
Abstract
Background
Higher socioeconomic status (SES) among people with migraine has been associated with an increased use of triptans, but it is undetermined whether high SES is also associated with dispensation of monoclonal antibodies against calcitonin gene-related peptide (CGRPi), a prophylactic treatment against migraine episodes. Our hypothesis was that higher SES is associated with CGRPi dispensation, although the association is expected to be attenuated in a country that generally allows for reimbursement of CGRPi costs.
Methods
In this register-based nested case-control study, the association between SES, categorized into three levels (low, middle and high) and the outcome of a first dispensation of a CGRPi was assessed among people with a migraine diagnosis in Region Stockholm, using univariable and multivariable logistic regression models.
Results
Of 52,996 individuals in the study population, 3.2% (n = 1674) were dispensed CGRPi. Individuals with high or middle SES had an increased probability of being dispensed CGRPi, compared to individuals with low SES (adjusted odds ratio = 1.68; 95% confidence interval = 1.46–1.92 and adjusted odds ratio = 1.41; 95% confidence interval = 1.24–1.61, respectively).
Conclusions
Higher SES was associated with dispensation of CGRPi, which suggests unequal access to CGRPi.
This is a visual representation of the abstract.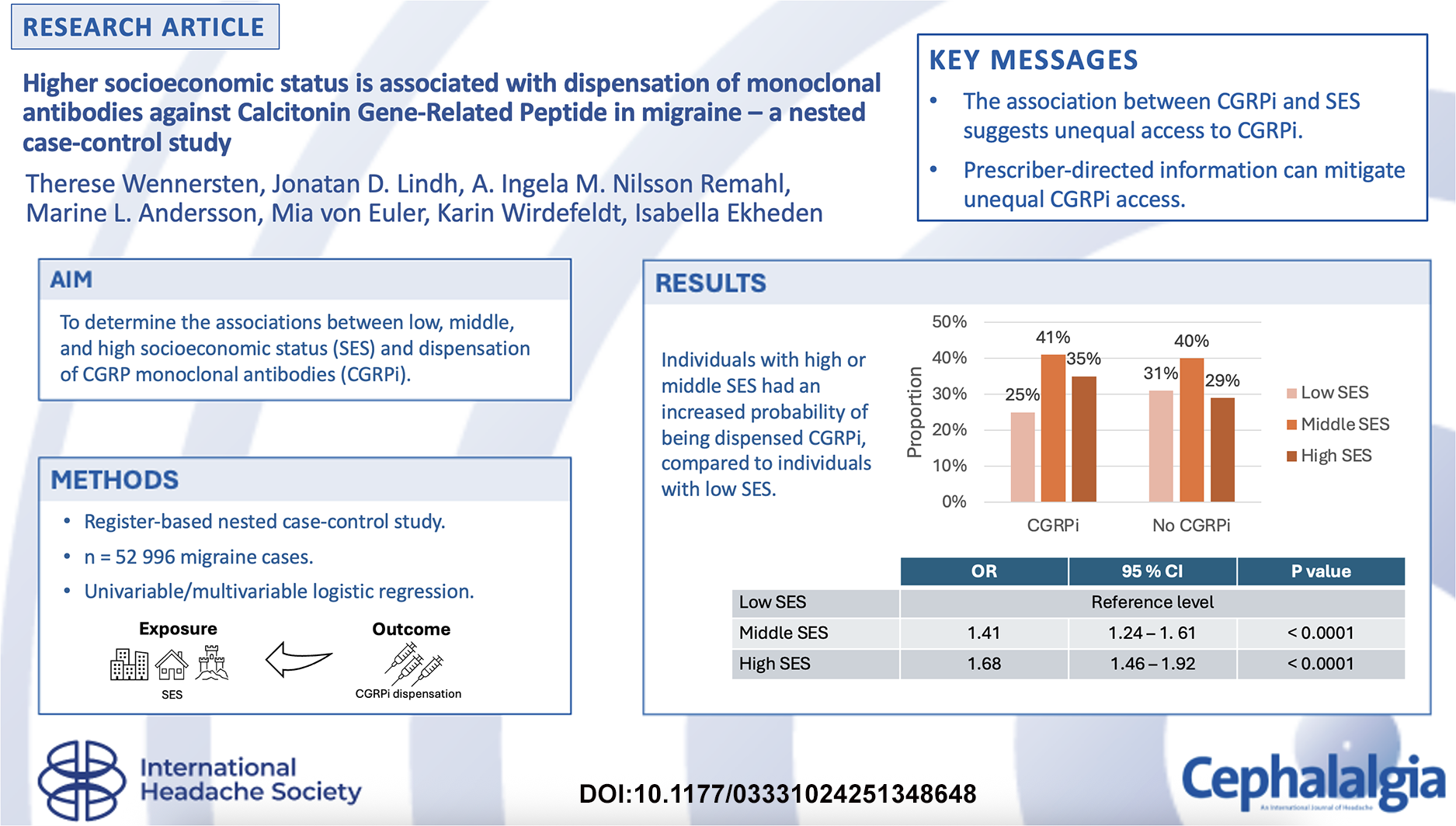
Introduction
Migraine is estimated to affect one billion patients globally (1) with significant productivity losses for society and for the individual because of long periods of episodic or chronic pain. Access to effective treatments against migraine is vital both for society and the patients, but prior studies indicated unequal access to triptans, a first-line treatment for acute migraine episodes. When triptans were protected by patents, in 2005–2009, the annual average cost per prescription for triptan tablets was US$160–212 (2), in contrast to the years 2010–2013, when the corresponding costs were in the range US$54–131. Consequently, higher levels of education, higher income and health insurance were found to be associated with triptan use (3–5).
It is hoped that more effective management of migraine is achievable with monoclonal antibodies against calcitonin gene-related peptide (CGRPi), approved for patients with at least four migraine days per month, but equal access to CGRPi is not guaranteed considering the relatively high cost compared to other prophylactic migraine treatments. To limit the high health care expenses for CGRPi, many countries have more restrictive recommendations for the use of CGRPi than the approved indication, including Sweden, where CGRPi are only subsidized (partially funded within the healthcare system) for patients with chronic migraine who have failed at least two prior prophylactic drugs against migraine (6–9).
Similar to triptans before patents expired, it is possible that CGRPi are more accessible for individuals with a higher socioeconomic status (SES) than individuals with low SES, but studies of the associations between SES and dispensation of CGRPi are scarce. Therefore, the present study aimed to determine the associations between low, middle and high SES and dispensation of CGRPi. Our hypothesis was that migraine patients with a higher SES had an increased risk of CGRPi dispensation compared to patients with a low SES, although the association is expected to be attenuated in a country that generally allows for reimbursement of CGRPi costs.
Methods
Study design and data collection
This was a register-based nested case-control study based on a cohort from the VAL database. The VAL database is an administrative healthcare database containing information from health care providers contracted by Region Stockholm, Sweden. The VAL database holds registrations of healthcare contacts of individuals residing in Region Stockholm, including diagnoses from inpatient care, specialized outpatient care and primary care, as well as registrations of dispensed drugs. Diagnosis codes were available for specialized outpatient and inpatient care since January 1993 and for primary care since 2003. Registrations of dispensed drugs were available since July 2005. Data extraction from the VAL database was performed in June 2022 and marks the end of follow up in the present study.
Study population
Individuals were included in the study population if they were: (1) ≥18 years old; (2) registered in the population register of Region Stockholm during the study period, from 1 January 1993, to mid-June 2022; and (3) diagnosed with migraine (ICD10-code G43 or ICD9-code 346), or dispensed migraine drugs (ATC-code N02C) (see supplementary material, Table S1). The index date was either the date of the first migraine diagnosis or the date of the first dispensation of a migraine drug, whichever occurred earlier. The following individuals were excluded (Figure 1): (1) individuals with missing data regarding age or SES; (2) deceased before 26 July 2018 (when CGRPi were approved); (3) moved out from Region Stockholm before the index date or moved into Region Stockholm <5 years prior to the index date; and (4) no migraine diagnosis. Individuals who moved out of Region Stockholm before the index date or moved into Region Stockholm <5 years prior to the index date were excluded because of the risk of missing registrations of migraine diagnoses and drug dispensations during the time not registered in Region Stockholm.

Flowchart of participants in the study population. Created with BioRender.com.
Definition of cases, controls and exposure
Individuals with migraine with at least one dispensation of CGRPi were defined as cases, and individuals with migraine without CGRPi dispensation were defined as controls.
The exposure was SES at the time of migraine diagnosis. Information about the three SES groups (high, middle and low) was defined by using the mosaic variable in the VAL database. The variable mosaic is based on the internationally used Mosaic™ classification developed by Experian MIS (10,11), and held by InsightOne in the Nordic countries (11).
InsightOne derives the Stockholm mosaic variable in a multi-step process. First, civil registration addresses, originally collected by the Swedish Tax Agency, are extracted. Next, addresses are grouped into 103,000 geographical areas and clustered according to 150 demographic variables (such as age, household income, household composition, educational level, children in the household and country of origin/ethnicity (10)) extracted from CreditSafe, Statistics Sweden and The Swedish Transport Agency (11) to create homogeneous clusters (10,11). After stepwise and repeated clustering, 44 unique sociodemographic clusters remain, informing about the distribution of different sociodemographic clusters in each geographical area (11).
Using the 150 demographic variables once again, a Mosaic factor Status is created with consideration to covariance. For example, high income and high educational level correlate positively and low income correlates negatively with the Mosaic factor Status (12).
By combining the Mosaic factor Status, the mean Mosaic factor Status value for the population and the 44 sociodemographic clusters in Region Stockholm, each sociodemographic cluster is then classified into three SES groups (high, middle and low SES) (12). Each geographical area (with median population of 1,100 adults) is assigned the dominant SES classification from the sociodemographic clustering, resulting in the Stockholm mosaic variable (12), after which the mosaic variable is linked to the registered address in the VAL database. In Region Stockholm, about 30% of the population is classified into the high SES group, 40% into the middle SES group and 30% into the low SES group (12).
Variables of interest
Baseline characteristics collected from the VAL database were age, sex, number of healthcare visits related to migraine (as a proxy variable for migraine severity) and dispensations of the following drugs: metoprolol (ATC-code C07AB02), propranolol (C07AA05), candesartan (C09CA06), amitriptyline (N06AA09), topiramate (N03AX11) and botulinum neurotoxin type A (M03AX01). The frequency of healthcare visits related to migraine and dispensations of the above-mentioned drugs used to prevent migraine episodes, were included if they occurred before the first dispensation of CGRPi, or during the entire study period for individuals without any dispensations of CGRPi.
Statistical analysis
Baseline characteristics for categorical variables are presented with frequencies (counts and percentages), and continuous variables with median values and interquartile range (IQR). To investigate whether there were SES differences between cases and controls, we used univariable and multivariable logistic regression, presented with odds ratios (OR) and 95% confidence intervals (CI). The reference group was low SES. Differences in SES between cases and controls were also assessed by merging the middle SES group with either the high or the low SES group, thereby making the SES variable binary. The multivariable logistic regression was adjusted for age at the time of migraine diagnosis (continuous variable), sex, healthcare visits related to migraine (continuous variable) and time of diagnosis before/after 26 July 2018 (when CGRPi were approved).
A sensitivity analysis was performed where the classification of the SES group of the cases was collected at the date of the dispensation of CGRPi instead of the date of diagnosis.
All analyses were performed using R, version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria). p < 0.05 was considered statistically significant.
Results
Patient characteristics
In total, 108,993 individuals ≥ 18 years were registered with a migraine diagnosis or were dispensed migraine drugs in Region Stockholm from January 1993 to June 2022 (Figure 1). Of these, 55,997 were excluded (51.4%) due to missing age, missing SES, deceased before 26 July 2018, moved out from Region Stockholm before the index date or moved into Region Stockholm <5 years before index date or no migraine diagnosis (including those who were dispensed CGRPi without a migraine diagnosis).
Of the 52,996 individuals ≥18 years with a migraine diagnosis and SES data that remained in the study population, 3.2% (1674 individuals) had been dispensed a CGRPi and were defined as cases. The remaining 51,322 individuals, (96.8%), were defined as controls.
The proportion of women in the cohort was 83% for the cases and 78% for the controls (Table 1). The median age was 41 years (IQR = 34–49 years) for cases and 42 years (IQR = 32–52 years) for controls. Most individuals in both groups (89% of cases and 80% of controls) received their migraine diagnosis before 26 July 2018 (when CGRPi were approved). The median frequency of healthcare visits related to migraine was higher for the cases than controls (16 visits, IQR = 7–28 vs. 2 visits, IQR = 1–4), but the difference between the SES groups regarding healthcare visits (see supplementary material, Table S2) was not statistically significant (p = 0.09). Among cases, 79% had received ≥2 prophylactic drugs, CGRPi excluded (median = 2, IQR = 2–3) compared to 14% among controls (median = 0, IQR = 0–1).
Baseline characteristics of the study participants.

*Number of following drugs that have been dispensed during the study period: metoprolol (ATC-code C07AB02), propranolol (ATC-code C07AA05), candesartan (ATC-code C09CA06), amitriptyline (ATC-code N06AA09), topiramate (ATC-code N03AX11) or botulinum neurotoxin type A (M03AX01).
Abbreviation: IQR = interquartile range.
Furthermore, the proportion of patients who purchased CGRPi outside of the public funding criteria was not statistically different by SES group (p = 0.20) (see supplementary material, Table S3).
Association between SES and CGRPi dispensation by univariable analysis
There was a significant association between SES and CGRPi dispensation in the univariable analysis (Table 2). Compared to individuals with a low SES, individuals with a high SES had OR = 1.53 (95% CI = 1.34–1.74) of being dispensed CGRPi (Table 2). Individuals with middle SES had OR = 1.26 (95% CI = 1.12–1.43) of being dispensed CGRPi compared to individuals with low SES. The association remained significant irrespective of how the middle SES group was merged with the other SES groups. The OR of CGRPi dispensation was 1.33 (95% CI = 1.20–1.47) in the high SES group when compared with the merged low and middle SES group and 1.37 (95% CI = 1.23–1.54) in the merged middle and high SES group compared with the low SES group (Table 2).
Logistic regression analyses showing the association between socioeconomic status and the first CGRPi dispensation.
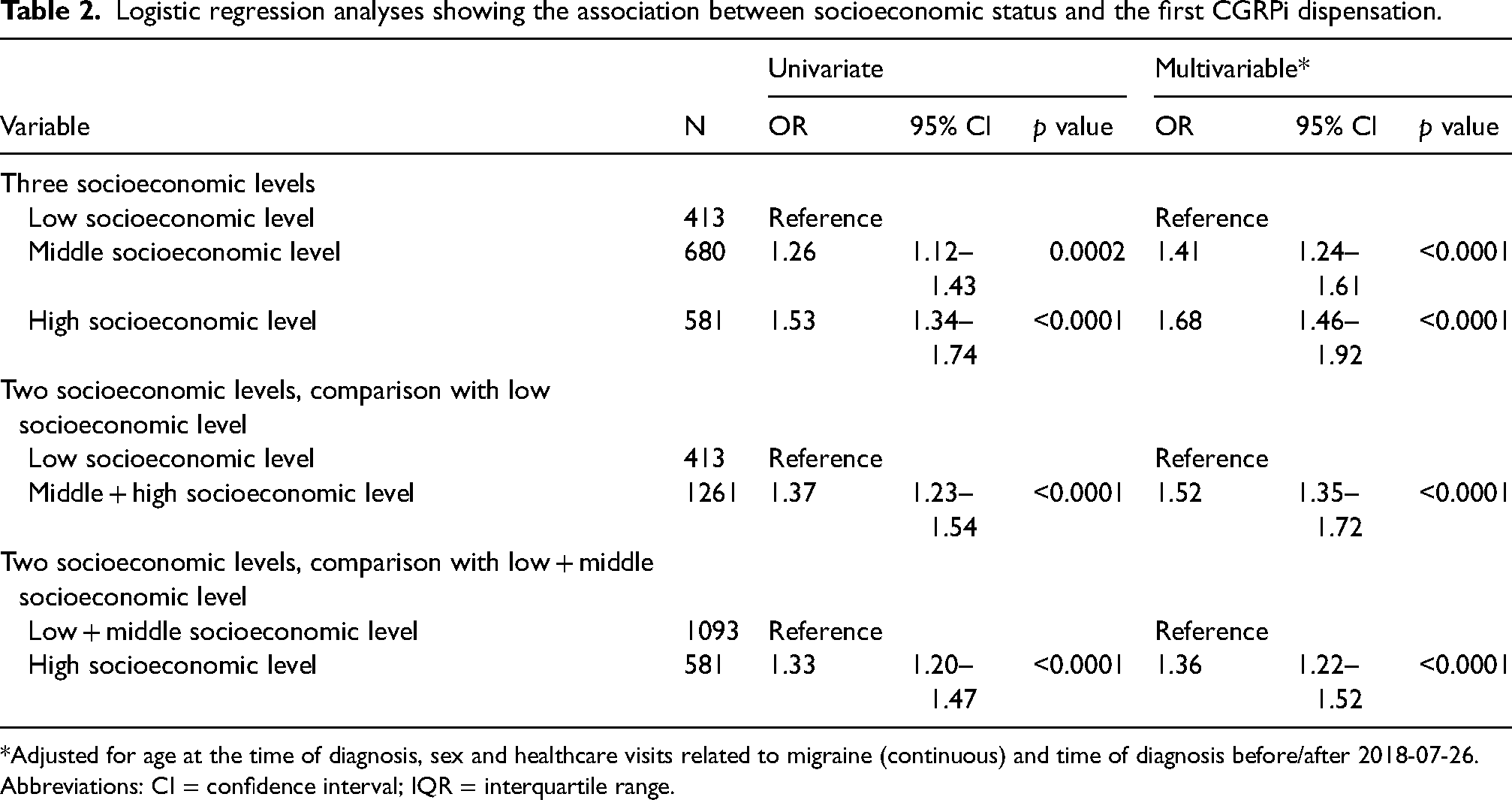
*Adjusted for age at the time of diagnosis, sex and healthcare visits related to migraine (continuous) and time of diagnosis before/after 2018-07-26.
Abbreviations: CI = confidence interval; IQR = interquartile range.
Association between SES and CGRPi dispensation by multivariable analysis
The association between SES and CGRPi dispensation remained statistically significant in the multivariable analysis (Table 2). Compared to individuals with a low SES, individuals with a high SES had OR = 1.68 (95% CI = 1.46–1.92) of being dispensed CGRPi (Table 2). Patients with middle SES had OR = 1.41 (95% CI = 1.24–1.61) of being dispensed CGRPi compared to individuals with low SES. Irrespective of how the middle SES group was merged, the association remained significant. The OR of CGRPi dispensation was 1.36 (95% CI = 1.22–1.52) in the high SES group compared to the merged low and middle SES group and 1.52 (95% CI = 1.35–1.72) in the merged middle and high SES group compared to the low SES group (Table 2).
Sensitivity analysis
The sensitivity analysis showed a trend towards a stronger association for the high SES group in the multivariable analysis, as well as when high SES was compared with a merged group of middle and low SES (see supplementary material, Table S4). Compared to individuals with low SES, individuals with a high SES had OR = 1.78 (95% CI = 1.55–2.05) of CGRPi dispensation (see supplementary material, Table S4). In the middle SES group, individuals had OR = 1.38 (95% CI = 1.21–1.58) for CGRPi dispensation.
Discussion
We found that higher SES is associated with CGRPi dispensation, where individuals with high SES had a 68% higher odds ratio of CGRPi dispensation and individuals with middle SES had a 41% higher odds ratio of a CGRPi dispensation compared to the low SES group. Of particular interest, this study was performed in Sweden, where the cost of CGRPi is subsidized (partially funded within the healthcare system) with a high-cost protection (a maximum cost per year for medicines, irrespective of income level), and, even so, we observed an association between SES and CGRPi dispensation.
Our data support our hypothesis that, in Sweden, CGRPi treatment is associated with higher SES. This is in concordance with previous findings for triptan treatment (3–5) and suggests unequal access to CGRPi. It is less likely that our results indicate an unequal need for CGRPi, because there are documented health care disparities faced among patients with headache disorders (13,14), highlighting that patients with low socioeconomic characteristics have less access to health care (15) despite a higher prevalence of migraine among patients with low household income compared to higher income groups (16). Patients with low SES are therefore expected to have a higher need for migraine prophylaxis, although studies documenting this are lacking.
Despite the lack of direct evidence of a medical need for CGRPi among patients with low SES, the high discontinuation rates that have been observed for migraine prophylaxis preceding CGRPi, indicate that the medications did not fully meet the treatment needs of the patients (17), and were related to an increased use of healthcare resources and costs (18). Moreover, there is robust evidence that CGRPi are more efficacious than placebo, even though the effect size is small (19), and better tolerated than non-migraine specific prophylactic treatment such as topiramate (20,21).
Our results may be explained by a higher health literacy among the individuals in the high SES group, such that these individuals seek more medical care, or demand more when in contact with the healthcare system. Other explanations may be that patients with a higher SES have better access to healthcare through corporate health initiatives, that healthcare workers are more prone to detect a migraine diagnosis, or more vigilant with prophylactic migraine treatments in the higher SES groups. Furthermore, although costs for prescribed medicines are subsidized in Sweden, such costs might lead to lower tendency among patients with lower SES to collect their CGRPi prescription. Importantly, the relatively small proportion of patients that purchase CGRPi independently, outside of public funding criteria, was not statistically different between SES groups, which makes it less likely that individuals with higher SES might access these treatments sooner or more frequently.
The findings obtained in the present study underline the need for healthcare policy interventions addressing the SES disparities in the treatment of migraine. Our study corroborates the previous documentation on health care disparities in headache medicine regarding race/ethnicity, SES and geography (13). Healthcare policy could mitigate these health disparities by emphasizing education interventions suggested in the previous literature towards the public (addressing health literacy) and care providers (with a focus on cultural sensitivity and competence and implicit bias) as well as increasing the representation of underserved groups in headache research (13).
That the reported ORs increased in the multivariable compared with the univariable analyses may seem counterintuitive, but inconsistencies between univariable and multivariable models are documented (22). Here, the minor discrepancy could be attributed to the inclusion of the continuous variables age and healthcare visits related to migraine, variables that appear to be more influential in the multivariable model compared to the univariable model.
The proportion of women in this study was consistent with prior triptan studies. Here, 84% of the cases and 78% of the controls were women. In prior triptan studies, 72–79% of the patients without triptan treatment and 74–87% with triptan treatment were women (3–5). This indicates a representative sample selection of the migraine population in this study.
Two of three previous studies of the associations between SES and triptan use had an increased risk for recall bias because data were collected from self-reported questionnaires and not confirmed by medical records (3–5). Furthermore, as a result of differences in the health care systems in Europe and the USA, the generalizability of the previous studies of SES and triptan use to the European context is limited.
Strengths
The main strength of the present study is the register-based design, which limits the risk for nonresponse bias, recall bias, and selection bias. Another strength is the near complete coverage of drug dispensations in Region Stockholm in that we used the National Prescribed Drug Register, where CGRPi dispensations are included, and the proportion of patients who purchased CGRPi outside of public funding criteria was similar in the different SES groups. Furthermore, we included data from the primary health care, making our results more generalizable to the migraine population in Sweden. In addition, Sweden provided universal coverage of healthcare during the study period, which adds to the strength of our study because patients with chronic migraine, more likely in need of CGRPi, also have an increased need of healthcare services.
Another strength with this study was the robust and multifaceted classification of SES. Although the Mosaic™ data (11) were not accessible on an individual level, the final SES groups were based on a composite of as many as 150 demographic variables, of which educational level is one and other examples are age, household income, household composition, educational level, children in the household and country of birth/ethnicity data. Although disability is not registered directly in the nationwide health registers, indirect effects of disability on income and education are reflected in our SES variable.
Limitations
Because the information underlying the mosaic data was not available on an individual level, there may be misclassification of SES group, but such misclassification would be non-differential since we used the same method for cases and controls. Furthermore, some potential confounders were not addressed, or only partly addressed, such as healthcare-seeking behavior, frequency and severity of migraine episodes and co-morbidities. Nevertheless, the frequency of healthcare visits related to migraine could in part act as a proxy variable for migraine severity. Because the number of healthcare visits related to migraine was similar in the different SES groups, we find it less likely that the SES group is a surrogate for migraine severity or frequency. Although this should be investigated in more detail in future studies, the fact that CGRPi are only subsidized for patients with chronic migraine in Sweden makes our study population relatively homogenous regarding migraine severity and frequency, which further strengthens this assessment. Another limitation is that misclassification of SES group may have occurred if the patient moved between different SES groups over time.
It was not within the scope of this study to investigate historical SES information since the outcome of interest was CGRPi dispensation and not outcomes of the underlying migraine disease.
A limitation with the source data from the National Prescribed Drug Register is the lack of information on treatment indication for dispensed drugs. Therefore, we do not know whether the prophylactic drugs metoprolol, propranolol, candesartan, amitriptyline, topiramate and botulinum neurotoxin type A were prescribed for migraine or other indications. We assumed these drugs were intended as prophylactic treatment for migraine episodes because the dispensation of two or more of these drugs was more common among cases (79%) than controls (14%), although this cannot be confirmed in the present study.
Conclusions
In summary, we observed a higher odds ratio for dispensation of CGRPi among patients with higher SES, compared to patients with low SES, suggesting unequal access to CGRPi. To address this issue and increase the access to CGRPi among patients with low SES, directed information should be provided to prescribers, particularly those in primary care and neurology clinics. Information to the public about symptoms associated with chronic migraine and available prophylactic treatments may also increase the access to CGRPi among patients with low SES.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251348648 - Supplemental material for Higher socioeconomic status is associated with dispensation of monoclonal antibodies against calcitonin gene-related peptide in migraine: A nested case-control study
Supplemental material, sj-docx-1-cep-10.1177_03331024251348648 for Higher socioeconomic status is associated with dispensation of monoclonal antibodies against calcitonin gene-related peptide in migraine: A nested case-control study by Therese Wennersten, Jonatan D. Lindh, A. Ingela M. Nilsson Remahl, Marine L. Andersson, Mia von Euler, Karin Wirdefeldt and Isabella Ekheden in Cephalalgia
Footnotes
Clinical implications
Acknowledgements
We wish to thank Sara Freyland, statistician at the Institute of Environmental Medicine, Karolinska Institutet, for her assistance with the data analyses.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Authors Karin Wirdefeldt, Isabella Ekheden, and Ingela Nilsson Remahl are members of the Drug and Therapeutics Committee in Stockholm County. Remaining authors declare that they have no competing interests.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Drug and Therapeutics Committee in Region Stockholm. The authors Karin Wirdefeldt, Isabella Ekheden and Ingela Nilsson Remahl are members of the Drug and Therapeutics Committee in Neurological diseases in Region Stockholm, and they had specific roles in the conceptualization, design, data collection, analysis, decision to publish and preparation of the manuscript. Karin Wirdefeldt was supported by Region Stockholm (clinical research appointment).
Author contributions
TW, JDL, AIMNR, KW and IE designed the study. TW and IE drafted the application for ethical approval. The ethical approval application was read, revised and approved by all authors. TW and IE drafted the data collection application from the VAL database. The data collection application from the VAL database was read, revised and approved by all authors. TW, JDL, KW and IE participated in, or supervised, data processing and data analysis. All authors interpreted the data. TW wrote the first draft of the manuscript. All authors read, substantively revised and approved the final version of the manuscript submitted for publication. KW and IE obtained funding for the study.
Data availability
The datasets used and analyzed during the current study are not publicly available due to reasons of sensitivity/restrictions to the availability of the data. Requests for data extraction from the VAL database are coordinated by the Center for Health Data (Centrum för Hälsodata) in Region Stockholm. The statistical code is available upon reasonable request from the Principal Investigator.
Ethical statement
Ethical approval for this study was obtained by the Swedish Ethical Review Authority (Dnr 2021-05078, 2022-00372-02).
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.