
Abstract

Introduction
The International Classification of Headache Disorders (ICHD) was first published in 1988, with a second edition in 2004 and finally a third edition beta version in June 2013 (1). There are no competing classifications and the different editions have been translated into all major languages of the world, resulting in global distribution and global use. Each of these editions represents a huge effort involving more than 100 experts and each has taken three years to develop. In an iterative process the classifications have gradually been improved, solving problem after problem. Classification research has slowly emerged as a branch of the headache sciences and has developed both quantitatively and, more important, qualitatively. A reasonable amount of good studies were available for the third edition.
Despite all these efforts, there are still unresolved issues. As chairman of all three editions, I feel a need to focus on what I consider to be the most important problem areas that remain unsolved in ICHD-3 beta. This beta version is meant for field testing over a three-year period so that a final edition may be published in 2016. It is possible, therefore, to solve some of the problems I am going to raise before the final ICHD-3 is published. On the other hand, the unsolved issues are really very difficult and several of them may not find their resolution this time but will be left for a future ICHD-4 and a future classification committee.
Migraine
A problem area in migraine patients continues to be headaches that do not fulfill migraine criteria but fulfill criteria for tension-type headache (TTH). Previously the term interval headaches was used. Increasing evidence suggests that they are often, but not always, mild migraine attacks. In the rules for how to use the classification it is specified that one possibility is to make a diagnosis of migraine, which requires just five attacks fulfilling criteria. Another is to count the number of attacks. Here also less-typical attacks may be counted such as attacks treated before full development of migraine symptoms or attacks fulfilling only criteria for probable migraine. These problems probably require biomarkers for their final solution. The same pertains to patients who never fulfill criteria for migraine but do fulfill criteria for probable migraine and criteria for TTH. Today the default rule is to code for the entity for which criteria are fulfilled and not for the entity for which only the probable category is fulfilled. Without biomarkers it is probably impossible to do better.
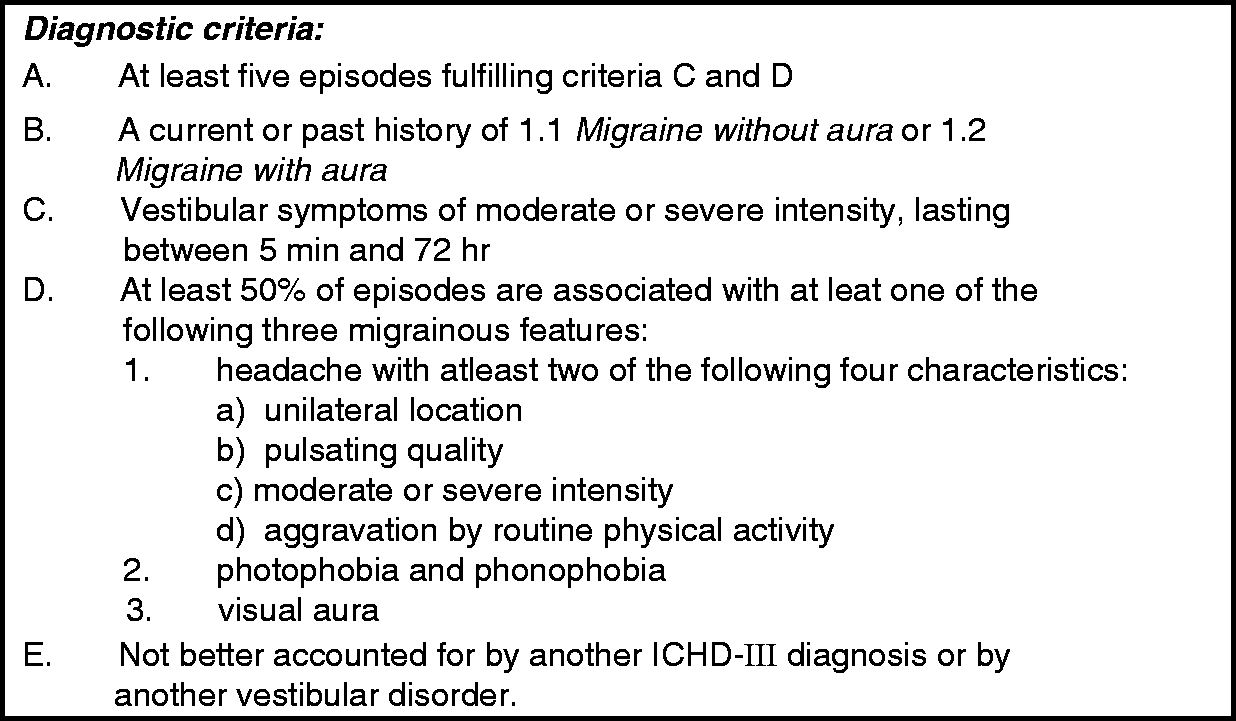
We have shown that the diagnostic criteria for 1.2.2 Migraine with Brain Stem Aura (Figure 1), when taken literally, include too many patients. Neurologists generally consider this diagnosis to be very rare. Another problem is the distinction between migraine with brain stem aura (previously basilar migraine, basilar artery migraine) and A 1.6.5 Vestibular Migraine, for which diagnostic criteria have now been provided in the appendix (Figure 2). There is no doubt that many headache patients fit into both sets of criteria and this is unacceptable. One kind of headache should be diagnosable in one and only one place of the classification. Unambiguous diagnostic criteria for retinal migraine were presented already in 1988 and subsequently in 2004. Not a single paper has, however, documented the existence of retinal migraine with reasonable certainty. If no further research studies are conducted documenting this entity then it should be displaced to the appendix or deleted. Chronic migraine has been included in the main body of the classification with unambiguous diagnostic criteria. It is of course quite arbitrary to single out this segment of severely affected patients because migraine is a continuum of severities. However, the distinction between chronic and episodic TTH made already in ICHD-1 was equally arbitrary but, nevertheless, proved useful. So is also the diagnosis of chronic migraine likely to be. A positive response of chronic migraine to botulinum toxin A is so far the only clinically useful aspect of chronic migraine. Future research must focus on differences between chronic and episodic migraine. The criteria are based on the opinion of experts and it is difficult to field test them in the absence of biomarkers, imaging results, genetic differences or other validation factors but it should be attempted.
1.2.2 Migraine with Brain Stem Aura. A1.6.5 Vestibular Migraine.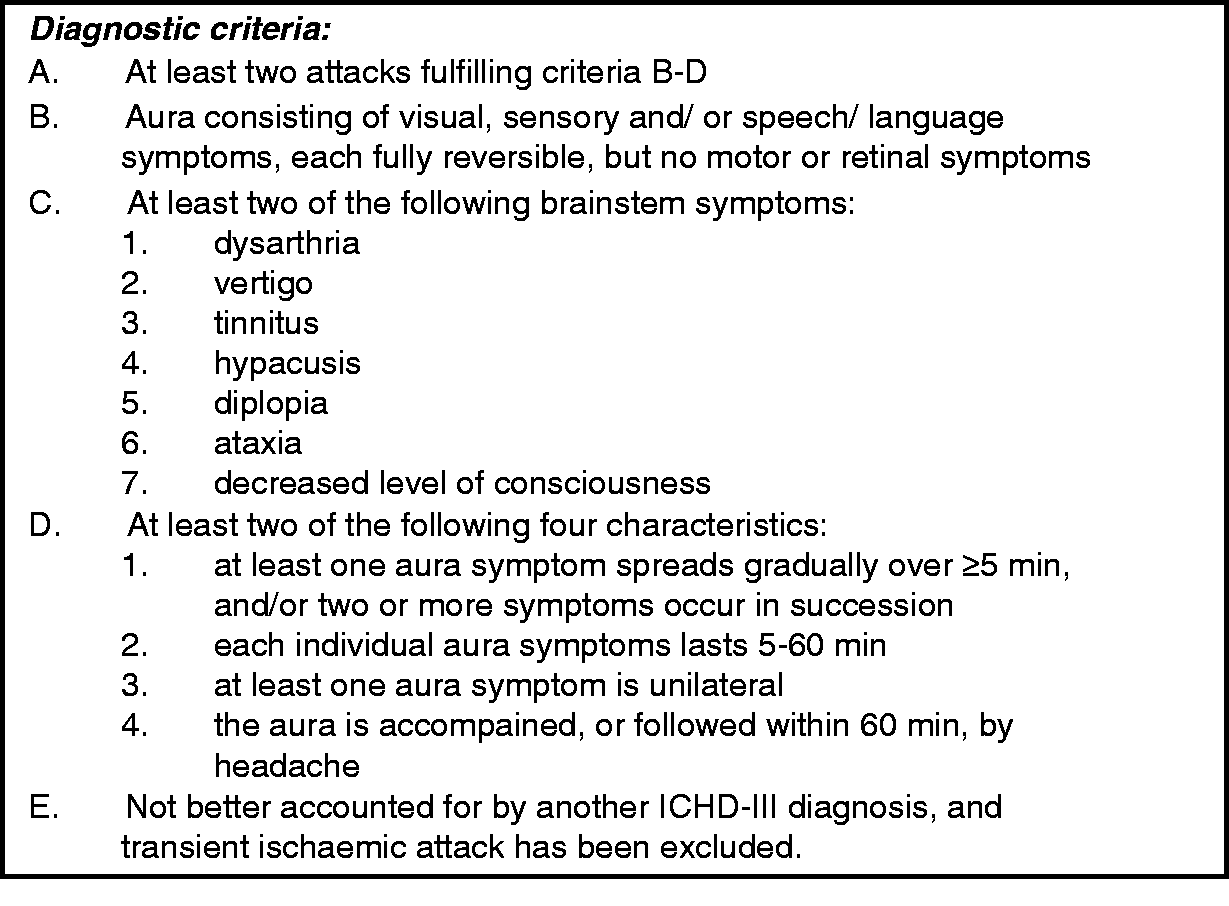
TTH, cervicogenic headache and temporomandibular disorder (TMD)
TTH is generally accepted as the most common type of primary headache, and diagnostic criteria for TTH have not changed appreciably over three editions of the classification. A big problem is, however, that this headache is relatively featureless and that there are no biological markers to help in the diagnosis. Little research has been conducted in TTH in recent years and there is not a single drug registered for the prophylaxis of TTH. As it is, the diagnostic criteria are rather open and basically characterize a headache without migraine characteristics and without any known cause. It is subdivided into a type with and a type without pericranial muscle tenderness. This tenderness can be located in the chewing muscles or the neck muscles or in their tendon insertions. The diagnostic criteria for 2.2 Frequent Episodic Tension-Type Headache are given in Figure 3.
2.2 Frequent Episodic Tension-Type Headache.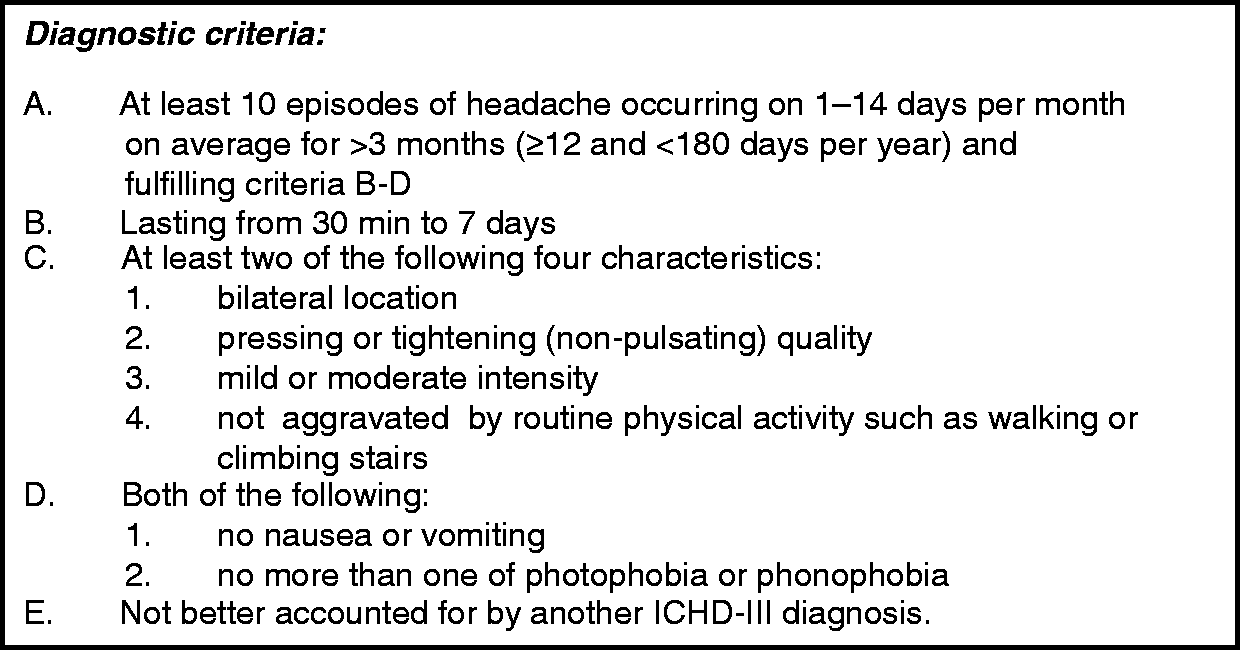
Cervicogenic headache is likewise featureless and is considered to be caused by a cervical disorder or lesion (Figure 4). Effect of diagnostic blocks is a supporting criterion but blockade of trigger points is also effective in migraine and TTH. Side-locked pain is mentioned in the comments but TTH is often half-sided. Provocation by digital pressure on neck muscles or by head movements are also mentioned in the comments but are also typical in TTH. It is mentioned in the comments that, when cervical myofascial pain is the cause of the headache, it should probably be coded as a TTH. In the appendix there are, however, criteria for cervicogenic headache attributed to cervical myofascial pain. Undoubtedly patients with tenderness of cervical muscles could be coded both to cervicogenic headache (perhaps only the appendix criteria) and to TTH. Elsewhere the classification takes great care to avoid one headache fitting two different sets of criteria.
11.2.1 Cervicogenic Headache.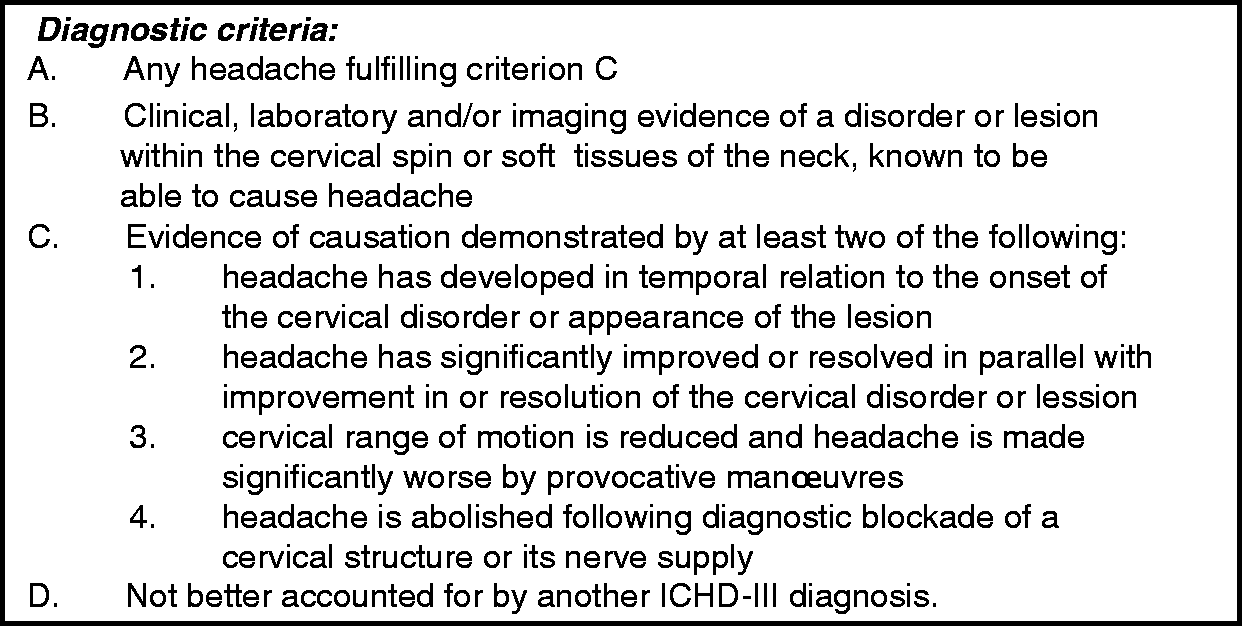
Headache attributed to TMD poses even worse problems. Diagnostic criteria are shown in Figure 5. This is also a featureless headache. The evidence of TMD relies on a temporal relationship that is usually difficult or impossible to ascertain. A key feature is that headache is produced or exacerbated by active neck movements, passive movements and/or pressure on the temporomandibular joint (TMJ) and surrounding muscles of mastication. There is no requirement for specified disorders of the TMJ. It is, thus, fully possible for a patient to fulfill these criteria with nothing but myofascial tenderness in the masticatory apparatus. In the comments it is mentioned that when the diagnosis of TMD is uncertain then the patient should be diagnosed as TTH but it is admitted that there is a big overlap and that the diagnostic criteria are not able to distinguish between TTH and headache attributed to TMD. A patient with TTH and predominant tenderness of chewing muscles would probably be diagnosed as TMD by a dentist and TTH by a neurologist. Again, this is highly unsatisfactory.
11.7 Headache Attributed to Temporomandibular Disorder (TMD).
It is clear to the present author how, at least partly, to solve these problems but there are strong opinions in opposite directions. In my opinion the diagnostic criteria for cervicogenic headache and TMD in ICHD-3 beta have been loosened too much. There should be specific requirements of definite organic abnormalities in the neck or in the TMJ other than myofascial tenderness in order to diagnose cervicogenic headache and TMD, respectively. In this way all headache patients who have myofascial tenderness and/or reduced range of movement, etc as the only abnormality would be coded as TTH. A patient would get one and only one diagnosis for his or her disorder because it would be obvious to the physician/dentist which diagnosis to use. If this were effected, then it might be considered to subdivide TTH into patients with tenderness predominantly in the masticatory muscles, patients with tenderness predominantly in the neck muscles, patients with diffuse tenderness and patients without increased tenderness. One problem remains, however, in relation to TMD. Many, if not most, patients experience pain only in the face and/or around the jaw joint and do not have headache. This is typical with predominant tenderness in the masseter muscle or the medial pterygoid muscle. Such patients should have the diagnosis of TMD but not the diagnosis of headache attributed to TMD.
Trigeminal autonomic cephalalgias
Very little has been changed in this chapter over the years. One persistent problem that remains unsolved is the use of the word chronic for cluster headache without attack-free periods. The word chronic in ICHD-2 was used with three different meanings. Chronic migraine and chronic TTH essentially meant frequent. Chronic cluster headache meant without attack-free periods, and chronic secondary headaches meant headache persisting more than three months after the causative disease. During the development of ICHD-3 beta it proved completely impossible to find a better word for chronic migraine and chronic TTH and these terminologies were kept without much discussion. We replaced the word chronic with persistent in the secondary headaches but the word chronic for cluster headache was not replaced. It should have been, in the opinion of the present author. The terms remitting and non-remitting cluster headache were proposed and would have been an improvement. The argument for keeping chronic cluster headache was that the diagnosis was too well embedded. This is not a good argument, in my opinion. The previously used term common migraine was, for example, replaced by migraine without aura (MO), despite the fact that it had been in use for many years. Another problem is that the diagnostic criteria for cluster headache have never been field tested. They are rather lengthy and there are perhaps more features mentioned than necessary. If proper field testing were conducted, it might be possible to simplify the diagnostic criteria without sacrificing sensitivity or specificity. Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) is an exceedingly rare kind of headache. Short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA) includes SUNCT and is only slightly more common. Suggestions to delete the SUNCT version were not accepted. Very few neurologists know or accept the difference between the two syndromes, and recently a report has suggested that they are part of the same continuum (2). Field testing and simplification seems warranted.
Other primary headache disorders
This chapter is perhaps the best example of revisions performed on the basis of thorough clinical research. Existing criteria as well as alternatives were tested in large numbers of patients leading to the revised criteria, which very likely have improved sensitivity and specificity. Without having the necessary material to prove it, it seems a problem to me that almost all the criteria are monothetic. This means that only one feature is mentioned and it must be fulfilled in order to get the diagnosis. The alternative, polythetic criteria, require, for example, two of four or one of three subcriteria fulfilled. This allows inclusion of all available evidence, even clinical features that are seen in only, for example, half of the patients. Let us just analyze a single set of diagnostic criteria and remember that the same reasoning can be applied to many of the other diagnostic criteria in this and other chapters. The criteria for 4.9 Hypnic Headache are given in Figure 6. Criterion A should ideally require a specific number of attacks but now requires “recurrent headaches,” not a specific criterion. Criterion C requires that headache must be present on more than 10 days per month for more than three months. But some otherwise typical patients may have headaches on fewer than10 days per month and some may have had it for only two months. Criterion D requires duration to be ≥15 minutes and ≤4 hours after awakening. Some patients may perhaps have longer-lasting headaches. It is also required that there should be no cranial autonomic symptoms or restlessness but maybe some patients have restlessness. The problem is seemingly solved by the probable category, which requires fulfilling all criteria but one. It is important, however, to have as few patients as possible in the probable categories. As mentioned, the present criteria are a big step ahead but if some of the criteria were made polythetic it could perhaps improve the criteria even more. It would be very interesting to see scientific studies testing polythetic criteria in a large number of patients with suspected hypnic or other primary headache. The diagnostic criteria for new Daily Persistent Headache lack a criterion saying: “No identifiable cause of the headache.” As it is now only the last general exclusion criterion prevents secondary causes.
13.1.1 Classical Trigeminal Neuralgia.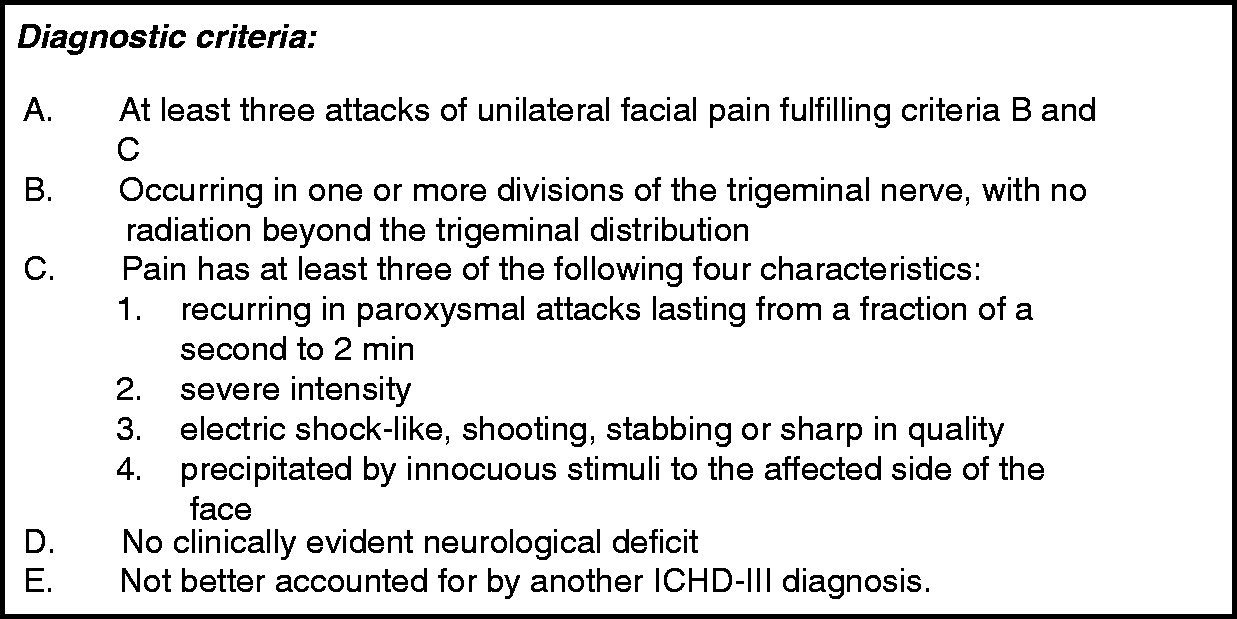
Headache attributed to trauma or injury to the head and/or neck
The first diagnosis in this category is called “acute headache attributed to traumatic injury to the head.” This is such a lengthy, clumsy diagnosis that doctors probably will continue to use the previous diagnosis “acute post-traumatic headache.” On the other hand these lengthy diagnoses are more precise. This raises a general problem in the headache classification of lengthy diagnoses. Abbreviations are obviously the answer here and this has been established in many other fields of medicine, for example, cardiological diagnoses referring to the affected arterial segment. The Headache Classification Committee should probably develop a list of authorized abbreviations of headache diagnoses, preferably acronyms that can be spoken.
Missing in this chapter is headache attributed to insignificant head trauma. We are not talking about mild head injury but about really insignificant traumas such as patients who have banged their head into a shelf raising up from a sitting to a standing position, patients who have knocked their head into the door frame on the way out of the door or similar trauma with so little force that it is impossible to imagine any damaging effects. Where should these patients be placed in the classification today? The only possibility is probably to disregard the trauma and code them as new daily persistent headache, but there is an obvious event that reportedly has caused the headache and this is not the case in new daily persistent headache. I therefore believe that headache attributed to insignificant trauma should be included in chapter 5 of a future edition.
Headache attributed to cranial or cervical vascular disorder
This is an extensive and very detailed chapter containing many important headache diagnoses. Similar to most other chapters on secondary headaches, there is very little research documenting these headaches and even fewer testing the diagnostic criteria. A small recent study has shown that after arterial dissection a fairly large number of patients suffer from headache persisting after three months (3). Whether this is the case for other diagnoses in this chapter is uncertain. A peculiar feature is headache probably attributed to reversible cerebral vasoconstriction syndrome. The general principle in the classification is not to include any probable categories in the secondary headaches. Here is an unwanted exception that should be removed.
Headache attributed to non-vascular intracranial disorder
This important chapter is in good shape and contains many important headache disorders. Similar to other chapters on secondary headaches the great majority of these headaches have not been studied prospectively in large patient numbers. Likewise, there are no studies of persistent headache attributed to intracranial disorder. A large number of patients should be studied with standardized collection of clinical data allowing testing of the existing and alternative diagnostic criteria. Patients who do not fulfill existing criteria should be analyzed to see if the criteria can be adapted to be more inclusive without losing specificity. For some headaches this may not be terribly important but, for example, headache attributed to Chiari malformation type 1 is important. Many of these patients have neurosurgery because of their headache and it remains completely uncertain whether the headache is in fact caused by the Chiari malformation and whether this surgery is beneficial.
Headache attributed to a substance or its withdrawal
There are new criteria for medication-overuse headache (MOH). In the past headache had to occur or worsen simultaneously with medication overuse and it had to disappear or get better after discontinuation of the medication overuse. In most cases it was, however, not possible to establish such temporal relationships. Furthermore, there is no guarantee that a primary headache made chronic by medication overuse is reversible after discontinuation of the overuse. The new criteria simply require that the patient has a primary headache and uses acute medication more frequently than allowed according to ICHD-3 beta diagnostic criteria. This has greatly facilitated the diagnosis of medication overuse. In my opinion the current solution is pragmatic and useful and it also solves the problem of primary versus secondary headache because patients with overuse should have both the MOH diagnosis and the primary headache diagnosis.
Headache attributed to infection and headache attributed to disorder of homeostasis
There are no major problems in these chapters except for the usual lack of prospective scientific study of the entities included. In particular persisting headache after meningitis is worth more study.
Headache or facial pain attributed to disorder of cranium, neck, eyes, ears, nose, sinuses, teeth, mouth or other facial or cervical structures and headache attributed to psychiatric disorder
The problems around cervicogenic headache and TMD have already been discussed together with TTH. There are no other specific problems in this chapter except the usual lack of scientific validation of the diagnostic criteria. The same is true concerning headache attributed to psychiatric disorder. Here the evidence is very sparse and nothing has been done to identify or validate such disorders since publication of the ICHD-2.
Painful cranial neuropathies and other facial pain
The title of this chapter is actually a little bit odd because it is a chapter in a headache classification. It should perhaps better read painful cranial neuralgias and other facial pains. Diagnostic criteria for trigeminal neuralgia have been elaborated by a joint committee of members of the International Headache Society and members of the International Association for the Study of Pain. The criteria for 13.1.1 Classical Trigeminal Neuralgia given in Figure 6 are certainly very specific but they may be too insensitive. As always, new criteria are developed on the basis of the opinion of experts and prospective testing on large numbers of patients is necessary. Most of the other entities in this chapter are relatively rare and do not pose significant problems. The same is true of the final chapter, 14: “Other headache disorders,” which simply contains headache not elsewhere classified and unspecified headache.
Concluding remarks
Headache classification is an evolving process. Even after 25 years of work and three editions of the ICHD there are still possibilities for further improvement. In this paper I have partly pointed to some inconsistencies in the ICHD-3 beta and partly I have made clear how little research has been conducted, particularly in the secondary headaches. Hopefully this paper can stimulate field testing so that results will be ready soon enough to be used for the final version of ICHD-3. If not, I have at least raised issues to be addressed by a future Headache Classification Committee that shall develop the fourth edition of the ICHD in 10–15 years’ time.
Clinical relevance summary
Basilar/brain stem aura overdiagnosed. Tension-type headache should be broad. Cervicogenic and temporomandibular headaches overlap. Trigeminal neuralgia too insensitive.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.