
Abstract
Background
Migraine and gynecological conditions, such as endometriosis (EDM) and polycystic ovarian syndrome (PCOS), are highly prevalent among females and appear to influence each other, with a potential shared pathophysiological mechanism. Therefore, this study aims to provide a comprehensive summary of the current evidence regarding the relationship between migraine and EDM/PCOS from a clinical perspective.
Methods
A systematic review was conducted using four databases (MEDLINE(Pubmed), EMBASE (Elsevier), Web of Science and Cochrane Library) along with searches in the grey literature. The protocol was registered prospectively on the PROSPERO platform (CRD42024628010). The primary search was performed on 4 December 2024. Eligible studies included observational studies that compared two or more groups of females with migraine, EDM and/or PCOS diagnosis. The modified Newcastle-Ottawa Scale was used to assess the quality of the included studies. Data extraction was performed and results systematically analyzed.
Results
From an initial 408 identified studies, a final selection of 15 was analyzed (14 focused on EDM and 1 on PCOS) with a total of 289,519 individuals included. All selected studies achieved a score of 6 or higher on the mNOS. When comparing females with and without EDM, the prevalence of migraine reached up to 44.7%, with females affected with EDM having up to a five-fold increased risk of developing migraine (adjusted odds ratio = 5.35, 95% confidence interval = 2.11–16.4). When comparing females with and without migraine, a higher prevalence and risk of EDM was observed, with rates reaching 53.4% and an adjusted odds ratio up to 10.5 (95% confidence interval = 2.2–51.4). Mixed findings were found regarding the influence of EDM on migraine characteristics, as well as the impact of migraine in EDM-related symptoms and disease severity. Females with migraine and EDM exhibited higher scores in disability assessment tools (Headache Impact Test-6, 30-item Endometriosis Health Profile), suggesting a greater disease burden. Due to the limited data, no conclusions could be drawn regarding a link between PCOS and migraine.
Conclusions
Although further high-quality research is required to better understand the underlying mechanisms linking migraine, EDM and PCOS, the current evidence supports a significant association between migraine and endometriosis.
Introduction
Females with migraine frequently experience non-headache-related pain, including visceral pain associated with comorbid gynecological conditions. Gynecological disorders such as endometriosis (EDM) and polycystic ovary syndrome (PCOS), similar to migraine, are highly prevalent among females during their reproductive age (1–3). All together, these conditions significantly reduce quality of life, contribute to greater disability (4–6), and impose a substantial economic burden on healthcare systems (6–9).
EDM is a complex and often chronic inflammatory disorder affecting up to 10% of reproductive-age females, in which endometrial-like tissue grows outside the uterus, most commonly within pelvic structures (3,10,11). Its clinical spectrum is heterogeneous, including dysmenorrhea, menorrhagia, pelvic pain, dyspareunia, bowel and urinary disturbances and infertility (Figure 1). While surgical visualization and histological confirmation remain the gold standard for diagnosis, certain forms can be detected via ultrasonography (USG) and pelvic magnetic resonance imaging (MRI). Several mechanisms have been proposed for the origin of ectopic lesions, including retrograde menstruation, coelomic metaplasia, metastatic spread or neonatal uterine bleeding, while lesion persistence is influenced by immune, angiogenic, hormonal and genetic factors. Treatment strategies include surgical removal of lesions and/or hormonal therapy (10,11).

The main symptoms or manifestations of the three included conditions in the systematic review: migraine, polycystic ovarian syndrome and endometriosis.
PCOS is an endocrine disorder affecting up to 13% females (2) and represents the leading cause of irregular menstrual cycles and anovulatory infertility in reproductive-age females (Figure 1) (12). Adult diagnosis requires at least two of the following criteria: clinical or biochemical hyperandrogenism, ovulatory dysfunction and polycystic ovarian morphology and/or elevated anti-Müllerian hormone levels (13). PCOS is strongly linked with insulin resistance, obesity, increased risk of type 2 diabetes, metabolic syndrome and cardiovascular disease (12). Although its pathology remains incompletely understood, management approaches include lifestyle modifications (particularly body weight reduction), pharmacological treatment with insulin-sensitizing agents, and hormonal therapy to suppress ovarian androgen secretion and protect the endometrium (12).
Beyond their individual impact, migraine, EDM and PCOS share epidemiological and clinical risk factors, such as early menarche and menorrhagia for migraine and EDM (14–16), and obesity for PCOS and migraine (17). Moreover, all three are associated with overlapping comorbidities, including psychiatric disorders such as anxiety and depression (16,18–20). Hormonal dysregulation and treatments prescribed for EDM and PCOS may also influence migraine course (21), and genetic factors may contribute to the observed overlap (22–24).
Interest in the comorbidity between migraine and EDM has grown in the last decade, culminating in the recent publication of two systematic reviews (25,26). These reviews provide valuable and complementary insights by focusing on the association and risk quantification between migraine and EDM. However, the present work goes beyond these efforts by adopting a clinically oriented perspective on EDM and further broadens the scope by also addressing PCOS, which has not previously been evaluated in a systematic review. Increasing evidence regarding the link between these disorders could not only contribute to a better understanding of the underlying etiology of each pathology, but also aid in reaching an early diagnosis, which is frequently delayed in all three disorders (9,14,15). Additionally, it could help refine treatment approaches, ultimately leading to better clinical management and a significant long-term multidimensional improvement in the lives of the affected females.
Therefore, the aim of this systematic review is to synthesize the current evidence on prevalence, risk factors, and clinical manifestations in females with migraine and two gynecological disorders: EDM and PCOS. Additionally, it aims to identify limitations in the existing literature to better inform both patient care and future research in this area.
Methods
This systematic review adhered to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) reporting guidelines (27). The protocol was registered prospectively on the International Register of Systematic Reviews (PROSPERO) platform (Registration ID: CRD42024628010; 3 December 2024).
The literature search was conducted on 4 December 2024, across four databases: MEDLINE-PubMed, EMBASE (Elsevier), Web of Science-Web of Science Core Collection (Clarivate) and Cochrane Library. OpenGrey and Google Scholar were used to capture the grey literature. The search was collaboratively performed by a librarian specialist from the Vall d’Hebron Barcelona Hospital Campus Library and LG-D. To ensure a comprehensive review, LG-D and TJ-B screened the reference lists of relevant articles and related reviews both forward and backward to identify studies that might have been missed in the electronic searches. The literature search used medical subject heading terms (MeSH) and synonyms, combined with Booleans operators “AND” and “OR”. The primary search terms and groups included: (i) “Migraine”, “Migraine Disorders”, (ii) “Polycystic Ovary Syndrome” and (iii) “Endometriosis”, with no filters applied. Details of the comprehensive search strategy used are provided in the supplementary material (Doc. S1).
Inclusion criteria for the systematic review comprised observational studies, including case–control, cohort or cross-sectional designs, that compared at least two groups of females with EDM and/or PCOS and a migraine diagnosis according to the International Classification of Headache Disorders (ICHD criteria) (28), using validated migraine tests and/or diagnosis confirmation by a physician. Exclusion criteria consisted of articles for which full-text articles were unavailable in English or Spanish, as well as study types such as reviews, case reports, case series, animal studies, conference abstracts, editorials, theses or commentaries.
Regarding the article selection process, two reviewers LG-D and TJ-B independently assessed all articles based on their titles and abstracts. Abstracts deemed potentially eligible according to the inclusion criteria and without any exclusion criteria were advanced to full-text screening (Figure 2). In cases of disagreement between the two reviewers, a third reviewer (HL-P) was consulted to reach a consensus.

Flowchart of studies in the systematic literature review following PRISMA guideline and recommendations. Abbreviations: EDM = endometriosis; PCOS = polycystic ovarian syndrome.
Concerning data extraction, two reviewers (LG-D and TJ-B) independently conducted data extraction for all the selected studies, recording the information in an Excel electronic spreadsheet. The following details were extracted from each paper: title, author, year of publication, sample size, demographics (age), study country, and main objectives and results. In the included articles, risk of bias was independently assessed by two reviewers (LG-D and TJ-B) following the modified Newcastle-Ottawa Scale for Observational Studies (mNOS) rating poor (0–3 stars), fair (4–6 stars) or high quality (7–9 stars) data. Any discrepancies were resolved by consulting a third reviewer (HL-P).
Results
Included articles
Our search initially identified a total of 408 original articles and reviews. After removing 83 duplicates, 325 papers remained. These papers were subsequently screened by title and abstract, narrowing the selection to 21 articles. A full-text review of these articles resulted in the inclusion of 15 papers for the analysis (14 on migraine-EDM and one on migraine-PCOS) (Figure 2), with a total of 289,519 individuals included.
Regarding EDM and migraine, the risk of bias for each study is summarized in the supplementary material (see supplementary material, Table S1). The included studies consisted of six case–control, two cohort and six cross-sectional studies. Among these, one article scored 6, two articles scored 7, two studies scored 8 and nine studies scored 9, indicating a generally high-quality data. Most of the included studies were published in the last 10 years (8/14; 57.1%), with the oldest study dating from 2004. When analyzing the authorship of the included articles, the majority were affiliated with Gynecology and/or Obstetrics departments (54/100), followed by Neurology or Neuroscience departments (32/100) and other fields such as Epidemiology or Genetics (16/100) (see supplementary material, Table S2). Eight of the included studies compared females with and without EDM (Table 1), two studies compared females with and without migraine (Table 2) and four studies compared females with EDM and migraine to females with only EDM or only migraine (Table 3).
Summary of studies comparing females with endometriosis and without endometriosis

Abbreviations: EDM = endometriosis; MG = migraine; AM = adenomyosis; WoEDM = without endometriosis; WoMG = without migraine; MG + EDM = migraine and endometriosis; HC = healthy control; AOR = adjusted odds ratio; SUP = superficial peritoneal endometriosis; OMA = ovarian endometrioma, DIE = deep infiltrating endometriosis; TUS = transvaginal ultrasound; MZ = monozygotic; DZ = dizygotic; vs. = versus; ICHD = study using International Classification of Headache Disorders (ICHD-1, first edition; ICHD-2, second edition; ICHD-3, third edition); NHMRC, Australian National Health and Medical Research Council; MRM = menstrually-related migraine; nr = not reported; rASRM score = revised American Society for Reproductive Medicine score; VAS = visual analogue scale.
Studies comparing females with and without migraine

Abbreviations: EDM = endometriosis; MG = migraine; WoEDM = without endometriosis; WoMG = without migraine; MG + EDM = migraine and endometriosis; HC = healthy control; AOR = adjusted odds ratio; SUP = superficial peritoneal endometriosis; OMA = ovarian endometrioma, DIE = deep infiltrating endometriosis; TUS = transvaginal ultrasound; vs. = versus; ICHD = study using International Classification of Headache Disorders (ICHD-1, first edition; ICHD-2, second edition); MRM = menstrually-related migraine; MWoA = migraine without aura.
Studies comparing females with comorbidity of migraine and endometriosis to females with only endometriosis and/or only migraine
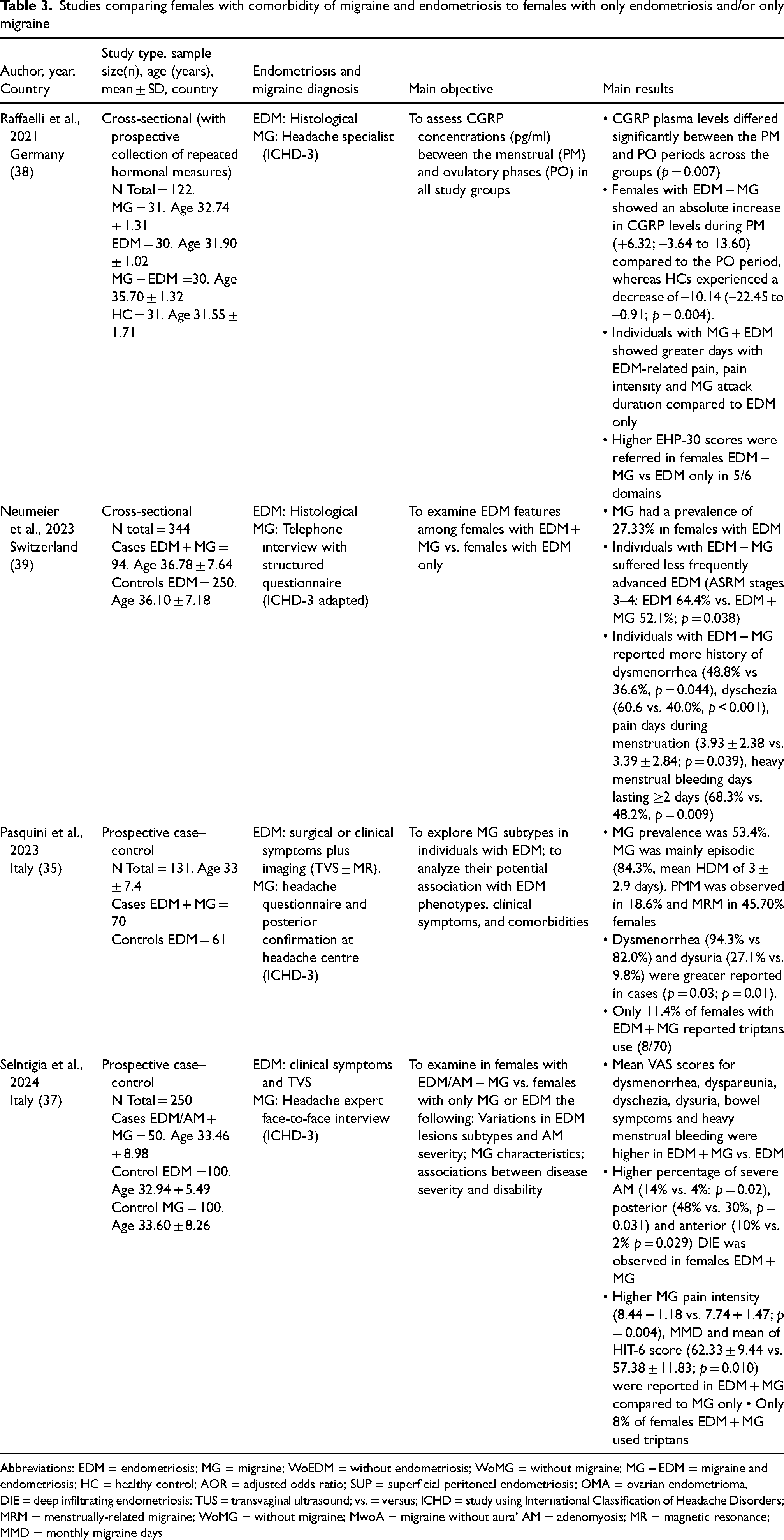
Abbreviations: EDM = endometriosis; MG = migraine; WoEDM = without endometriosis; WoMG = without migraine; MG + EDM = migraine and endometriosis; HC = healthy control; AOR = adjusted odds ratio; SUP = superficial peritoneal endometriosis; OMA = ovarian endometrioma, DIE = deep infiltrating endometriosis; TUS = transvaginal ultrasound; vs. = versus; ICHD = study using International Classification of Headache Disorders; MRM = menstrually-related migraine; WoMG = without migraine; MwoA = migraine without aura’ AM = adenomyosis; MR = magnetic resonance; MMD = monthly migraine days
Regarding PCOS, only one case–control study, with a mNOS risk score of 8 was finally included. From the total authors (n = 3), two were from the Neurology Department (see supplementary material, Table S1 and S2).
Migraine and endometriosis
Prevalence and risk factors
A higher prevalence of migraine has been reported in females with EDM compared to those without in several of the included studies (4,29–33), with estimates ranging from 14.2% to 44.7% (29,30). However, one study reported no significant difference in the overall migraine prevalence in females with and without EDM (34). Besides, some studies have assessed the risk of developing migraine in females with EDM (24,29,31,32), consistently finding a significantly increased risk, ranging from 1.35 to 5.35 times higher (Table 1) (adjusted odds ratio (AOR) = 1.35, 95% confidence interval (CI) = 0.94–1.95, p = 0.009 (24); AOR = 5.35 95% CI = 2.11–16.4, p < 0.001 (29)).
Age appears to influence migraine risk in females with EDM. One study found that each additional year of age was associated with a 23% increase in migraine risk (OR = 1.23, 95% CI = 1.13–1.16; p ≤ 0.001) (29). Another study reported that migraine onset occurred earlier in females with EDM (16.4 ± 7 years) compared to those without (21.9 ± 6.1 years; p = 0.001) (4). However, another study found no significant difference in headache onset age between females with both migraine and EDM and those with migraine alone (16). Nonetheless, age does not seem to fully explain the association between migraine and EDM (24). Besides, although migraine and EDM symptoms typically emerge during adolescence or young adulthood, there seems to be an average delay of 12 years between both diagnoses (35).
On the other side, individuals with migraine appear to have higher prevalence and risk of EDM compared to those without migraine, with prevalence estimates ranging from 22% to 53.4% (16,35–37) and an up to 10.5-fold increased risk of EDM (AOR = 10.5; 95% CI = 2.2–51.4) (36). Furthermore, the association between migraine and adenomyosis (AM), a condition in which endometrial tissue infiltrates the muscular wall of the uterus, has also been explored. One study found a higher prevalence of migraine among females with both AM and EDM compared to those with isolated AM (42.8% vs. 9.8%, p = 0.001) (33). Moreover, in this study, females with migraine had a five-fold higher risk of EDM coexisting with AM compared to those without EDM (AOR = 5.4; 95% CI = 3.0–9.5, p < 0.05) (33).
Migraine clinical features and treatment
One study found that both migraine with aura (MA) and migraine without aura (MWoA) were more frequent in females with EDM compared to those without (MA: 13.5% EDM vs. 1.2% no EDM, p < 0.001; MwoA: 24.8% EDM vs. 13.9% no EDM; p < 0.016) (4). Another study found no differences in migraine subtypes (MA and MwoA) between females with migraine and EDM compared to those with only migraine (37).
Regarding migraine characteristics, females with both migraine and EDM experienced a higher frequency of monthly migraine days (MMD) (36,37), greater pain intensity (33,37) and longer attack duration (38), compared to those with only migraine. Conversely, other studies found no significant differences in migraine pain intensity, frequency, or duration between females with and without EDM (4,34). Regarding self-reported menstrually-related migraine (MRM), two studies found no differences in the number of MRM attacks between females with and without EDM (4,30).
Few studies have assessed migraine treatment. Ferrero et al. (4) reported that only 27.8% of females with both migraine and EDM have consulted a headache specialist. In this study, 70.6% of females with EDM and migraine used NSAIDs for headache management, while only 7.8% used triptans (4). Other studies showed reported triptans usage rates of 8% to 11.4% in females with both EDM and migraine (35,37).
Endometriosis clinical features
Findings on EDM symptom severity and its association with migraine remain inconsistent. One study found that females with both migraine and EDM reported higher chronic non-cyclic pelvic pain intensity than those with EDM but no headache (visual analogue scale (VAS) 3.6 ± 2.9 vs. 2.3 ± 2.8; p = 0.007) (32). In this line, Selntigia et al. (37) reported higher VAS scores for EDM symptoms in individuals with both migraine and EDM. However, other studies have found no statistically significant association (4,32).
Symptom frequency also appears to be higher in individuals with both migraine and EDM. Compared to those with EDM alone, females with both conditions experienced more frequently dysmenorrhea (35), dyschezia (39), dysuria (35), prolonged menstrual pain (39) and long-lasting heavy menstrual bleeding (39). Indicators of heavy menstrual bleeding were also more prevalent among females with migraine compared to those without migraine (36). Moreover, a history of menorrhagia (36) and dysmenorrhea (16,35) was reported more frequently in females with both migraine EDM than in those with either condition alone (16,35,36).
The relationship between migraine and EDM severity stages remains debated. One study found that females with migraine had a significant higher risk of moderate to severe EDM than those without (revised American Society for Reproductive Medicine (rASRM) score stage IV – severe: AOR = 4.6, 95% CI = 2.7–8.1, p < 0.001; stage III – moderate: AOR = 3.6, 95% CI = 2.1–6.2, p < 0.001) (33). Another study reported that females with migraine and EDM rASRM stage 3–4, were more likely to have intestinal EDM (39). Additionally, females with both EDM and migraine exhibited higher frequency of ovarian endometriomas (OMA) (OR = 2.78, 95% CI = 1.11–6.98) (32), deep infiltrating endometriosis (DIE) (32,37) and AM (37). Conversely, other studies found no association between migraine prevalence and EDM severity (4), rASRM scores (30), OMA (35), superficial peritoneal endometriosis (SUP) (32) or DIE (35).
No significant differences in infertility prevalence have been reported between individuals with both migraine and EDM (16%) and those with only migraine (14%; p = 0.745) (37). Indeed, one study found that females with both migraine and EDM had more pregnancies and deliveries than those with EDM alone (pregnancies 48.9% vs. 37.2%; p = 0.048; deliveries 0.57 ± 0.91 vs. 0.30 ± 0.63; p = 0.009) (39).
Migraine, EDM and calcitonin gene related peptide (CGRP)
Only one of the included studies has specifically assessed fluctuations in CGRP plasma levels in migraine and EDM individuals, particularly during the menstrual and ovulatory phases (38) (Table 3). Females with both conditions showed an absolute increase in CGRP levels during menstruation (+6.32 pg/ml; −3.64 to 13.60 pg/ml), whereas healthy controls (HCs) experienced a decrease (−10.14 pg/ml; −22.45 to −0.91 pg/ml; p = 0.004). Relative changes in CGRP levels between the periovulatory and menstrual phases were significant in females with both migraine and EDM compared to HCs, even after adjusting for covariates. However, no correlation between CGRP levels and migraine or EDM pain frequency was observed.
Comorbidity and disability associated with migraine and EDM
A study by Tietjen et al. (16) found that females with EDM and migraine exhibited higher rates of self-reported comorbidities, including interstitial cystitis (OR = 10.6, 95% CI = 1.9–56.5), chronic fatigue syndrome (OR = 3.6, 95% CI = 1.1–11.5) and anxiety (OR = 2.2; 95% CI = 1.0–4.7) compared to HCs.
Few studies have assessed the impact of migraine and EDM comorbidity on daily activities. Actual evidence suggests that females presenting with both conditions (migraine and EDM) experience greater daily life impairment (4). Specifically, one study suggested a reduction in work productivity of up to 46.7% (±18.7%) in this group compared to 30.5% (±8.6%) in females without EDM (p < 0.001) (4). Another study showed that females with both migraine and EDM presented a poorer overall quality of life (p = 0.003) (36). However, findings regarding migraine and EDM-related disability scales have been mixed.
One study indicated that individuals with both migraine and EDM scored higher on the Headache Impact Test-6 (HIT-6) compared to those with only migraine (4,16). However, two studies reported that Migraine Disability Assessment (MIDAS) scores were not significantly associated with the presence of EDM in females with migraine (4,36). Besides, females with migraine and EDM had higher Endometriosis Health Profile questionnaire (EHP-30) scores, particularly in the pain domain, indicating a greater burden of EDM-related symptoms compared to those with EDM alone (38).
Heterogeneity of the included studies
The included studies exhibit significant heterogeneity. First, regarding the included studies design, with only a few being prospective cohort studies (2/15) (24,38). Second, geographic variability was evident, with most studies conducted in Europe (6/15; 40%) and Asia (5/15; 33.3%), while fewer were conducted in the USA (3/15; 20%) and Oceania (1/15; 6.67%). Additionally, the studies spanned from 2004 to 2023, which may have influenced the diagnosis of the different included conditions (EDM/PCOS and migraine), as diagnostic criteria and methods have evolved over time.
Furthermore, differences in inclusion and exclusion criteria were observed across the studies. While most focused-on female of reproductive age, with median ages around 30–40 years, some studies included females aged over 50 years (16,24). Besides, although the majority explicitly reported using ICHD criteria for migraine diagnosis (13/15; 86.7%), one study applied migraine validated screening tools (30), while another relied on migraine coding with subsequent physician-validated diagnoses (31). Even among those ICHD criteria, validation tools or physician validation, initial self-reported diagnoses were applied in some studies (32,34,35).
Variations in EDM diagnostic methods criteria were also present, with some studies using clinical symptoms combined with transvaginal USG or MRI (31,35,37), while others required surgical or histological confirmation (4,16,24,29,30,32–36,38,39). Moreover, some studies selected highly specific females, mainly from tertiary care or highly specialized units. Some of these encompass including females with mandatory chronic pelvic pain (34,38) or excluding females with (recent) contraceptive or hormonal therapy use, which is the first-line treatment for EDM (33,34,38).
Samples sizes of the included studies also varied widely, ranging from 102 (36) to 283,987 (31) individuals. Furthermore, adjustments factors for OR calculations varied across studies. While most adjusted for age (16,29,31,32,36,38), others adjusted for other additional factors such as body mass index (29,32,38), family history of migraine (32), history of depression (36), infertility (31), pelvic pain (31), hormonal treatments (31) or surgical treatments (31).
Migraine and PCOS
Only one prospective case–control prospective study, conducted in Iran, specifically examined the prevalence and characteristics of migraine among individuals with and without PCOS (40). In total, 284 females were included (females with PCOS: n = 107, age 29 ± 7.3 years; females without PCOS: n = 133, age 28.8 ± 7 years). No differences in the prevalence of migraine were observed between the two groups (with PCOS 17.8% vs. without PCOS 10.5%, p = 0.13). Furthermore, no differences in mean pain headache intensity (5.7 ± 2.7 vs. 5.8 ± 2.8; p = 0.62), frequency (41 vs. 44 attacks; p = 0.17) or migraine preventive treatments (12.6% vs. 12.03%, p = 0.52) were observed between groups.
Discussion
This systematic review provides a comprehensive summary of the evidence from the past decade on the relationship between migraine and EDM/PCOS. Our analysis explored the association in three directions: comparing females with and without migraine, females with and without EDM/PCOS, and females with comorbidities versus those with only migraine or only EDM/PCOS. The evidence, especially regarding EDM and migraine, suggests that the link between these conditions cannot be solely attributed to its high prevalence among young females. In contrast, the data for PCOS and migraine remains very limited, precluding firm conclusions.
Across included studies, migraine was consistently more prevalent in females with EDM (4,23,29–33), and EDM was more frequent in females with migraine (16,35,36,39), supporting a bidirectional association. Both EDM and migraine appear to increase the risk of developing the other once established (24,31,32,36). These findings align with the two recent systematic reviews on this topic (25,26). Colombo et al. (26) performed a robust meta-analysis of 331,655 females, demonstrating a twofold increased risk of migraine in individuals with EDM (OR = 2.25, 95% CI = 1.85–2.72). This association remained significant after sensitivity analysis accounting for risk of bias, hormonal therapy and confounders. Lechowicz et al. (25), while not conducting a meta-analysis, also confirmed a higher prevalence of migraine among female with EDM.
When focusing on clinical characteristics, our review found inconsistent results regarding headache intensity, duration and other migraine features, making definitive conclusions difficult to establish (4,12,14,22,25–31). Colombo et al. (26) identified a stronger association with MWoA (OR = 2.64, 95% CI = 1.89–3.69), but not with aura (OR = 3.47, 95% CI = 0.53–22.89), whereas Lechowicz et al. (25) emphasized links with chronic migraine and proposed shared genetic predispositions, including estrogen receptor polymorphisms. Notably, in contrast to previous reviews, our work incorporated detailed data on functional outcomes, showing that females with both EDM and migraine experience greater disability and reduced quality of life, as reflected by higher HIT-6 scores (4,16) and lower work productivity (4).
Several pathophysiological mechanisms have been proposed to link migraine and EDM, although the exact mechanism remains unclear. While the scope of this review does not focus on the potential common pathophysiological mechanisms between migraine and EDM, and preclinical studies were excluded from our review, the included studies frequently discussed potential mechanisms. One key factor seems to be CGRP, which plays a crucial role in both migraine attacks (41) and pro-inflammatory responses in EDM (42). Its expression is regulated by the mitogen-activated protein kinases (MAPK) signaling pathway (43,44) and its homeostasis influenced by ovarian sex hormones (21,44). Hormonal fluctuations, particularly estrogens, are also central to both migraine and EDM conditions, affecting pain perception and exacerbating symptoms through modulation of pain pathways (45,46). Additionally, genetic predispositions and markers (i.e. ESRI gene) (22–24), as well as pro-inflammatory molecules such as prostaglandins, nitric oxide and cytokines, have been linked to shared pathogenesis of EDM and migraine (42–44). These inflammatory mediators, influenced by hormonal changes, appear to sustain both central and peripheral sensitization, contributing to chronic pain cycles (47,48). Additionally, psychiatric comorbidities, such as depression and anxiety, often seen in both conditions, may be linked to dysfunction in the serotoninergic system (49). Other comorbidities, including fibromyalgia, cystitis, and irritable bowel syndrome, suggest a connection with the autonomic nervous system, further complicating the overlap between migraine and EDM (50).
There is currently a pressing need for studies investigating the pathophysiological mechanisms underlying the comorbidity between migraine and EDM. To date and to our knowledge, only one study has explored CGRP factors for both EDM and migraine conditions in humans (38), although preclinical studies are increasing on this topic and will potentially lead to new perspectives. Further research is essential to validate these findings and to examine additional mechanisms such as the roles of the Schwann cells (51), macrophages (52) or other hormones such as prolactin (53), among others.
An additional finding in our review concerns the distribution of author affiliations in the included studies: over half were led by gynecology/obstetrics departments, approximately one-third by neurology or neuroscience, and the remainder in epidemiology or genetics. This disciplinary distribution may influence study design, diagnostic approach and outcome priorities. For example, gynecology-led studies may focus more on surgical diagnosis of EDM and disease staging, whereas neurology-led studies may employ more rigorous migraine phenotyping using standardized headache classifications. Such differences may contribute to heterogeneity in the literature. Recognizing these perspectives is important when interpreting the results and underscores the need for multidisciplinary collaborations to improve research quality and integrated management strategies for females with comorbid migraine and EDM.
Moving forward, and as previously stated, no definitive conclusions can be drawn regarding the association between migraine and PCOS due to the limited data available for analysis (40). Other studies not meeting our inclusion criteria suggest a higher prevalence of migraine and/or headache in females with PCOS. For example, in a nationwide Danish cohort of 19,199 females with PCOS and 57,483 controls, PCOS was associated with a twofold increased risk of migraine (2.1% vs. 0.9%; RR = 2.3) and a 1.7-fold higher prescription rate of analgesics/migraine medications (25.4% vs. 15.3%) (54). In a case–control study from Southern Punjab, Pakistan, migraine was reported in 55.4% of PCOS patients compared to 10.7% of controls (OR = 10.4, 95% CI = 5.78–18.71; p < 0.001) (55). A cross-sectional Dutch study reported a 46.9% lifetime prevalence of migraine among middle-aged females with PCOS (56). These findings suggest a possible association between PCOS and migraine, although evidence remains sparse and heterogenous.
The etiology of PCOS, like that of migraine, remains incompletely understood. Nevertheless, the previously discussed hypotheses linking migraine and EDM, particularly those related to hormonal factors and inflammation, may also play a role in the relationship between migraine and PCOS. However, given that PCOS is also classified as an endocrine disorder, additional metabolic factors, including obesity, insulin resistance and androgen-related hormonal imbalances, should be considered in this context (57).
Study limitations
As mentioned in the Results, the included studies in our systematic review vary significantly in study design, diagnostic methods and population characteristics. These variations contribute to the heterogeneity of findings, potentially affecting the comparability of results across studies and limiting their generalizability.
Regarding selection bias, although our criteria were broad, some studies with a different main primary focus (e.g. examining overall EDM comorbidities) or study design (e.g. lacking a comparator group) may contain relevant information that was not included. Despite conducting a comprehensive search across four databases and the gray literature to minimize publication bias, as well as a previous systematic review on EDM and migraine not detecting such bias (58), we cannot rule out the exclusion of studies reporting negative results. Additionally, as the review primarily includes observational studies, it does not allow for causal conclusions.
Differences in findings between this review and previous systematic reviews (25,26) may also be explained by methodological differences. We excluded studies relying solely on self-reported or coding-based diagnoses, which were included in other reviews. While this approach increased diagnostic certainty, it also reduced the number of eligible studies, especially in PCOS.
Clinical implications
Currently, there are no established clinical recommendations for managing females with both migraine and EDM/PCOS. Given the prevalence of these conditions, their potential association and the significant diagnostic delays reported (59–61), consultations with gynecologists and neurologists present an opportunity to identify comorbidities. However, due to the limited evidence available, developing specific clinical and treatment recommendations remain challenging.
Patients with EDM, and potentially PCOS, should be routinely screened for migraine, with the ID Migraine™ tool (62) as a potential screening aid for gynecologists. If migraine is suspected, referral to a general practitioner or neurologist, accompanied by a headache diary, should be recommended for definitive diagnosis and follow-up, in accordance with the healthcare system and country-specific protocols. Both acute and preventive treatments should also be considered based on current guidelines because further research is needed to evaluate the impact of migraine-specific treatments on both headache and gynecological pain relief (63,64). When initiating hormonal treatment, migraine comorbidity should be carefully assessed. Recommendations should align with those for females with migraine alone, with special attention to the presence of aura and the possibility of menstrually-related migraine (21,65,66).
In young females presenting with migraine in the outpatient clinics, a systematic menstrual history evaluation, including menstrual cycle regularity, associated pain and blood flow, as well as pregnancy intentions, is recommended. Depending on the responses, and particularly in the context of dysmenorrhea, menorrhagia or pelvic pain interfering in daily activities, referral to a gynecologist should be considered. This is especially relevant for EDM and PCOS because clinical history alone is insufficient and complementary diagnostic procedures are required (10–13).
These considerations emphasize the need for closer collaborations between neurologists and gynecologists in the comprehensive care of affected females. Establishing multidisciplinary committees, clinical case discussions and implementing specialized training programs for gynecologists and neurologists could enhance awareness and knowledge across specialties. Gynecologists could become more familiar with migraine management, while neurologists could develop a better understanding of gynecological conditions and implications of different hormonal therapies. The interdisciplinary approach may lead to improved patient outcomes and more comprehensive management strategies for females affected by both conditions.
Taken together, our findings complement and extend those of Colombo et al. (26) and Lechowicz et al. (25). Colombo et al. (26) provided the most robust quantitative estimate of the association, while Lechowicz et al. (25) offered broader clinical and pathophysiological perspectives. In contrast, our review not only corroborates the epidemiological evidence linking EDM and migraine, but also broadens the scope to PCOS, a condition not previously examined in systematic reviews. By adopting a clinically oriented approach, our work highlights the increased burden of migraine in females with gynecological disorders, the bidirectionality of associations, and their impact on clinical outcomes, thereby filling an important gap in the literature.
Conclusions
Migraine appears to be more prevalent among females with EDM, who, in turn, face a higher risk of developing migraine compared to those without it. Evidence suggests that both disorders influence each other with respect of clinical symptoms and disease progression. Further high-quality research is needed to better understand the potential pathophysiological relationship between migraine and PCOS. Given the high prevalence of these three conditions, addressing their comorbidity could have significant public health implications, and certain treatments could be effective for both conditions.
Key findings
Females with EDM and those with migraine appear to have a reciprocal increased risk of developing the other condition compared to individuals without either disorder.
EDM and migraine disorders may mutually influence each other in terms of symptom severity and clinical course.
The association between migraine and PCOS remains unclear, highlighting the need for further research.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251386776 - Supplemental material for The interplay between migraine, endometriosis and polycystic ovarian syndrome: A systematic review
Supplemental material, sj-docx-1-cep-10.1177_03331024251386776 for The interplay between migraine, endometriosis and polycystic ovarian syndrome: A systematic review by Laura Gómez-Dabó, Teresa Jordà-Baleri, Helena Losa-Puig, Edoardo Caronna and Patricia Pozo-Rosich in Cephalalgia
Footnotes
Acknowledgments
We thank Miriam Basagaña-Farrés (Vall d’Hebron Barcelona Hospital Campus Library) for contributing to the literature search and search term strategy in all electronic databases.
Author contributions
LG-D, EC and PPR made substantial contributions to conception and study design. LG-D and TJ-B worked on acquisition of data. LG-D, TJ-B and HL-P wrote the first draft. EC and PPR critically revised and finally approved the version to be published. All authors fully comply with and approve the version to be published.
Data availability
All data are available and will be shared on reasonable request from any qualified investigator.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The salary of LG-D has been partially funded by Río Hortega grant Acción Estratégica en Salud 2021–2023 from Instituto de Salud Carlos III (CM24/00072); TJ-B and HL-P report no disclosures relevant to the manuscript. EC has received honoraria from Novartis, Chiesi, Lundbeck, MedScape, Lilly, Teva and Dr Reddy's; his salary has been partially funded by Río Hortega grant Acción Estratégica en Salud 2017–2020 from Instituto de Salud Carlos III (CM20/00217) and Juan Rodés fellowship, Subprograma Estatal de Incorporación de la Acción Estratégica en Salud 2023 (JR23/00065). He is a junior editor for Cephalalgia. PP-R has received, in the last three years, honoraria as a consultant and speaker for: AbbVie, Dr Reddy's, Eli Lilly, Lundbeck, Medscape, Novartis, Organon, Pfizer and Teva. Her research group has received research grants from AbbVie, Novartis and Teva, as well as Instituto Salud Carlos III, EraNet Neuron, European Regional Development Fund (001-P-001682) under the framework of the FEDER Operative Programme for Catalunya 2014-2020 – RIS3CAT; she has received funding for clinical trials from AbbVie, Amgen, Biohaven, Eli Lilly, Novartis and Teva. She is the Honorary Secretary of the International Headache Society. She is in the editorial board of Revista de Neurologia. She is an associate editor for Cephalalgia and Neurologia. She is a member of the Clinical Trials Guidelines Committee of the International Headache Society. She has edited the Guidelines for the Diagnosis and Treatment of Headache of the Spanish Neurological Society. She is the founder of ![]() . PPR does not own stocks from any pharmaceutical company.
. PPR does not own stocks from any pharmaceutical company.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.