due to geographic variation in GP practice participation in CPRD (with Scotland and Wales being over-represented in the GOLD dataset), the dataset may not be geographically representative (25). There may be variations in prescribing practices across the four nations, meaning the rates of prescriptions seen in this study may not be representative of the UK overall.
Findings in the context of other literature
Our findings of an association between migraine and miscarriage are in agreement with those of a Danish pregnancy cohort study which found an adjusted prevalence ratio of 1.10 (1.05–1.15) (10). While a Norwegian registry linkage study by Magnus et al. showed a small nonsignificant association (aOR 1.02 [0.98–1.05]) (11), this might be because of the low prevalence of migraine (3.14%), which is likely to be an under-ascertainment, meaning that their comparator population also included women with migraine. In a prospective cohort study of pregnancy planners, Crowe et al. found a non-significant association of a similar magnitude between migraine and miscarriage (HR 1.03 [0.91–1.06]) (12). This study included 1683 pregnant women with migraine, a much smaller cohort than our study and the other registry-based studies. This study relied on self-reported migraine diagnosis, which has the advantage of capturing cases that have not presented to health services. On the other hand, they did not use validated criteria to confirm the diagnosis, so it is possible that other headache disorders were misclassified as migraine, potentially diluting the results. It is worth noting that, as around a third to a half of pregnancies are unplanned (30,31), this cohort may not be representative of pregnant women in general. Taken together with the results from our studies, the totality of evidence would suggest a slightly higher risk of miscarriage in women with migraine.
The effect size of the association between triptans and miscarriage is comparable to those of a meta-analysis by Marchenko et al. (32), with results showing a pooled OR of 1.27 (95% CI 0.58–2.79) when comparing triptan exposed women with migraine controls. This was based on the results of two small studies which included 360 women, which may account for the wide confidence intervals. Results from a nested case-control in a Canadian pregnancy register published since this meta-analysis, showed that, in comparison to healthy controls, women exposed to triptans during pregnancy had higher odds of miscarriage (aOR: 1.63 [95% CI 1.34–1.98]). To account for indication bias, the authors of this study adjusted for migraine diagnosis during pregnancy or in the year prior to pregnancy in their analysis, meaning their migraine prevalence was around 2%. In addition, dispensed triptans were considered as the exposure, which will perhaps better reflect medication that was taken than prescribed medication (15).
No previous studies have considered amitriptyline treatment and its impact on miscarriage. Two studies have found a significant higher risk of miscarriage in patients with depression. One found an increased risk in disease-matched controls (RRR 1.3 [1.1–1.5]) (17) and the other found an increased risk in comparison to patients without depression (RR 1.47 [1.28–1.70]) (18), but this did not remain significant when the analysis was restricted to women with depression. Another study did not find any significant association (19). It is worth noting that the tricyclic dosage for the management of depression is higher than the dosage used in the management of pain such as that used for migraine prophylaxis.
A meta-analysis of the impact of NSAID exposure on the risk of miscarriage pooled the results of ten studies and shower a higher risk that was not statistically significant (OR 1.37 [0.99–1.88]). However, there was a significantly higher risk of miscarriage for NSAIDs when the analysis was restricted to studies where NSAIDs were taken around the time of conception (2.32 [1.16–4.66]) (16).
Biological plausibility
The potential vascular effects of migraine and drugs used to treat migraine should be considered, especially in relation to utero-placental perfusion.
Migraine is characterised by endothelial dysfunction, which may explain the increased risk of cardiovascular disease and stroke in patients with migraine (6,7). Endothelial dysfunction within the placenta has been suggested as one of the underlying causes of both miscarriage and pre-eclampsia (33). The well-established link between migraine and pre-eclampsia would appear to support this hypothesis (9).
Triptans are contraindicated in patients with cardiovascular disease and ischaemic stroke due to their serotoninergic vasoconstrictive properties (34). Miscarriage secondary to utero-placental hypoperfusion has been postulated with frequent triptan use (35). The serotoninergic effect of triptans, through their binding to 5HT receptors, has been suggested as a potential causal mechanism (32). A serotonergic mechanism has also been hypothesised to be involved in miscarriage (36). Some tricyclic antidepressants, in particular amitriptyline, have a serotonin inhibition effect, which may also explain the link between amitriptyline and miscarriage found in this study (15).
Although it is widely accepted that NSAIDs are contraindicated in late pregnancy (> 30 weeks) (37), due to premature closure of the ductus arteriosus, they are widely prescribed in early pregnancy (13,38). Inhibition of prostaglandin synthesis by NSAIDs may also cause utero-placental hypoperfusion and miscarriage secondary to mal-implantation in early pregnancy (19,39–41).
Implications for research and practice
Previous studies have found associations between migraine and other pregnancy complications, such as preterm birth (10) and low birth weight (9). It is less clear what, if any, impact medications have on these outcomes. There has been some suggestion of an association between triptans and low birth weight (42), whereas conflicting results have been found in studies of the impact of triptans on preterm birth, with both an association (43) and protective effect (42) being reported. Further research on the impacts of migraine medications on other pregnancy outcomes is warranted. This information is vital for women and clinicians to make informed decisions about care during pregnancy.
Much evidence around medications in pregnancy comes from observational studies which have associated limitations and biases. This lack of robust evidence, alongside the legacy of tragedies such as thalidomide (44), has led to a precautionary, “better safe than sorry”, approach to prescribing during pregnancy (45). Recently, there have been calls for more nuanced discussions of risk during pregnancy (45,46). An approach that supports shared decision making with women is warranted, for example through the use of decision aids (47).
Conclusion
In this large cohort study and nested case-control analysis, migraine and its treatment with triptans, NSAIDs and amitriptyline were found to be associated with a higher risk of miscarriage. Although measures were taken to account for the potential impact of severity of migraine on the risk miscarriage, the effects of confounding by indication and potential for reverse causality must be considered when interpreting the results of this study. Further work is needed to understand the potential causative mechanisms.
Dissemination to participants and related patient and public communities
We plan to disseminate these research findings to relevant stakeholders by presenting our findings at relevant conferences, through our PPI channels and by engaging with the media through press releases.
Clinical implications
This study adds weight to the evidence that migraine and associated triptan, amitriptyline and NSAID exposure is associated with a higher risk of miscarriage.
This is the first study to examine the association between NSAIDs, amitriptyline and miscarriage specifically in women with migraine.
The potential impact of confounding by indication and reverse causality must be considered when applying the results of this study to clinical practice.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251414634 - Supplemental material for Migraine, associated treatments and risk of miscarriage: A matched cohort study and nested case-control study using the CPRD pregnancy register
Supplemental material, sj-docx-1-cep-10.1177_03331024251414634 for Migraine, associated treatments and risk of miscarriage: A matched cohort study and nested case-control study using the CPRD pregnancy register by Katherine Phillips, Krishna Gokhale, Christine Damase-Michel, Helen Dolk, Catherine Nelson-Piercy, Benjamin R Wakerley, Francesca Crowe and Krishnarajah Nirantharakumar in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024251414634 - Supplemental material for Migraine, associated treatments and risk of miscarriage: A matched cohort study and nested case-control study using the CPRD pregnancy register
Supplemental material, sj-docx-2-cep-10.1177_03331024251414634 for Migraine, associated treatments and risk of miscarriage: A matched cohort study and nested case-control study using the CPRD pregnancy register by Katherine Phillips, Krishna Gokhale, Christine Damase-Michel, Helen Dolk, Catherine Nelson-Piercy, Benjamin R Wakerley, Francesca Crowe and Krishnarajah Nirantharakumar in Cephalalgia
Footnotes
Acknowledgments
We would like to thank the patient and public involvement representatives for the MuMPreDiCT group for their input to this study.
Author contributions
K.P., K.N., F.C. and B.R.W. conceived the study, designed the initial analysis and defined definitions for exposures, covariates and outcomes. K.P. and K.G. undertook the analysis and all authors contributed to interpretation of an improvements to the analysis. K.P. drafted the manuscript and led the revision process. All authors critically reviewed the manuscript, approved the final version of the manuscript and agree to be accountable for all aspects of the work. K.N. is the guarantor for this work.
Data availability statement
The data that support the findings of this study are available from CPRD but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
CPRD has ethics approval from the Health Research Authority to support research using anonymised patient data. The study has been approved by the Independent Scientific Advisory Committee for CPRD (reference: 22_001790)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was not specifically funded but was supported by the MuMPreDiCT consortium which is funded by the Strategic Priority Fund “Tackling multimorbidity at scale” programme (grant number MR/W014432/1) delivered by the Medical Research Council and the National Institute for Health Research (NIHR) in partnership with the Economic and Social Research Council and in collaboration with the Engineering and Physical Sciences Research Council. KP, NIHR Clinical Lecturer, is funded by the NIHR for this research project. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, National Health Service (NHS) or the UK Department of Health and Social Care.
This work was also supported by Health Data Research UK (HDRUK2023.0030), which is funded by UK Research and Innovation, the Medical Research Council, the British Heart Foundation, Cancer Research UK, the National Institute for Health and Care Research, the Economic and Social Research Council, the Engineering and Physical Sciences Research Council, Health and Care Research Wales, Health and Social Care Research and Development Division (Public Health Agency, Northern Ireland), Chief Scientist Office of the Scottish Government Health and Social Care Directorates.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.