
Abstract
Background
Although guidelines for clinical trials have proposed a definition for a migraine day, randomised clinical trials tend to vary in their definition used.
Methods
Definitions of a migraine day in phase III trials with monoclonal antibodies and small molecules targeting the calcitonin gene-related peptide pathway for the preventive treatment of migraine were compared.
Results
Twelve different definitions were found across 23 trials. Variation in headache duration, the inclusion or exclusion of probable migraine and the inclusion or exclusion of a treated migraine attack with a specific or non-specific drug were most subject to debate. No single criterium or set of criteria was common to all definitions used. The most common single criterium used was a minimal headache duration of at least 30 minutes where only two clinical trials allowed for a headache with a shorter duration to be included.
Conclusion
There is a pressing need for a standardised accepted definition of a migraine day both from a clinical and research perspective.
This is a visual representation of the abstract.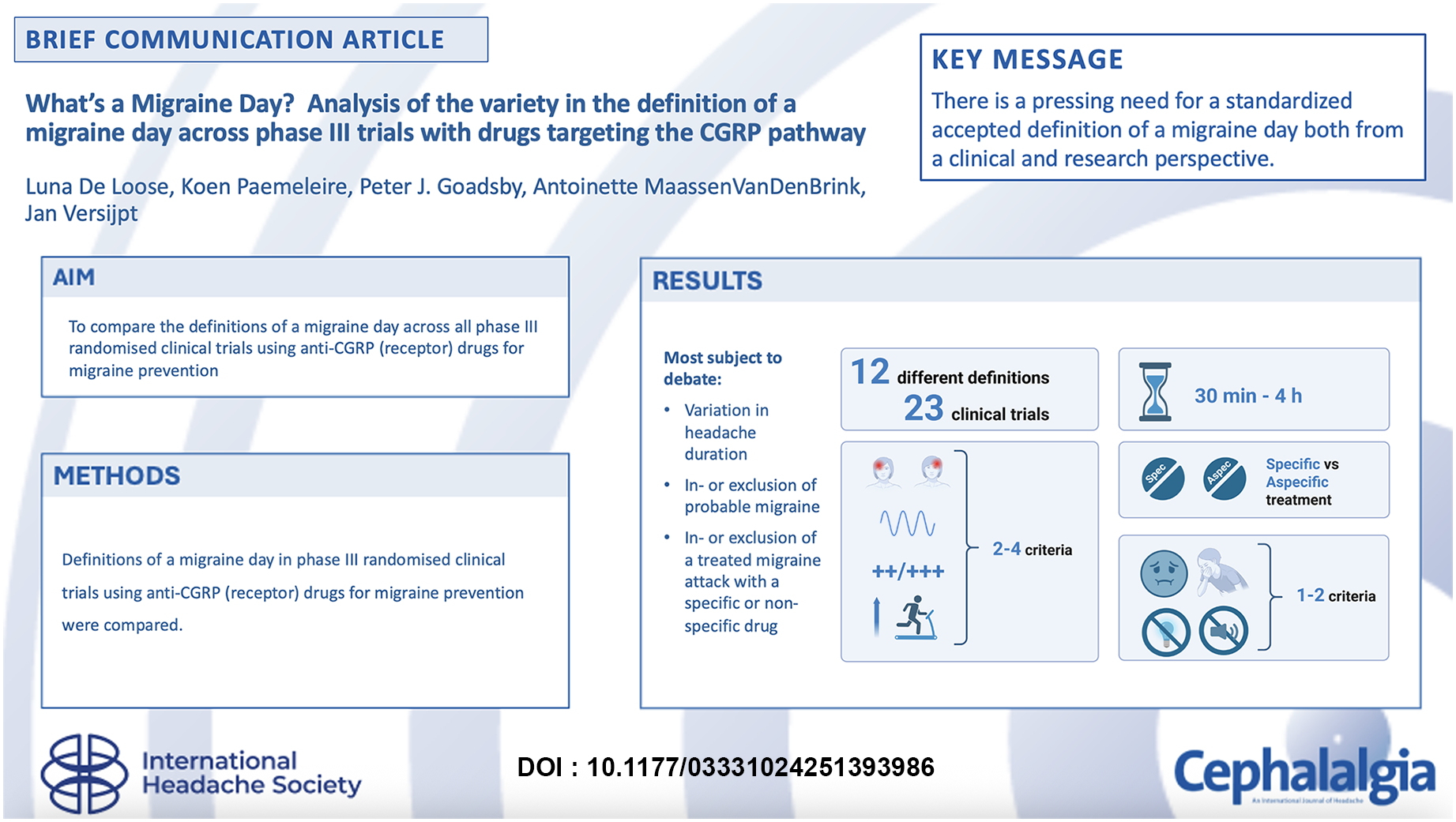
Introduction
Migraine is a primary headache disorder that is three times more common in women than in men, often first appearing in puberty or early adulthood (1). Its one-year prevalence is 14–15%; however, this number is likely to be an under-estimate (2). Formal criteria for the diagnosis of migraine – both with or without aura – are defined by the International Classification of Headache Disorders (ICHD) from the Headache Classification Committee of the International Headache Society (IHS) (Table 1). Its first edition (ICHD-1) was published in 1988 (3), and the third and most recent edition dates from 2018 (4). The fourth edition is currently in progress (5). Diagnostic criteria for chronic migraine appeared in the ICHD-2 in 2004 (6) and were subsequently refined in 2006 and formally incorporated into the ICHD-3b in 2013 (7). One of the items of these criteria refers to “a headache believed by the patient to be migraine and relieved by migraine-specific medication”. This criterion entails a subjective aspect and excludes patients who are relieved with non-migraine specific analgesics like anti-inflammatory drugs.
Diagnostic criteria for migraine, defined by the International Classification of Headache Disorders (ICHD)-3 (4).

Although criteria for a migraine diagnosis are well known and accepted, no established universally accepted criteria exist for a migraine day in a known person with migraine. There have been proposals for a definition of a migraine day by the International Headache Society in the guidelines for controlled trials for, respectively episodic migraine in 2020 (8) and for chronic migraine in 2018 (9) (Table 2). Noteworthy is the difference in duration of the headache episode in these two definitions, the inclusion of probable migraine days and the consideration that only the response to a migraine-specific medication is accepted to label a headache day as a migraine day. Others have examined various attack lengths to define a migraine day to avoid reliance on specific (notably triptan) treatments (10).
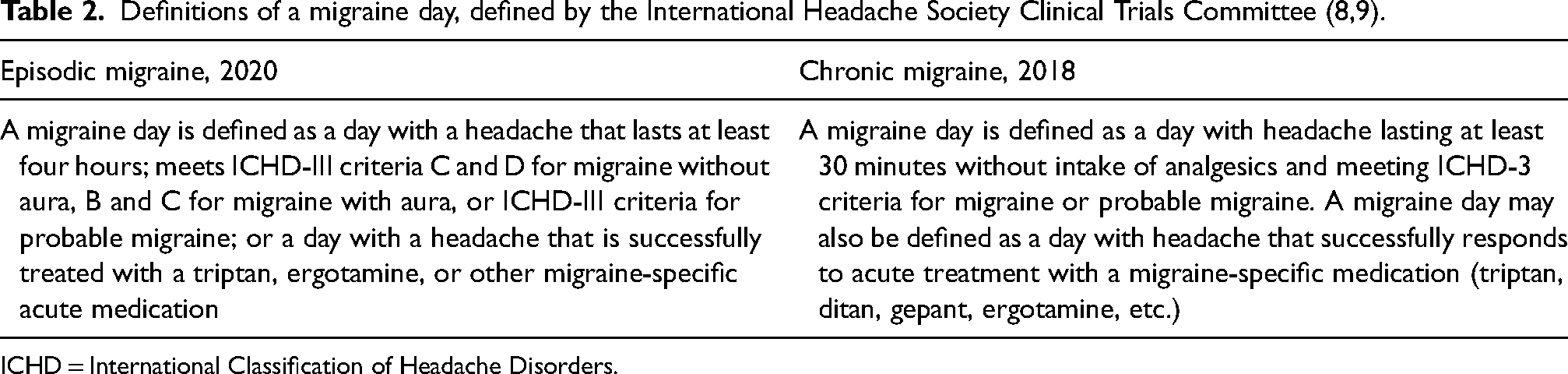
ICHD = International Classification of Headache Disorders.
The present study aimed to compare the protocol definitions of a migraine day across all phase III randomised clinical trials using monoclonal antibodies and small molecules targeting the calcitonin gene-related peptide (CGRP) pathway for migraine prevention.
Methods
A database search on clinicaltrials.gov was performed using the following terms: TEV-48125 or fremanezumab, LY2951742 or galcanezumab, ALD403 or eptinezumab, AMG334 or erenumab, BHV-3000 or rimegepant, and MK-8031 or atogepant. Only phase III trials in adults with a randomised parallel group, double-blinded, placebo-controlled design studying the efficacy of an agent in monotherapy of which the full article was available in English, published until 2024, were considered.
These trials either concerned episodic migraine, chronic migraine or “difficult-to-treat” migraine. Difficult-to-treat migraine was defined as patients with episodic migraine (11,12) or chronic migraine(13–15) who had documented failure to two-to-four classes of migraine preventive medications. The definition of a migraine day was retrieved from either the study protocol or the full-length article.
Results
Twenty-three trials in episodic, chronic or difficult-to-treat migraine were included. Overall, 12 different definitions were found (11–33). The results for every trial grouped per study drug are displayed in Table 3. Within one group of trials with the same drug up to three different definitions were used. No single criterium or set of criteria was common to all definitions used. Below the most relevant differences are summarised.
Duration
Three different minimal headache durations were used, ranging from 30 minutes to four hours. Within one group of trials with the same drug, different durations were used as well (11,13,16–23). Even within one trial, more specifically the DELIVER study, a minimal duration of four hours was required for migraine without aura, but only a minimal duration of 30 minutes was required for migraine with aura (14). Only two clinical trials allowed for a headache with a shorter duration than 30 minutes to be included (24,28).
Headache characteristics and/or associated symptoms
Differences across trials were found concerning the necessity to meet both criteria C and D for migraine without aura (Table 1). In all erenumab and rimegepant trials, meeting only one of C or D was sufficient to label a headache day as a migraine day (11,16–19,30). All atogepant trials consistently used the same definition, which was different from trials with other drugs. Noteworthy is their protocol-specific definition of a probable migraine day where either one criterion of the headache characteristics had to be met ànd one additional criterion of associated symptoms (either nausea and/or vomiting, photophobia and phonophobia or typical aura) or two criteria of headache characteristics without associated symptoms nor aura. In both cases, the headache had to last at least two hours (12,31–33).
Treatment inclusions
In the erenumab, fremanezumab, galcanezumab (chronic migraine only), rimegepant and atogepant trials, a headache day was counted as a migraine day if the patient took a migraine-specific acute drug such as a triptan or ergot alkaloid, regardless of the duration of the headache (11–13,16–23,29–33). A minority of these trials stated that even the presence of a headache was not required when the patient took a migraine-specific acute drug (11,16,18,19,30). In case of the DRAGON study, the previous two definitions of a migraine day were even applied after intake of non-migraine specific acute drugs (19). Amongst the eptinezumab trials, the PROMISE-2 trial required a minimal headache duration of 30 minutes before non-specific or specific acute medication could be taken into account to label a headache day as a migraine day (25). In the DELIVER trial, this same minimal duration of 30 min was accepted but only for migraine-specific drugs (14).
Discussion
Although all CGRP-based monoclonal antibody and small molecule trials used the reduction in monthly migraine days as the primary or secondary endpoint, an extensive heterogeneity in the used definition of a migraine day was found, hampering a formal comparison. This heterogeneity is particularly striking because more than half of these trials were performed after the corresponding guidelines for clinical trials were published by the IHS (Table 3) (8,9). Additionally, the implementation of a uniform definition for a migraine day in digital headache diaries would be beneficial from a clinical perspective for both treating physicians and patients allowing for an automated and uniform treatment evaluation.
A summary of the definition of a migraine day across 23 phase 3 trials targeting the CGRP pathway.

EM=episodic migraine; CM=chronic migraine; DTT=difficult to treat migraine. (1) Probable migraine as defined by the ICHD-3: a headache that meets all but one criterion (4). (2) A protocol-specific definition of a probable migraine day was used (see main text) (12,31–33).
As for headache duration, if untreated, a minimal duration of four hours is required according to the ICHD-3 criteria (Table 1) (4). This could already be debated since earlier epidemiological studies demonstrated that 20–30% of people with migraine are known to have migraine attacks with a shorter duration (34,35). Of note, it is widely accepted that children and adolescents need only a two hour duration to meet migraine criteria (4). If treated, a substantial number of trials did not require a minimal headache duration to label a headache day as a migraine day. It could be argued that a minimal duration is, however, reasonable, given the pharmacokinetics of analgesics and triptans – when administered orally – requiring one hour at a minimum to reach peak plasma concentration (36). A previous study comparing migraine days based on longitudinal E-diary data found that, when headache episodes did not last four hours, although fulfilling both headache features and accompanying symptoms for migraine, 98% of the episodes still had a headache duration of ≥ 30 minutes (10).
According to the ICHD-3 criteria for migraine with aura, it is not mandatory to even have a headache accompanying the aura (Table 1) (4). However, it is important to emphasise that, both in trials conducted to test the efficacy of a prophylactic agent and in clinical practice, the overall aim is typically to reduce the headache and not the aura burden.
The difference in allowing acute treatment with specific versus non-specific drugs to label a headache day as a migraine day is notable. Overall, non-specific drugs such as non-steroidal anti-inflammatory drugs are more available to patients and more widely used than specific drugs such as triptans, gepants or ditans. Furthermore, few studies have directly compared specific and non-specific treatments with the notable exception of some anti-inflammatory drugs like naproxen and sumatriptan (37) and meloxicam and rizatriptan (38,39). Excluding patients or migraine episodes who are relieved with non-specific drugs to label their headache days as migraine days excludes a large number of headache treated migraine patients and leads to an underestimation of the amount of migraine days. On the other hand, the use of this exception might reassure regulators and Health Technology Agencies that the headache days counted are indeed true migraine days.
Lastly, looking at the criteria for probable migraine defined by ICHD-3, probable migraine is a headache that meets all but one criterion for a migraine with (A-C) or without (A-D) aura (4). Therefore, trials that include days with probable migraine into the calculation of the difference in migraine days as a primary endpoint are probably more at risk for bias. This indeed could lead to a confusion between different primary headache disorders. More specifically, the differential diagnosis between a probable migraine day and a day with tension-type headache becomes marginal, although according to the classification rules, a definite diagnosis always trumps a probable diagnosis (4). Currently, no biomarkers exist for either migraine or tension-type headache, complicating sensitivity or specificity calculations for any operational definition. One might consider adopting the definition of a migraine day that yields the greatest difference between active treatment and placebo in prevention trials involving migraine-specific drugs, such as the CGRP pathway inhibitors. However, this empirical strategy may lack mechanistic validity because the effect of this drug class on non-migraine headaches has not been studied extensively and therefore risks being overly pragmatic. Another consideration could be to clarify better the definition of tension-type headache by using the appendix criteria that more robustly demarcates the disorder (4). Importantly, patients included in migraine prevention trials have all been clinically diagnosed with migraine and therefore bear a substantial migraine burden. This ensures that, even when probable migraine days are included in outcome measures, this population reflects individuals with clinically significant migraine symptoms. Hence, while definitional overlap with tension-type headache may introduce some bias, the overall burden of disease in these patients remains clear. This is also in line with the current IHS recommendation stating that in patients who already have a migraine diagnosis, and where the issue is to count the number of attacks they are having (e.g. as an outcome measure in a drug trial), attacks fulfilling criteria for probable migraine should be counted as migraine (4). Future refinement of definitions should balance diagnostic precision while at the same time maintaining the representativeness of the desired patient population.
While we observed considerable heterogeneity in the definitions of a migraine day, our study does not provide data on how this variability affects trial outcomes, since this would require raw study data. The previously mentioned E-diary study found that a single definitional change (i.e. reducing the minimum headache duration from at least four hours to ≥30 minutes) could lead to an increase of 5.4% in monthly migraine days (10). While this indicates that definitional changes may affect trial outcomes, the clinical significance of such changes remains to be determined. Future research could explore how differing definitions impact efficacy estimates, placebo responses and drug effect sizes across trials.
Conclusion
A standardised internationally accepted definition of a migraine day in people with migraine is mandatory both from a clinical and research perspective.
A substantial variety exists in definitions used for a migraine day, even in recent large robust clinical trials. There is a pressing need for a standardised accepted definition of a migraine day, both from a clinical and research perspective.
Footnotes
Author contributions
LDL wrote the first draft of the article. All authors contributed to the literature search, writing of the review, creation of tables and revision in response to (internal) review. All authors approved the final version of the manuscript submitted for publication.
Declaration of conflicting interests
JV received personal fees and non-financial support from Teva, Pfizer and Medtronic, personal fees from Novartis and Lundbeck, and grants and non-financial support from Allergan/AbbVie.
KP received personal fees from Allergan/AbbVie, Eli Lilly, Lundbeck, Man & Science, Novartis, Pfizer and Teva as a speaker and/or advisory board member.
PJG reports, over the last 36 months, personal fees for consulting from Aeon Biopharma, Abbvie, Aurene, CoolTech LLC, Dr Reddy's, Eli-Lilly and Company, Epalex, Ipsen, Kallyope, Linpharma, Lundbeck, Orion Pharma, Pfizer, PureTech Health LLC, Satsuma, Shiratronics, Teva Pharmaceuticals, and Vial; personal fees for advice through Gerson Lehrman Group, Guidepoint, SAI Med Partners and Vector Metric; fees for educational materials from CME Outfitters and WebMD; and publishing royalties or fees from Massachusetts Medical Society, Oxford University Press, UptoDate and Wolters Kluwer.
AMvdB received research grants and/or consultation fees from AbbVie, Amgen/Novartis, Eli Lilly, Lundbeck, Manistee, Pfizer, Satsuma, Teva and Tonix.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.