
Abstract
Background
Migraine is common in reproductive aged women. Understanding the impact of migraine and associated treatments on pregnancy outcomes remains very important. An umbrella review of systematic reviews, with or without meta-analyses, examined the link between migraine and pregnancy outcomes.
Methods
We systematically searched Medline, Embase and Cochrane to 27 October 2022. Quality appraisal was carried out using the AMSTAR2 tool. An established framework was used to determine whether included reviews were eligible for update.
Results
Four studies met review criteria. Migraine was reported to be associated with increased odds ratio (OR) of pre-eclampsia, low birth weight and peripartum mental illness (pooled OR = 3.54 (2.24–5.59)). Triptan-exposed women had increased odds of miscarriage compared to women without migraine (pooled OR = 3.54 (2.24–5.59)). In updated meta-analyses, migraine was associated with an increased odds of pre-eclampsia and preterm birth (pooled OR = 2.05 (1.47–2.84) and 1.26 (1.21–1.32) respectively).
Conclusions
Migraine is associated with increased odds of pre-eclampsia, peripartum mental illness and preterm birth. Further investigation of the relationship between migraine and placental abruption, low birth weight and small for gestational age is warranted, as well as the relationship between migraine, triptans and miscarriage risk.
Introduction
Migraine is the second most common primary headache disorder after tension-type headache and is estimated to affect about one in seven people worldwide. Migraine is two to three times more prevalent in women of childbearing age, with almost 30% experiencing migraine by the age of 45 years (1). Migraine is the leading cause of disability amongst people under the age of 50 years and contributes 45.1 million years lived with disability to the global disease burden, with 20.3 million of these in women aged between 15 and 49 years (2). People with migraine report a negative impact on their education, employment, family relationships and leisure activities (3).
Migraine is not a benign headache disorder and there is a well-established association between migraine and cardiovascular disease risk (4,5). Although many women report improvement or remission of migraine during pregnancy (6), as a result of its high prevalence in women of reproductive age, the impact of migraine and its treatment on pregnancy outcomes have been a key focus in recent literature. A 2019 meta-analysis found that migraine was associated with a significantly increased risk of pre-eclampsia and low birth weight (7). A subsequent large cohort study of a Danish population registry also found an increased risk of pregnancy-associated hypertension disorders, miscarriage, preterm birth and caesarean section (8). The findings of this study and other newer studies may alter the effect estimates reported in existing reviews.
Migraine often requires pharmacological therapies to alleviate symptoms and prevent attacks, some of which are contra-indicated in pregnancy. Recommended treatment options during pregnancy include paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs) (prior to the third trimester) or triptans for symptom relief and aspirin, beta blockers and amitriptyline for migraine prophylaxis (9). However, even for these medications, there is a paucity of evidence regarding their safety in pregnancy, meaning that it is advised they are used with caution (10,11). Despite this, medication use and polypharmacy are prevalent in pregnant women with migraine. A US study of an insurance claims found that around 15% received a triptan in the first trimester and preventative medication use ranged from 10 to 16% (12). A systematic review studying the treatments provided in migraine and associated adverse pregnancy outcomes found no increased risk when comparing with migraine who took triptans during pregnancy to women with migraine who did not take triptans, but insufficient evidence to evaluate the safety of other drugs, such as beta blockers and amitriptyline, used in the management of migraines (13).
Aura is present in approximately 30% of patients and manifests as transient focal neurological symptoms, which usually present as visual disturbances or, less commonly, sensory disturbance or weakness (1). Migraine with aura, has been associated with greater increased risk of ischaemic heart disease and stroke than migraine alone (4,5,14). It is not clear what impact the presence of aura has on pregnancy outcomes.
The present study aimed to review and synthesise existing evidence on outcomes of pregnancies of women with migraine, including in those treated and untreated and those with and without aura. The objectives were to identify and appraise higher level evidence (systematic reviews with or without meta-analyses) reporting on the association between migraine and pregnancy outcomes, to consolidate evidence from systematic reviews and meta-analyses using narrative synthesis and, where appropriate, quantitative synthesis, and to update existing systematic reviews and meta-analyses.
Methods
An umbrella review of systematic reviews with or without meta-analyses of the association between migraine and pregnancy outcomes was performed.
Population, outcomes and comparator
The population included all women, irrespective of age and setting, who were included in observational studies reporting on migraine and pregnancy outcomes. Exposures considered were (i) migraine; (ii) pharmacological therapy for the management of migraine (including medications used exclusively in the management of migraine and those with other indications, provided they were studied in the migraine population); and (iii) migraine with aura. Comparators were (i) women without migraine; (ii) women with migraine not managed with pharmacological therapy; and (iii) migraine without aura.
Outcome
The outcomes of interest were derived from our literature review from an ongoing study for developing core outcome set for pregnancies with multiple long term conditions (15) (supplementary Table 1).
Search methods
Searches were conducted in Medline, Embase and the Cochrane database of systematic reviews from inception to 15 November 2023. No restrictions were applied to language or setting when selecting the studies. The search strategy combined subject headings and free text keywords for migraine, pregnancy and pregnancy outcomes (supplementary Section 1). The search was limited to systematic reviews and meta-analyses.
Eligibility criteria
Systematic reviews and meta-analyses were included. A study was considered to be a systematic review if it met the following criteria: (i) it described the methodology used in adequate detail; (ii) a systematic approach was used to identify all relevant primary studies; and (iii) it performed quality appraisal of included studies (16). The following types of publications were not included: protocols, review articles, conference abstracts, guidelines, consensus, documents or expert position papers, summaries, comments, letters and brief reports.
Study selection and data extraction
After removing duplicate studies, two reviewers independently conducted the title and abstract screening and ineligible studies were excluded. Full text screening of eligible studies was conducted by two reviewers (KP and CCO) independently and a third senior reviewer (FLC) was consulted to resolve any discrepancy.
The list of excluded studies was maintained with the reasons for exclusion documented.
The details of the steps involved in study selection was reported using a PRISMA (i.e. Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart.
A standardised data extraction form was used by KP and data extracted from the studies were checked by second researcher (CCO). In the case of a conflict, a third reviewer was consulted (FLC). Data extracted included: author, year of publication, review aim, databases searched, time period, population, exposures, comparators, outcomes, covariates, study designs, exposure/outcome definition, data synthesis method, quality assessment tool, number of qualitative/quantitative analyses, results of meta-analysis and authors conclusion.
Quality assessment
The AMSTAR 2 tool was used to assess the methodological quality (17). The online AMSTAR 2 (A Measurement Tool to Assess systematic Reviews) was completed by two reviewers independently. Out of the 16 points the AMSTAR 2 tool, one point was awarded for each of the criteria met. As per the AMSTAR guidance, the following domains were considered critical weaknesses; protocol registered before review, adequacy of literature search, justification for excluding individual studies, risk of bias from individual studies included in the review, appropriateness of meta-analytical methods, consideration of risk of bias when interpreting results, assessment of presence and likely impact of publication bias. The reviews were rated as high quality (none or one non-critical weakness), moderate quality (more than one non-critical weakness), low quality (one critical flaw with or without non-critical weakness) or critically low quality (more than one critical flaw, with or without non-critical weaknesses). To resolve any disagreements a third reviewer was consulted.
Overlapping reviews
Reviews were considered to overlap if they evaluated the same outcomes and possibly included the same primary studies. In the case of overlapping, the degree of overlap was presented graphically using a citation matrix which mapped systematic reviews against primary studies. Overlap was quantified using corrected covered area (CCA). Overlap was rated as slight (0–5), moderate (6–10), high (11–15) and very high (>15) (18). In the case of high or very high overlap, one review was selected for inclusion. This was based on the following criteria: AMSTAR rating, year of publication, whether meta-analyses are reported and the number of participants.
Update of existing reviews
An established framework was used to determine whether included reviews were eligible for update. The following criteria was applied:
The key search terms from the review’s search strategy identified new studies which met the review inclusion criteria. The findings of the new studies would have potentially changed the conclusion of the review.
Only high and moderate quality systematic reviews were eligible for update.
Data analysis
Results from reviews were synthesised in narrative synthesis. Study characteristics were presented in a table. Where adjusted and unadjusted risk estimates were available, both were extracted. The findings were presented in forest plots which were created in Stata Statistical Software, Release 17 (StataCorp LLC, College Station, TX, USA).
Results
The database search yielded 291 articles. Following duplicate removal and title and abstract screening, 17 full text articles were assessed for eligibility. Following full text screening, four reviews were found to be eligible, two of which compared pregnancy outcomes between women with and without migraine (7,19) and two of which compared pregnancy outcomes between treated and untreated women with migraine (13,20) (supplementary Figure 1). The reasons for exclusion of full text articles are given in supplementary Table 2. No reviews reported on the association of aura with pregnancy outcomes. The characteristics of included studies are summarised in Table 1 (see also supplementary Table 3).
Characteristics of systematic reviews included in this umbrella review of migraine and pregnancy complications.

Abbreviations: BMI, body mass index, RCT, randomised controlled trial.
Methodological quality
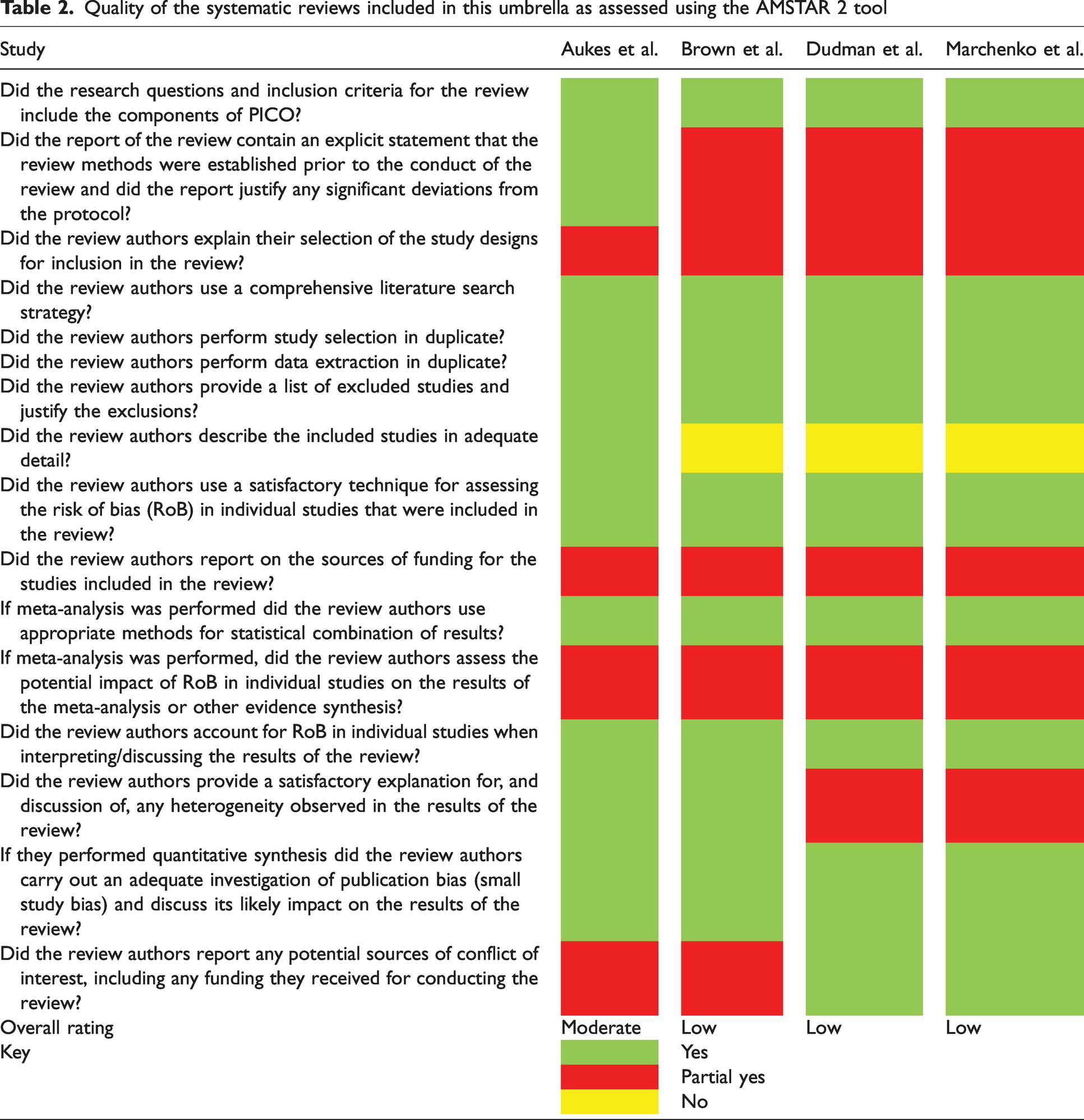
One study by Aukes et al. (7) was rated as moderate and three were rated as low quality. Brown et al. (19), Dudman et al. (13) and Marchenko et al. (20) were all rated as low quality because they were found to have critical weaknesses that included absence of an explicit statement that the review methods were established prior to the conduct of the review. Dudman et al. (13) did not assess publication bias and Marchenko et al. (20) did not account for risk of bias when interpreting results (Table 2).
Quality of the systematic reviews included in this umbrella as assessed using the AMSTAR 2 tool
Overlapping reviews
When considering overlap of reviews, both Dudman et al. (13) and Marchenko et al. (20) reviewed the effects of triptans on preterm birth and included overlapping studies (CCA 50%). According to the criteria, Dudman et al. (13) would have been included as it is the most recent. However, Dudman et al. (13) only performed meta-analysis on studies comparing patients exposed to triptan with the general population. As Marchenko et al. (20) compared triptan exposed patients with migraine control patients, both studies were included.
Eligibility for updates
Because only moderate or high-quality reviews could be considered eligible for update, Aukes et al. (7) was the only review that met this criterion. We were aware of large primary studies that had been published since Aukes et al. (7) conducted their search, which reported results that may change the outcome of the meta-analyses. Therefore, a scoping search was performed to identify relevant studies that had been published since the systematic review. We found five studies that met the eligibility criteria, three of which also reported a significantly higher odds of preterm birth. Aukes et al. (7) therefore met the criteria for an update.
Update to Aukes et al. (7)
A detailed description of the results of the search, screening, quality assessment, data extraction and more detailed results are available in supplementary Section 2.
Findings of included and updated studies
The findings from included and updated studies are summarised in Figure 1 (see also supplementary Figure 2).
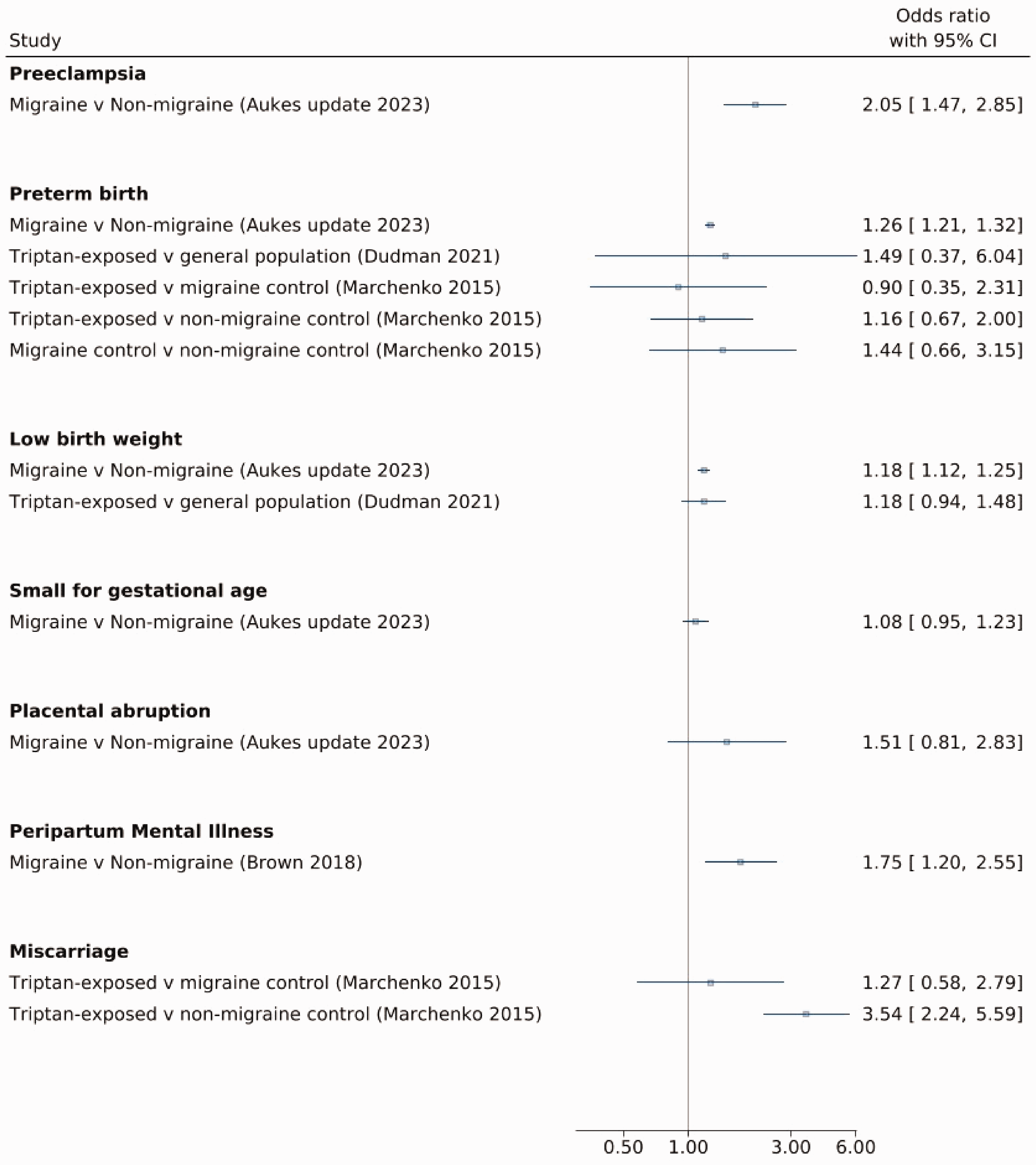
Forest plot of the odds ratios (95% confidence intervals) for associations between migraine, migraine treatments and pregnancy outcomes (umbrella review and update).
Pre-eclampsia
Aukes et al. found women with migraine were at increased odds of pre-eclampsia (pooled odds ratio (OR) = 2.07; 95% confidence interval (CI) = 1.37–2.76) compared to women without migraine (7).
The updated search found an additional six peer-reviewed studies and one abstract. In total, fourteen studies investigating a total of 1,415,249 women, reported on the association between migraine and preeclampsia. The updated meta-analysis found women with migraine had more than twice the odds of pre-eclampsia (pooled unadjusted OR = 2.05 (1.47–2.84)). The pooled OR was also statistically significantly higher for migraine for studies that included adjustment for confounding (pooled adjusted OR (aOR) = 2.22 (1.34–3.68)) (Figure 2a).

(a) Forest plot of random effects meta-analysis of unadjusted and adjusted odds ratios for preeclampsia in women with and without migraine (updated meta-analysis). (b) Forest plot for random effects meta-analysis of unadjusted odds ratios of preterm birth in women with and without migraine (updated meta-analysis). (c) Forest plot for random effects meta-analysis of unadjusted and adjusted odds ratios of placental abruption in women with and without migraine (updated meta-analysis). (d) Forest plot for random effects meta-analysis of unadjusted and adjusted odds ratios of low birth weight in women with and without migraine (updated meta-analysis) and (e) Forest plot for random effects meta-analysis of unadjusted and adjusted odds ratios of small for gestational age in women with and without migraine (updated meta-analysis).
Assuming a baseline risk of 46 cases per 1000 pregnancies (21), migraine is associated with an additional 44 cases of pre-eclampsia per 1000 (95% CI = 20–77 cases per 1000).
The ORs remained significant in sensitivity analyses, which restricted the meta-analysis to prospective cohorts and case–control studies and when abstracts were included in the meta-analysis. A meta-analysis of studies reporting adjusted risk ratios also found a significantly increased risk of pre-eclampsia. Only one study at low risk of bias reported adjusted odds ratios and this found a non-significantly increase in the odds of pre-eclampsia, although the pooled adjusted odds ratios for studies at low risk of bias remained significant (supplementary Figure 3).
There were sufficient studies to construct a funnel plot. Visual inspection of the plot indicated potential publication bias (supplementary Figure 4).
Preterm birth
Aukes et al. (7) found no significant association between migraine and preterm birth when the OR from five studies, including a total of 72,394 women, were pooled (1.23 (95% CI = 0.97–1.55)). However, when the results of two studies that reported aOR were pooled, migraine was associated with 25% increased odds of preterm birth (95% CI = 1.13–1.38).
From the updated search, six further studies were found of which four were peer reviewed and two were abstracts. In the updated meta-analysis, the pooled results of the nine studies, including a total of 364,079 women, found that; compared to women without migraine, women with migraine had a 26% higher odds of pre-term birth with a pooled OR = 1.26 (1.21–1.32). Three studies also reported adjusted OR (pooled aOR = 1.32 (1.15–1.51)) (Figure 2b).
Assuming a baseline risk of 99 per 1000 pregnancies (22), migraine is associated with an additional 23 cases of preterm birth per 1000 (95% CI = 19–28 cases per 1000).
The ORs remained significant in sensitivity analyses which restricted inclusion to the studies with low risk of bias and prospective cohort studies and in a meta-analysis which included abstracts (supplementary Figure 5). There were sufficient studies to construct a funnel plot. Visual inspection of the plot again indicated potential publication bias (supplementary Figure 6).
Placental abruption
Aukes et al. (7) retrieved only one study reporting on placental abruption, which found a more than twofold increase in the risk (aOR = 2.14 (95% CI = 1.22–3.75)).
In the updated search, two further studies were found of which one was an article published in a peer reviewed journal and one was an abstract. The two studies that were included in the meta-analysis included a total of 251,908 women. The odds of placental abruption were more than 50% higher in women with migraine, but this was not statistically significant (OR = 1.51 (0.81–2.84)) (Figure 2c). When the abstract was included, the odds of placental abruption was more than one third higher in women with migraine, which was statistically significant (OR = 1.35 (1.05–1.75)) (supplementary Figure 7).
Low birth weight
Aukes et al. (7) found that maternal migraine was associated with an increased odds of low birth weight (significant in unadjusted analysis only: pooled OR = 1.18 (95% CI = 1.03–1.34), three studies, n = 38,300; pooled aOR = 1.27 (95% CI = 0.89–1.82), two studies, n = 30,151).
Two further studies was found in the updated review. A total of five studies, investigating a total of 350,020 women reported on the association between migraine and low birth weight. In the updated meta-analysis, the odds of low birth weight was 18% higher for women with migraine; pooled unadjusted OR = 1.18 (1.11–1.24). The odds of low birth weight were higher in two studies that reported an adjusted OR, but this was not statistically significant; pooled aOR = 1.27 (0.89–1.82) (Figure 2d).
Assuming a baseline risk of 146 per 1000 pregnancies (23), migraine is associated with an additional 22 cases of low birth weight per 1000 (95% CI = 13–29 cases per 1000).
Small for gestational age
Aukes et al. (7) found, when pooling the results of two studies, that maternal migraine was not significantly associated with an increased odds of small for gestational age babies. Pooled OR = 1.06 (0.98–1.15) and aOR = 1.06 (0.99–1.14).
A further three studies were found in the updated review. A total of five studies investigating a total of 291,279 women, reported on the association between migraine and small for gestational age. In the updated meta-analysis, there was a slightly higher risk of small for gestational age in the unadjusted analysis but this was not statistically significant; pooled unadjusted OR = of 1.08 (0.95–1.23). For the studies that provided aOR, the pooled aOR was 8% higher, a result that was statistically significant; aOR = 1.08 (1.01–1.15) (Figure 2e). The pooled unadjusted OR was not significant in sensitivity analyses of the two articles published in peer reviewed journals only or at low risk of bias only (four studies) (supplementary Figure 8).
Peripartum mental illness
Brown et al. (19) found, when pooling the results of two studies, that maternal migraine was associated with increased odds of peripartum mental illness (OR = 1.75 (1.20–2.54)).
Migraine medications and pregnancy outcomes
Migraine medication and miscarriage
With regards to pregnancy outcomes in women treated with migraine medication, triptans were the only medication that were assessed in a meta-analysis. Marchenko et al. (20) found triptans were associated with more than three times the odds of miscarriage for women treated with triptans compared to healthy controls (pooled OR = 3.54 (2.24–5.59), two studies, n = 51,043). However, there was no significant association of triptans for migraine during pregnancy compared to women with migraine who were not exposed to triptans in pregnancy (pooled OR = 1.27 (0.58–2.79), two studies, n = 260).
Dudman et al. (13) only compared women treated with triptans to the general population in their meta-analysis. They did, however, report pooled prevalences of pregnancy outcomes in women with migraine comparing those who did and did not receive treatment in pregnancy. In agreement with Marchenko et al. (20), this review did not find a significant difference in the prevalence of miscarriage associated with triptan use (8.2% (95% CI = 6.1–10.6%) in those receiving no medication versus 10.2% (95% CI = 5.3–16.1%) receiving triptans). There was, however, a higher prevalence of miscarriage in patients receiving NSAIDs (22.6% (95% CI = 20.7–24.9%)).
Migraine medication and preterm birth
Marchenko et al. (20) found triptans were not significantly associated with risk of preterm birth in comparison to both untreated migraine controls (pooled OR = 0.9 (0.35–2.30) and healthy controls (pooled OR = 1.16 (0.67–1.99)). Dudman et al. (13), on the other hand, reported a significantly lower prevalence of preterm birth in women receiving triptans compared to those not receiving medications (6.6% (5.6–7.7%) versus 10.4% (8.9–12%)).
Discussion
Summary of findings
In this umbrella review of systematic reviews, women with migraine had a higher odds of pre-eclampsia, low birth weight and peripartum mental illness. Women exposed to triptans had a higher odds of miscarriage compared to healthy controls, but not in comparison with women with migraine who were not exposed to triptans in pregnancy (it is worth noting there were low numbers of subjects in the included studies, which likely led to wide confidence intervals for the pooled odds ratio).
This updated systematic review showed that women with migraine had a higher odds of preterm birth. When the results of non-peer reviewed abstracts were included, an association between migraine and placental abruption was also found. It confirmed the finding that there is an association between migraine and pre-eclampsia. In keeping with Aukes et al. (7), a small significant association between migraine and low birth weight was found when unadjusted odds ratios were pooled. By contrast to Aukes et al. (7), the updated meta-analysis found an association between migraine and small for gestational age when adjusted odds ratios were pooled.
Strengths and limitations
This review has several strengths. A predefined protocol was used, and a comprehensive search of multiple databases was conducted. Studies were screened, selected and quality assessed by two independent reviews. Data extraction was checked by an independent reviewer. The update to one review meant we were able to gain more clarity around association with some pregnancy related outcomes.
However, there are also some limitations to the study. First, most of the reviews were of low to moderate quality. As the primary studies that were included were observational, we are limited in our ability to make conclusions about causality. In the meta-analyses, there was high heterogeneity between studies for some of the outcomes including preterm birth and pre-eclampsia. Additionally, asymmetry was observed in the funnel plots of the results of studies for pre-eclampsia and preterm birth, suggesting potential publication bias. Some important outcomes, such as miscarriage, have not been included in systematic reviews, so were not considered in this study.
In the updated review, migraine prevalence varied depending on method by which authors identified diagnosis of migraine. Studies that used self-report found a prevalence of 17–19%, which is similar to the prevalence found in the Global Burden of Diseases study (2). Studies that relied on coding of diagnosis of migraine in electronic health records tended to report a lower prevalence of migraine (7.8–11%). Overall, it is possible that migraine diagnoses were under ascertained, but it is not clear what the impact this may have had on the effect estimates. Including women with migraine in the unexposed groups may have led to an underestimate of the impact of migraine on pregnancy complications. On the other hand, because these studies mostly relied on coding within secondary care (with one also using prescriptions for migraine medication) it may be that only the most severe migraine cases were captured, as less severe cases can be self-managed or managed in primary care. It is unclear from the studies found in this review what, if any, impact severity of migraine has on the risk of complications. However, if more severe migraine is associated with an increased risk, this may have led to an overestimate of the effect. Many of the included studies did not consider whether migraine was active at the time of pregnancy, or whether symptoms resolved during pregnancy (24). One study included by Aukes et al. (7) found a 13-fold increase in the risk of pregnancy-induced hypertension in those whose headache worsened compared to those who resolved (25). However, this study was based on small numbers of cases and relied on a retrospective recall of headache during pregnancy. Because headache is also a symptom of pregnancy-induced hypertension, reverse causality cannot be ruled out.
It should be noted that many of the medications used in the management of migraine (including amitriptyline and beta blockers) have other indications. There may be reviews and studies of the pregnancy outcomes associated with these medications that were conducted outside of the migraine population. These were beyond the scope of this review but may provide insight into their safety in pregnancy.
Some studies used prescription of medications as part of their definition of migraine, and, as found by Dudman et al. (13), there is a lack of evidence around the safety outcomes for most migraine medications. It is therefore unclear whether migraine treatment, and not the underlying disease, could be contributing to some of the outcomes found.
Biological plausibility
Migraine is a complex polygenic neurovascular disorder. There are well established associations between migraine and increased risk of cardiovascular disease and stroke. Women of childbearing age with migraine and aura are at increased risk of stroke and advised to avoid oestrogen-containing contraception, which further increases the risk (26). Potential biological mechanisms underlying this association include; increased burden of cardiovascular risk factors (such as hypertension) in women with migraine, endothelial dysfunction and hypercoagulability (4,5). Migraine has also been found to be associated with a pro-inflammatory state, with raised C-reactive protein found in some patients with the condition. It is hypothesised that sterile inflammation of the cerebral vessels may contribute to cerebral atherosclerosis and stroke (27). A similar pathophysiology is hypothesised to underlie the effect of migraine on the placenta, which may lead to pregnancy complications. A pro-inflammatory state has been found in pregnancies affected by pre-eclampsia (28) and preterm birth (29). Endothelial dysfunction and hypercoagulability have also been found in pregnancies effected by pre-eclampsia (30–32).
Marchenko et al. (20) concluded that the association between triptans and miscarriage is biologically plausible due to the serotonergic, vasoconstrictive properties of triptans (20). Miscarriage as a result of utero-placental hypoperfusion has been suggested with frequent triptan use (33). However, because the association was only significant when comparing triptan-exposed women to healthy controls, the association of triptans and miscarriage could be due to an association between migraine and miscarriage, which has been previously reported (8). Endothelial dysfunction in the placenta has been implicated in miscarriage and may, again, account for this association (34).
The higher prevalence of miscarriage in patients taking NSAIDs found by Dudman et al. (13) is in keeping with a previous meta-analysis (not restricted to the migraine population) which reported a more than twofold higher risk of miscarriage when NSAIDs were taken around the time of conception (35). A suggested mechanism for this is the inhibition of prostaglandin synthesis by NSAIDs may cause utero-placental hypoperfusion and miscarriage secondary to mal-implantation in early pregnancy (36–38).
Implications for future research and practice
Evidence for associations between migraine, low birth weight and small for gestational age remains unclear and therefore more studies examining the relationship between migraine and, preterm birth, small for gestational age and low birth weight are required. The stronger association between migraine and preterm delivery may be the main reason for babies being low birth weight; however, because migraine was associated with small for gestational age (albeit non-significantly), we cannot rule out the possibility of an association between migraine and fetal growth restriction.
It may be that more severe cases of migraine, or migraine that does not improve or worsens in pregnancy may have a stronger association with miscarriage. These women will be more likely to take triptans during pregnancy, leading to an apparent association between triptans and miscarriage. Further investigation of this potential confounding by indication is necessary, as is further investigation of the safety of other drugs used in the treatment of migraine, particularly NSAIDs.
The lower prevalence of preterm birth in women who took triptans during pregnancy compared to those who did not also warrants further investigation. Studies examining this association have found conflicting results (39,40).
No systematic reviews were found which examined the impact of migraine with aura on pregnancy outcomes. Because aura is associated with an increased risk of stroke (5), it is possible that aura will also increase the risk of pregnancy complications. Features such as aura or migraine related to the menstrual cycle have been found to affect whether migraine resolves during pregnancy (41). This is therefore an important area to focus on in future.
Conclusions
There is strong evidence to suggest that women with migraine have a higher risk of pre-eclampsia, preterm birth and peripartum mental illness. Further investigation of the relationship between migraine and placental abruption, preterm birth, low birth weight and small for gestational age is warranted, as well as the relationship between migraine, triptans and risk of miscarriage. There is a lack of information about the safety of other medications used for the treatment of migraine in pregnancy.
Clinical implications
Existing reviews have described an association between migraine, pre-eclampsia and peripartum mental illness. Our updated systematic review and meta-analysis found further evidence of an association between migraine, preterm birth and placental abruption. Further investigation of the relationship between migraine and preterm birth, low birth weight and small for gestational age and between migraine, triptans and risk of miscarriage is warranted.
Supplemental Material
sj-jpg-1-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-1-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-2-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-2-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-3-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-3-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-4-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-4-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-5-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-5-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-6-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-6-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-7-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-7-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-8-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-8-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-9-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-9-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-10-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-10-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-pdf-11-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-pdf-11-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-pdf-12-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-pdf-12-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-pdf-13-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-pdf-13-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-pdf-14-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-pdf-14-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-pdf-15-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-pdf-15-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-pdf-16-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-pdf-16-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-17-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-17-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Supplemental Material
sj-jpg-18-cep-10.1177_03331024241229410 - Supplemental material for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis
Supplemental material, sj-jpg-18-cep-10.1177_03331024241229410 for How migraine and its associated treatment impact on pregnancy outcomes: Umbrella review with updated systematic review and meta-analysis by Katherine Phillips, Conor Clerkin-Oliver, Krishnarajah Nirantharakumar, Francesca L Crowe and Benjamin R Wakerley in Cephalalgia
Footnotes
Author contributions
All authors were involved in the conception and design of this work. KP conducted the searches. KP and CCO selected studies, extracted relevant information and performed quality appraisal. FLC was consulted as a third reviewer when discrepancies arose. KP synthesised the data. All authors were involved in the drafting of the manuscript. KP is the guarantor of this review.
Declaration of conflicting interests
Benjamin R. Wakerley is founder of Ceftronics Limited.
Funding
This project was not specifically funded.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.