
Abstract
Introduction
The international headache classification has been enormously important promoting research and clinical management of patients with headache. It is a living document that develops from edition to edition and changes have been increasingly based on research, so called classification research. The aim of the present review is to present recent results of such research and to characterize the methods available for it.
Methods
Published research was identified by systematic search of PubMed. Lists of references of identified articles and the table of content of the last five years of Cephalalgia were screened.
Results
The major results of identified articles are summarized. Thereafter the different methodologies applied in these studies are described. Finally, some suggestions are made for the future consideration of the fourth classification committee.
Conclusion
Classification research is emerging as an important avenue of headache research. It has a multitude of different designs available and many of them do not need advanced equipment.
Introduction
The first edition of the international headache classification, later known as the International Classification of Headache Disorders (ICHD-1) represented a revolution (1). It was more comprehensive, gave a more precise nomenclature and used all available literature. The most important step forward was the development of explicit— also called operational— diagnostic criteria for all the different types of headaches. These criteria were largely based on the opinion of the experts in the classification committee but have since proven valid when scientifically tested in many cases. Explicit diagnostic criteria have several virtues. They allow precise clinical diagnosis and reduce inter observer variability. Most relevant in relation to the aim of the present article is that they can be tested scientifically. Every item in a set of diagnostic criteria can be tested and the results of the testing can easily be included in revised criteria. Also, the larger aspects of the classification can be tested. Perhaps there is no supporting evidence for a diagnosis? And perhaps new entities need to be accepted? The ICHD-1 provided a platform from which further development and refinement was possible. Subsequent editions, ICHD-2, ICHD-3beta and ICHD-3 have been developed along these lines (2,3). They have been revised by gradual evolution and revolution has been avoided. Opinion of experts has continued to play a significant role for ICHD-2 and more so than for ICHD-3. Thus, changes have been increasingly based on published scientific studies, also called classification research. This has turned out to be a special subfield of headache research but a field that is still small and in development. Now it is ready for increased input, but what are the results so far? How should this kind of research be done? And what are the most burning questions to be answered in the future? ThosAnde are the questions addressed in the present narrative review which seems timely as the committee for the fourth edition of ICHD is beginning its work (4). The present study uses the literature somewhat selectively and can in no way replace an extensive literature search of each diagnostic entity for ICHD-4.
Methods
This review aimed to include all literature formally testing the ICHD-3beta and ICHD-3. It proved very difficult, however, to be comprehensive as no search term was ideal. Headache AND classification AND research resulted in 2579 hits, most which appeared irrelevant at a quick glance. Headache AND field testing resulted in 631 hits. They were all read by title. Headache AND classification resulted in 6456 hits, and ICHD AND field testing gave 137 hits. Headache AND field testing as well as ICHD AND field testing were all read by title and overlapping titles were deleted. Thereafter 52 articles were read, and 29 articles were selected for inclusion. Much classification research has originated from the Danish Headache Center. We therefore scrutinized the publication list from the Danish Headache Center 2015–2025 and included an additional 13 highly relevant articles that had not been retrieved from PubMed. As Cephalalgia is the most relevant journal for classification research the table of contents for the last five years was also scrutinized and from this search an additional 25 papers were included. In total, 67 articles were included in this review. The aim has been to include all studies that formally test one or more diagnostic criteria while purely descriptive studies have been included selectively. A careful search of the literature for each diagnosis of ICHD-3 was outside of the scope of this article but has, of course, to be done for the ICHD-4.
Results
In the following research results will be presented in the order of ICHD-3 starting with migraine. It is interesting and very important that the diagnostic criteria from 1988 for migraine without aura (MO) based on the opinion of experts remain unchanged in ICHD-3. The only serious challenge was the suggestion to include osmophobia in the criteria. Two different suggestions were tested in a large amount of material from systematically studied migraine patients against datalfrom patients with tension-type headache (TTH) (5). Osmophobia was a very specific symptom practically absent in TTH but had only a limited sensitivity. It did not add to the migraine diagnosis as all patients with osmophobia also fulfilled existing criteria for migraine accompanying symptoms. It was concluded that complicating diagnostic criteria by adding osmophobia was not warranted. Others found, however, that osmophobia should be part of the diagnostic criteria as an added associated symptom of migraine because of its extremely high specificity (6). The question thus remains open. (Figure 1).
Migraine with aura (MA) did not have diagnostic criteria at the second digit level in ICHD-2. This was developed for ICHD-3beta. A diagnosis at the second digit level must include all patients diagnosed at a lower level in the hierarchy. A large field-testing study showed that this was the case and the diagnostic criteria for 1.2 migraine with aura were included in ICHD-3beta (7). There was suspicion that these criteria would not sufficiently separate migraine with aura from transient ischemic attack (TIA) and appendix criteria were suggested in ICHD-3beta that might perhaps solve this problem. That proved to be the case as the appendix criteria performed better than the main body criteria tested against a large group of patients with transient ischemic attack (TIA) (8). Consequently, the appendix criteria were included in the main body of ICHD-3. The value of these criteria was confirmed in an independent German sample (9). The symptomatology of the migraine aura is very rich. Several studies have demonstrated this (10). Simplicity is, however, a principle of diagnostic criteria and the multitude of symptoms described do not require alteration of the existing diagnostic criteria without extensive formal field testing.
Basilar artery migraine first described by case stories was renamed basilar migraine in ICHD-2 because of lack of evidence for basilar artery involvement. In ICHD-3 it was renamed migraine with brain stem aura because all experts agreed that the symptoms had to originate in the brain stem. Nevertheless, uncertainty about the very existence of this type of migraine continued. Yamani et al. (11) analyzed all available literature and used a large amount of material from prospectively, questionnaire-diagnosed migraine patients and data from the Danish Headache Center. They concluded that migraine with brain stem aura does exist but that it is very rare, and they suggested tighter revised diagnostic criteria.
Chronic migraine (CM) is also a developing concept that started in ICHD-2 with very tight criteria followed by more open criteria published as an independent article (12). Finally, the criteria allowed medication overuse in ICHD-3. It remained an open question, however, if patients with 8–14 days of migraine (so-called high frequency episodic migraine or HFEM) should have been included in the CM criteria. Chalmer et al. provided evidence that HFEM patients were very disabled and in many aspects as disabled as CM using the unique Danish medication and social benefit data bases (13). Diagnostic criteria that united traditional CM and HFEM in a new CM concept were presented (Table 1).
Proposed new diagnostic criteria for chronic migraine (13).
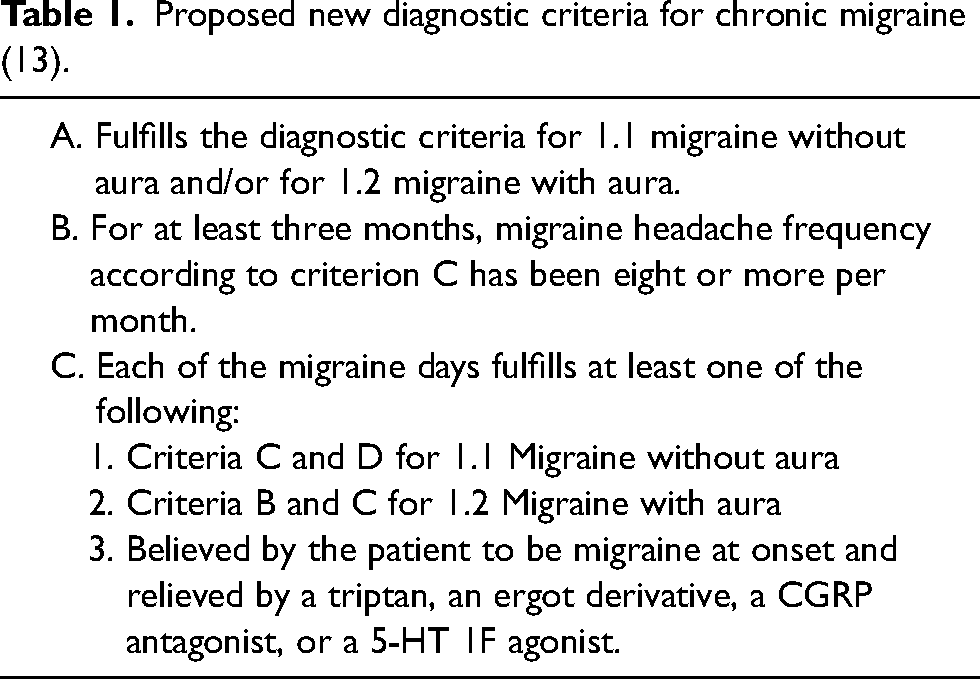
A further study from the US, the CAMEO study, supported that conclusion (14). Some concern was voiced about reimbursement possibilities for such an expanded concept of chronic migraine (15). Very recently an extensive narrative review also showed a considerable impact of HFEM, greater than for low frequency migraine (LFEM) (16). It suggested that HFEM should perhaps be a separate subdivision of migraine but disregarded that further subdivision of migraine would be impossible because the classification already subdivides in MO and MAand its sub forms. It had been possible to separate out CM because CM is a conglomerate of MO, MA and other headaches but that would not be possible for HFEM.
Tension-type headache (TTH) was divided according to frequency of attack in ICHD-2 and a little differently in ICHD-3, but no research has appeared to support or contradict this subdivision, and it remains an opinion of the experts of the classification committee. Each of the three subdivisions have also been divided according to tenderness of pericranial muscles. A meta-analysis confirmed the high prevalence of tenderness of pericranial muscles. In chronic TTH tenderness was found both cranially and outside the head while in episodic TTH it was restricted to the pericranium (17). The borderland between TTH and temporomandibular disorder (TMD) is interesting but remains insufficiently studied. It raises a question about the relation between primary and secondary headaches. During the development of ICHD-3 the relation between TTH and MO was debated. The current diagnostic criteria for episodic TTH allow photo- or phonophobia but not both and for chronic TTH mild nausea is also accepted. Appendix criteria suggested that TTH should not have any accompanying symptoms at all. This was tested in a large amount of material randomly selected from the general Korean population. Of the participants who fulfilled the ICHD-3 diagnostic criteria for TTH only half fulfilled the strict appendix criteria (18). Because TTH is so prevalent, the appendix criteria would leave 20–30% of the population to receive a diagnosis of probable TTH or probable MO. This would be unsatisfactory because a general rule demands that probable diagnoses should be as few as possible. It is an important future task to study patients fulfilling ICHD-3 criteria but not appendix criteria.
In ICHD-3beta fullness in the ear and forehead/facial flushing were added to the diagnostic criteria for cluster headache based on the opinion of experts. The value of this was tested in a large Dutch cohort (19). It found no evidence supporting the addition of these two symptoms. Since data always trump opinion, the two symptoms were not included in the ICHD-3. A further study supported this decision (20). A systematic review and meta-analysis described the epidemiology of short lasting unilateral neuralgiform headache attacks (SUNHA), a term including short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA) which were distinguished in ICHD-3. According to the review the differences between SUNCT and SUNA were minimal, and it was suggested to no longer distinguish but to just diagnose SUNHA (21). Unfortunately, that term is uninformative. Differences in therapeutic responses may differ and the issue of lumping is still debated. An extensive review described paroxysmal hemicrania and hemicrania continua with a focus on their borderlands. It did not suggest altered diagnostic criteria (22). A systematic review and meta-analysis emphasized that hemicrania continua has been relatively poorly characterized and suggested more systematic study in the future (23).
Chapter 4 of ICHD-3 on other primary headaches was considerably expanded and revised, often based on excellent published case series. Of 83 consecutive patients with cough headache 10.8% were secondary to intracranial disease (24). The duration, characteristics, associated features and location in primary cases were specified. Imaging was necessary to separate primary and secondary cases and should perhaps be included in the criteria of a future revision. In a respiratory clinic the prevalence of primary cough headache was 18% while in the former clinic-based study it was only 1% (25). Headache associated with sexual activity was described in 245 patients (26). Only 15.5% had primary sex headache while 71% had reversible cerebral vasoconstriction syndrome (RCVS) and 10.6% had probable RCVS. It was not possible to separate these diagnoses clinically. The results suggest that imaging should perhaps be included in the diagnostic criteria in future. The further relation to primary thunderclap headache was discussed in a review (27). It was again pointed out that, especially with two or more attacks, thunderclap headaches are caused by RCVS in most cases. Imaging in the acute stage should always be repeated two weeks later. These high prevalences of RCVS have not been reported in Caucasian patients. Methodological or racial differences in the prevalence of RCVS should be studied in future. Studies of many aspects of the ICHD-3 in different parts of the world are needed, like what has happened to the epidemiology of headache disorders.
An extensive questionnaire study among students and staff of a university analyzed the clinical features of headache attributed to ingestion or inhalation of a cold stimulus (Table 2).
Characteristics of headache induced by cold compared to the diagnostic criteria in ICHD-3 (28).

The data suggested that duration and location might differ from the ICHD-3 diagnostic criteria, but alternative criteria were not presented (28).
Of 280 patients with stabbing pain only seven had a secondary cause and the rest met the diagnostic criteria of ICHD-3beta for primary stabbing pain. Only 22 patients met ICHD-2 criteria illustrating the improvement from ICHD-2 to ICHD-3 (29). Hypnic headache was analyzed in 17 prospectively studied patients of whom 11 also underwent polysomnographic investigation. ICHD-2 criteria were not fulfilled by 35% (30). Hypnic headache occurred equally in REM and non-REM sleep. Two meta-analyses included 250 and 348 cases, respectively (31,32). The first study showed that the diagnostic criteria of ICHD-3beta were better than the criteria of ICHD-2 (31). The other meta-analysis gave very precise clinical characteristics which could also have been used to analyze the diagnostic criteria but were not (32). Finally, hypnic headache received a systematic review and meta-analysis which demonstrated a considerable between-study heterogeneity (33).
In ICHD-1 diagnostic criteria for secondary headaches demanded that the headache disappears or greatly diminishes after remission or successful treatment of the secondary cause. In clinical practice it is, however, necessary to give a diagnosis at the first patient encounter or soon after. Therefore, general diagnostic criteria that did not require remission were introduced in ICHD-2 and ICHD-3 (34). The need for this change was felt to be so obvious that it was introduced based on the opinion of experts. In contrast, revision of the general diagnostic criteria for secondary headaches of ICHD-3 has been suggested based on a large amount of material on ischemic cerebrovascular disease and controls (35). It included headache of a new type never encountered before and headache of a previous type but with significantly altered characteristics. Headache of a previous type without significantly altered characteristics was not considered secondary (Table 3).
Proposed general diagnostic criteria for secondary headaches (35).
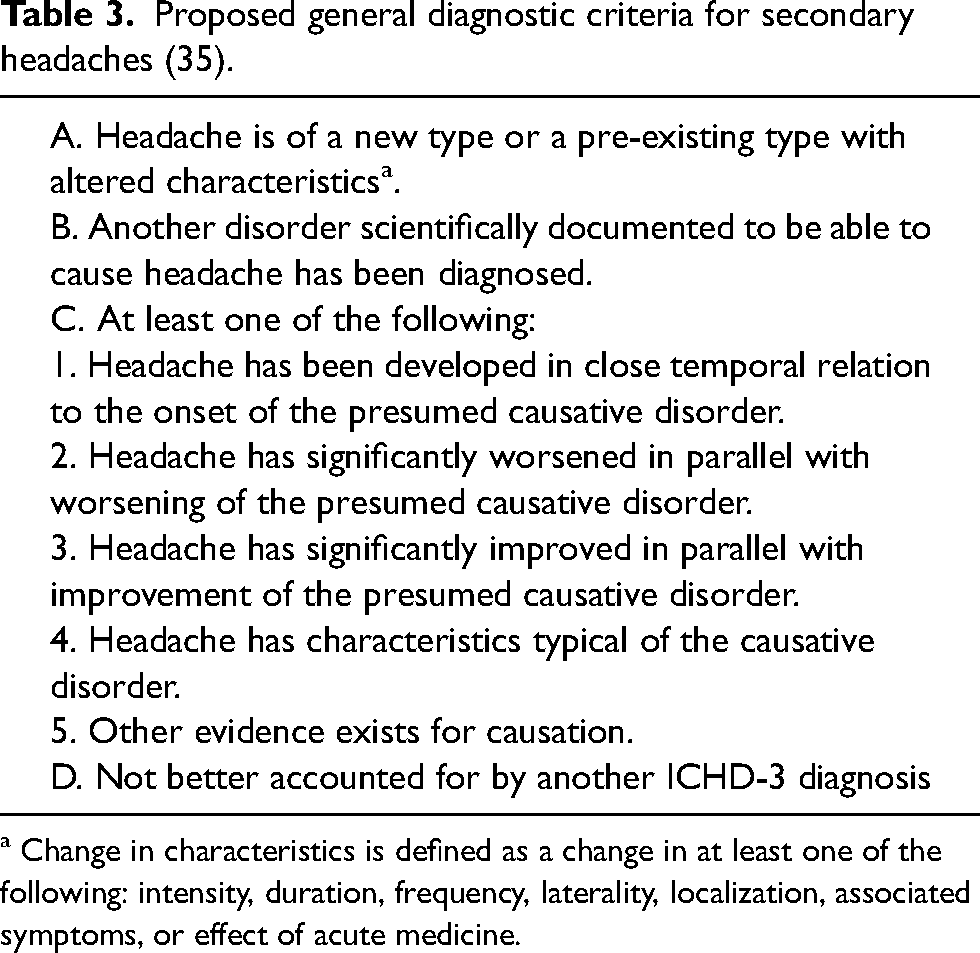
a Change in characteristics is defined as a change in at least one of the following: intensity, duration, frequency, laterality, localization, associated symptoms, or effect of acute medicine.
Emergency room patients with concussion (N = 302) were interviewed one week after admission. Of these, 92% endorsed headache and 94% of those had onset within 24 h. Headache was mostly constant but nausea, photo- and phonophobia were frequent. The ICHD-3 criteria were reasonable with a possibility to strengthen the onset criterion to one day rather than one week (36).
The diagnostic criteria of the ICHD-3 for headache attributed to transient ischemic attack and the criteria for headache attributed to ischemic stroke were tested in a large amount of material from such patients compared to a large amount of control material (37,38). Neither performed well and revised criteria for both TIA and ischemic stroke were proposed. Diagnostic criteria for sentinel headache before stroke were also suggested for the first time.
ICHD-2 included only a few diagnoses of persistent headache attributed to a secondary cause. A small study showed that headache often persists for more than three months after carotid artery dissection (39). The results were later confirmed and expanded in a large study (40). A long-term follow-up study showed persistent headache after dissection in 22.5% after 2.5 years (41). The above-mentioned material of ischemic stroke and controls as well as another cohort study showed that headache also attributed to ischemic stroke persists in a significant number of patients (42,43), often leading to medication overuse and causing considerable reduction of quality of life. Persistent headache attributed to cerebral venous thrombosis was described in a follow-up interview. After 1.1 years on average 59% still had headache believed to be attributed to past thrombosis (44). To prove the entity a future prospective study was recommended. A suitable control group would greatly strengthen such a study.
The criteria for reversible cerebral vasoconstriction syndrome headache were evaluated in two large consecutive series of patients at one center. First an epidemiological description was given based on 138 patients (45) and then the ICHD-3beta criteria were evaluated in a further 99 patients (46). Some criticisms of the diagnostic criteria were mentioned. No specific suggestions for revised criteria were made but criteria were revised between ICHD-3beta and ICHD-3 possibly based on these results. Headache attributed to cranial venous sinus stenting was described as a possible new entity in a series of 47 patients (47). It could be a candidate for inclusion in the appendix of ICHD-4 or even main body if confirmed in a separate study.
A prospective study of patients referred on suspicion of idiopathic intracranial hypertension (IIH) compared those in whom the diagnosis was confirmed to those where it was ruled out (48). Aggravation by coughing or straining, relief after cerebrospinal fluid (CSF) withdrawal and retrobulbar location were headache features statistically more frequent than in the control group. Revised diagnostic criteria were suggested but they included non-headache features typical of IIH. A subsequent study from the same group followed the same design in an even larger group of patients (49). It could not confirm a difference between IIH and control patients regarding straining but did not ask about coughing or retroorbital location while the effect of CSF withdrawal was confirmed. It concluded that headaches associated with IIH were often migraine-like and sometimes TTH-like. Thus, the headache did not have special characteristics. They suggested that the headache should be defined as headache of a new kind or of a previously encountered kind that had significantly worsened in association with other symptoms of IIH. Considering the above-mentioned differences, it may still be discussed whether it is possible to include headache characteristics in the diagnostic criteria. According to ICHD-3 the diagnostic criteria for secondary headaches can be included in three different ways. If there are no typical features of the headache, any headache should be mentioned, if there are such differences they should be included in order to guide clinical evaluation and if the headache is actually typical in itself, as seen for example with headache attributed to low intracranial pressure, that should be specified. The latter was examined in a prospective study of patients with orthostatic headache (50) (Figure 2).
The data could perhaps strengthen ICHD-3 diagnostic criteria but that was not specifically proposed.
The relation between epilepsy and headache has a long history but its importance seems to have dwindled over recent decades. Only one prospective diary-based study has examined headache attributed to epileptic seizure (51). It tested the diagnostic criteria of ICHD-3beta. The main conclusion was that headache during or following epileptic seizure is rare. Headache shortly before seizure was more frequent. A future study should include a normal control group recording at the frequency expected in the epileptic group. Sturge-Weber syndrome is associated with a high prevalence of headache (52). Explicit diagnostic criteria were not suggested. Chiari 1 malformation is associated with both typical occipital- and a non-typical headache (53). The syndromes were described in detail, but evidence of causality remains weak with a risk of surgical overtreatment. In a systematic review of cardiac cephalalgia (CC) all published cases and case series were analyzed (54). Reported clinical features were compared to the diagnostic criteria of ICHD-3. The headache features described under criterion C3 did not find sufficient support in the literature. Subsequently the same authors reported 54 consecutive patients with CC (55). The results showed that the headaches very rarely had a migraine phenotype. Furthermore, the diagnostic criteria could be simplified by removing criteria C3 and C4 as they did not add to the diagnosis. Coronary intervention can apparently also cause headache (56). Like most other case series this study also lacked a control group which makes it difficult to estimate causality. Postural tachycardia syndrome (POTS) according to a systematic review and meta-analysis was associated with migraine-like headache in 36.8% of cases (57). The acute episodes make a random co-occurrence highly unlikely. A control group was missing in the reviewed studies. It would have strengthened the case. Airplane headache was included in the main body of ICHD-3 based on a very characteristic clinical picture described in case series. A much larger study of 50,000 passengers showed, however, that several of the features included in the ICHD-3 diagnostic criteria were not accurate (58). Revision of the criteria based on this recent study was suggested but no revised set of criteria was presented.
A good example of field testing is a study of classical trigeminal neuralgia (CTN) (59). An important differential diagnosis is primary idiopathic facial pain (PIFP). Material from 37 such patients was compared to 206 consecutive patients with CTN. Both sensitivity and specificity were unchanged between ICHD-2 and ICHD-3beta. It was concluded that sensory abnormalities should not by themselves rule out the diagnosis. Modified criteria were suggested and partly considered in ICHD-3. Occipital neuralgia is a somewhat disputed entity. A meta-analysis and systematic review showed high heterogeneity and a need for population-based study (60). Recurrent painful ophthalmoplegic neuropathy previously called ophthalmoplegic migraine was systematically reviewed (61). The authors proposed specific changes to the ICHD-3 diagnostic criteria.
The appendix was originally thought to be for diagnoses on the way out of the main body of the classification because of insufficient evidence and for diagnoses on the way in. Alternative criteria from those of the main body were also placed in the appendix for future comparison with main body criteria. One study found for example that the appendix criteria were superior (8) and another that the main body criteria were best (5).
There have been many suggestions for further subdivision of migraine, but none were accepted because they would have to be applied to all subtypes of migraine and therefore would make the classification too complicated. On the other hand, there is a need to study menstrual migraine, sensitizing migraine patients, migraine patients with autonomic symptoms and several other subtypes of migraine. The solution is to give explicit diagnostic criteria for all interesting subtypes of migraine (possible endophenotypes) in the appendix available for scientific study. The ICHD-3 appendix criteria for menstrual migraine were tested in a very large amount of material from blood donors roughly representative of the Danish population (62). Problems with high frequency- and chronic migraine in menstrual related migraine were quantified. These serious problems were solved by proposed revised diagnostic criteria. The same for pure menstrual migraine in patients with relatively rare attacks. Pure menstrual migraine was observed in a quarter of patients with menstrual migraine. In contrast another study found pure menstrual migraine to be extremely rare (63). It included patients from a tertiary headache referral center, many with chronic migraine or high frequency episodic migraine. Therefore, it may have underestimated pure menstrual migraine. It demonstrated a considerable discrepancy between headache history and headache by prospective questionnaire recording and recommended the latter. It is a general principle of ICHD, however, that diagnostic criteria should allow diagnosis at the first patient encounter or immediately after the necessary work-up. That would be impossible with prospective questionnaire diagnosis. For scientific study of mechanisms, it may be preferable to have a prospective diary confirmation of menstrual relationship but even then, such a long prospective recruitment period seems difficult. Another possible endophenotype is migraine with autonomic symptoms. Its prevalence varies much in previous studies. How many autonomic symptoms should be recorded? How severe should they be? Should they locate to the side of unilateral migraine? In what proportion of attacks should they occur? These questions have not been answered. The best attempt used questionnaires as well as interview characterization of a large amount of population-based material (64) (Table 4). It suggested diagnostic criteria based on questionnaires for genetic studies and other studies requiring large numbers of patients and stricter criteria for clinical and pathophysiological studies (Figure 2). These criteria are not perfect but a good stepping-stone for future investigation. Other subdivisions such as sensitization should be studied with similar methodologies.

Osmophobia is a very specific symptom of migraine and hardly exists in tension-type headache. Left bars show percentage of attacks with osmophobia and right side bars show percentage of patients having osmophobia during at least one of four observed attacks (6).

Exact measurement of on- and off time of headache attributed to spontaneous low intracranial pressure (50).
Proposed diagnostic appendix criteria for migraine with cranial autonomic symptoms for use in genetic and epidemiological studies (64).

Vestibular migraine is a diagnosis that has been used often without much scientific backing. It was positive that specialists from the Barany society and the headache classification committee together proposed diagnostic criteria sufficiently explicit to be field tested in contrast to previous very relaxed criteria (65). Since the parallel publication of these criteria in the ICHD-3 and in the otological literature there has, unfortunately, been no field testing of the criteria. Studies of patients diagnosed with these criteria have been done (66) but that does not diminish the need for testing the criteria.
Research methodology
In the following it is attempted to distinguish between the different research methodologies used to improve headache classification.
It is still possible to identify logical flaws in the classification. A previous example is the change of general diagnostic criteria for the secondary headaches from ICHD-2 to ICHD-3 (34). It was simply obvious that the former did not allow a definite diagnosis at the first patient encounter while the revised criteria did. To allow changes based only on logics, it is important that committee members agree, and the criteria should subsequently be tested. A logical flaw may also be identified and then scientifically evaluated. ICHD-3 diagnostic criteria for pure menstrual migraine could not diagnose patients with rare attacks. The existence and quantity of such patients was then confirmed in a large patient material and revised diagnostic criteria were suggested (62). The simplest method in classification research is to describe a possible new entity in the case story format. If the new type of headache is very rare a single case may be the only possibility but normally at least two, three or more cases are necessary for a publication (47). The publication of one or a few cases can trigger similar reports from other parts of the world so that the knowledge base is gradually increased. The diagnostic criteria of any of the existing headache disorders must not be fulfilled and the cases should have distinctive features allowing the construction of proposed explicit diagnostic criteria. With enough cases and small series published, a meta-analysis of all existing evidence is appropriate despite the inherent problem of heterogeneity of included studies. Existing diagnostic criteria should be tested against the clinical data from the meta-analysis. Revised explicit diagnostic criteria should be proposed as the result of such a study, but existing studies often present only the statistical data (32). Better than a meta-analysis is a large series. It can be done single center or multi-center if the headache is rare. The same protocol should then be used in all participating centers. No good examples of such a multi-center study of a classification have, however, been published. A single center study benefits from homogeneity but the material is less representative than in a multi-center multi-national study. Excellent studies from Korea may for example not be representative of Caucasians and vice versa (26,29). A controlled clinical study can be regarded as the gold standard of classification research. In headaches with a relatively acute onset comparison can be made to a normal control group. The above-mentioned studies of ischemic cerebrovascular disease are good examples (38). In such studies a large series of cases is collected in parallel with normal or near normal control material. Headaches that occur in patients but considerably less in controls must be caused by the disease. An ICHD-3 type of headache can also be compared to the most important differential diagnosis. This was for example done in the studies of migraine with aura compared to TIA (8) and trigeminal neuralgia compared to primary idiopathic facial pain (PIFP) (59). IIH was compared to patients who were referred for IIH but did not to have it (49).
Discussion and future challenges
Considering the importance of the international classification of headache disorders, the ICHD, it may surprise that research to improve it does not have more volume as shown in the present review. It is not difficult to get such studies published as Cephalalgia, the official journal of the International Headache Society and the home of the ICHD classifications, has shown interest in such studies. It is also a kind of research that does not need very expensive equipment. Classification research may, however, be a challenge conceptually. Hopefully the present review may clarify the concepts and stimulate further classification research.
It is often argued that classification research represents circular reasoning because patients are diagnosed according to existing criteria and therefore cannot easily be used to revise the same criteria. The argument overlooks the fact that diagnostic criteria must not only be sensitive and specific, but also as simple as possible and therefore use only the necessary parameters. Other parameters typical of a kind of headache are often not included. The criteria preferably use clinical features available at the bedside. Imaging results, biochemistry, heredity, drug response, age and other data that are not usually part of the diagnostic criteria but can contribute to research characterization of cases. Thus, having collected a large series of patients and controls all these other parameters should be evaluated. Both the patient group and the control group will then have cases that are misdiagnosed by ICHD-3 criteria. Alternative diagnostic criteria can then be developed and compared to ICHD-3 criteria for sensitivity and specificity. In this way research spirals up and is not circular. Every round of research lifts the quality of the criteria.
There is always discussion between “lumpers” and “splitters”. The former want to have as few diagnoses as possible and have for example suggested to lump migraine and tension-type headache according to a continuum severity model as well as lumping migraine with and without aura. Subsequent research has, however, shown marked differences between these disorders supporting the separation in ICHD. Thus, the desire for simplicity of the “lumpers” has sometimes disregarded important differences. Splitting can also be wrong. In extreme cases it can lead to so many different diagnoses that the classification becomes impractical. For clinical use the already considerable size end detail of ICHD-3 is dealt with by the hierarchical format allowing clinicians to diagnose only at the first or second digit level. An example of splitting is to classify headache in every single type of infection. That would be an enormous task and totally out of proportion in relation to the importance of the topic. The balance between splitting and lumping has been fine-tuned during years of discussions in former classification committees and this will probably continue.
What are the most obvious needs for classification research in the future? Many entities in ICHD-3 still need analysis in large and preferably representative case series. Most obvious is the need in secondary headaches. For each secondary cause it is necessary as a minimum to know patients’ past headache history (migraine or TTH), characteristics of the presumed secondary headache, whether it is of a new type or a past headache and whether it has or does not have significantly altered characteristics. What alterations of characteristics are needed to show causality? That will differ between different types of secondary headache, and it has only been studied in a few types (35,37,38). Relevant parameters are frequency, severity, location, character, time course, response to drug treatment and probably more. Patients’ own feeling that a headache is different from previously should also be considered.
A more comprehensive list of suggestions for future classification research has been given by the present author in a recent paper on the history and future of headache classification (67).
The main problem of classification to solve in future is that ICHD-3 is based almost exclusively on clinical parameters. The need for biomarkers is pressing but difficult to meet. There are several studies of genetics, imaging, biochemistry and neurophysiology that suggest their use, but they are only able to distinguish migraine from normal in relatively large groups of patients. What is needed is of course distinction at the individual level. It would not need to be absolute. Parameters with say a 50% difference in prevalence between migraine and non-migraine individuals could perhaps be used as part of polythetic diagnostic criteria. But the same difference would also have to be present between migraine and other kinds of headache. Significant future development in technology seems necessary before the dream of including biomarkers can be realized in the classification of headache disorders.
Conclusions
The international headache classification ICHD has developed significantly from edition to edition. Even after ICHD-3 a lot remains, however, to be studied. The volume of classification research is not impressive but enough high-quality studies cited here can serve as examples for the future. The results and methodologies are summarized in this review in the hope that the interest in classification research may increase in the future.
Headache classification is crucial for accurate clinical diagnosis and effective patient management. Standardized classification methods can significantly improve research quality and consistency. Future revisions to headache classification should be supported by scientific research and evidence.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.O.: Owns stock in the following companies: Alligator Biosci, Cephagenix, Moberg Pharma, Novo Nordisk, H. Lundbeck.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.