
Abstract
A variety of headaches are frequently associated with the occurrence of neck pain. The purpose of this paper was to describe the adherence to diagnostic criteria of a series of patients enrolled on the basis of two clinical criteria: (1) unilateral headache without side-shift, and (2) pain starting in the neck and spreading to the fronto-ocular area. One hundred and thirty-two patients (36 male and 96 female) entered the study. Sixty-two patients were assigned to Group A (patients fulfilling criteria 1 and 2), 40 to Group B (criterion 2 only) and 12 to Group C (criterion 1, only). Eighteen subjects were excluded because X-rays of the neck were not available. Patients were evaluated regardless of whether or not they fell into one or more of the following diagnostic categories: cervicogenic headache (CEH), migraine without aura (M) and headache associated with disorders of the neck (HN) (IHS definitions). Fulfilment of the diagnostic criteria for CEH was found to be particularly frequent in Group A. A higher frequency of CEH diagnosis was found when two criteria were used (Group A) than in Group B (P = 0.001); in the former group a higher mean number of diagnostic criteria for CEH were also present (P = 0.001). Group A patients more frequently presented pain episodes of varying duration or fluctuating, continuous pain and moderate, non-excruciating, non-throbbing pain than Group B patients (P = 0.04 and P = 0.08, respectively). In Group C patients, the frequency of these two criteria was relatively low (17%) especially of the first mentioned variable. The presence of at least five of the seven ‘pooled’ CEH criteria (present in ≥ 50% of the patients) might be deemed a reliable cut-off point, allowing the headache to be diagnosed as ‘probable’ CEH. If patients fulfilling M or HN criteria in addition to the CEH criteria are added to the ‘pure’ CEH group a total of 74% of Group A patients may have a CEH picture. The temporal pattern of pain and the quality of pain in Group A showed good sensitivity and specificity (≥ 75) when compared with Group B; therefore, the chances of diagnosing a definite CEH are significantly more frequent in patients presenting with unilateral pain that also begins as a neck pain. Head/neck trauma and radiological abnormalities in the cervical spine were not significantly associated with CEH, M or HN diagnoses. An improvement of the current diagnostic IHS criteria might make it possible to avoid the existing, partial overlap of CEH with HN and M. Extensive use should be made of the GON, and other, blockades in the routine work-up of CEH, both in the differential diagnosis and in the mixed forms (CEH + M, and CEH + HN), in order to improve the efficiency of the current diagnostic system.
Introduction
Cervicogenic headache (CEH), as it was described in 1983 (1), is regarded as a preferentially unilateral headache that initially may be remitting but that tends to become chronic over time. It is of moderate intensity, appears most frequently in females, and is associated with symptoms and signs linking it to the neck. These include: onset of pain attacks in the neck/back of the head; reduced range of motion in the neck; precipitation mechanisms related to the neck, and possibly, the presence of shoulder/arm pain ipsilaterally to the head pain. A detailed clinical description of this headache appears in the IASP classification of chronic pain (2), where it is coded VII-2.
The clinical description of CEH as it appears in the original paper (1), is based on a relatively limited series. Clinical/instrumental evaluation provided evidence that the headache symptoms were the effect of a ‘noxa’, localized in the neck. Since then, this description has remained the point of reference for scientific purposes, i.e. further investigations of mechanisms, of levels of cervical dysfunction, and of treatments. However, the original criteria for CEH may have been rather specific, and thus their sensitivity could be unduly low. Some series of headache patients (retrospective evaluations) have pointed to such a trend (3). Attempts have been made to evaluate the consistency of the criteria for CEH in various series of headache patients (4–7). Fifteen per cent of the headache patients in an outpatient clinic in Brazil were identified as CEH (4, 5). In a Danish study (8), based on 826 randomly selected individuals from a population register, c. 18% were diagnosed as CEH cases. In Pereira Monteiro's study (6) of a population from Porto, the prevalence of CEH was found to be 0.4%, on the basis of the IHS criteria for headache associated with neck disorders. When the criteria of Sjaastad et al. (9) were applied, this prevalence rose to 1% and 4.6%, respectively, depending upon whether all, or only five, of these criteria were used. These data point to a higher sensitivity of the CEH criteria compared with the IHS criteria.
As described in the IHS diagnostic criteria in 1988 (10), the term ‘headache associated with disorders of the neck’ is clearly non-specific. Neck pain is also considered by the IHS classification to be the cause of referred headache or projected pain. The loose description ‘headache associated with disorders of the neck’ fails to specify, for example, the side, character and temporal pattern of the pain. It also requires X-ray evidence of changes in the neck (features which are not a regular part of the CEH definition). The IHS definition considers different pain conditions (tension-type headache, migraine, temporomandibular dysfunction, ‘pure neck ache alone’, etc.) to be fully acceptable for inclusion under the heading ‘headache associated with disorders of the neck’. Furthermore, there exists no clinical study prior to 1988 conducted on a large clinical patient series that supports the consistency of the IHS criteria (of group 11.2.1), in particular the X-ray criterion, nor has any validation study of clinical/radiological criteria been carried out since the classification was proposed. On the other hand, the situation as regards CEH looks somewhat different: CEH, a secondary headache with a rather well-defined clinical picture, is characterized by two essential, clinical aspects: (a) unilaterality of pain; (b) a clinically demonstrable neck factor.
On a more general level, the IHS system and its diagnostic criteria display a reasonably good power of resolution if one considers episodic headaches (migraine, cluster headache) and neuralgias (11, 12), but only few studies document their validity in more or less continuous forms. One flaw of the IHS system is its poor definition and importance of headache as a symptom among the secondary forms (i.e. ‘associated with’), whenever a headache case is observed for clinical as well as epidemiological purposes.
Any investigation into CEH, be it clinical or epidemiological, will inevitably involve the need to consider diagnoses other than CEH, reached by applying standard diagnostic criteria, such as the IHS ones. There is thus the chance that CEH will find itself grouped with the IHS classification's ‘unclassifiable’ primary/secondary headaches, or (more frequently?) with the same classification's diagnoses of ‘genuine’ migraine, tension-type headache, headache associated with disorders of the neck, etc. (or even with more than one of the aforementioned diagnoses).
In order routinely to identify a headache as CEH, a category of ‘possible CEH’ cases is needed, but in order to develop such a category, the sensitivity and specificity of the diagnostic criteria would first have to be evaluated.
Currently, while the differential diagnosis of CEH vs. other unilateral headaches such as cluster headache (13), chronic paroxysmal hemicrania (14) and hemicrania continua (15) can be made with reasonable certainty, the greatest difficulties appear to concern the overlap between the respective diagnostic criteria for CEH and migraine without aura (‘common migraine’).
The principal aim of the present investigation was to ascertain the extent to which the following two complaints may assist in the classification of cases of ‘possible’ CEH: (a) pain starting in the neck and spreading to the frontal area; and (b) unilaterality of headache without side-shift.
We intend subsequently to evaluate the reliability of the CEH diagnosis (according to the original criteria) in a prospective series of patients.
Materials and methods
Patient series
The study was conducted on 132 consecutive patients (36 men and 96 women, mean age 35 ± 11 years; range: 19–70) educated for a mean of 12 ± 4 years. The mean age at headache onset was 29 ± 13 years; the mean illness duration was 6 ± 3 years, range 2.5–9 years.
Methods
Clinical information was obtained from patients at the time of their first consultation at the Headache Centre of the C. Mondino Foundation, University of Pavia. A headache history was obtained through a structured interview (part of the compilation of a large data base which also included standard clinical examination and the gathering of data relating to different instrumental, diagnostic and therapeutic procedures) conducted by a single investigator (FA). Patients were selected on the basis of two clinical characteristics derived from the original diagnostic criteria for CEH (1, see Appendix 1): (a) unilateral headache without side-shift; and (b) pain starting in the neck and spreading to the fronto-ocular area. They were then grouped as follows. Group A (presence of both features): unilateral headache without side-shift (I) and pain starting in the neck, eventually spreading to oculo-fronto-temporal areas, where the maximum pain is often located (VI). Group B (fulfilment of one criterion): pain starting in the neck, eventually spreading to the oculo-fronto-temporal areas (where the maximum pain is often located) (VI). Group C (fulfilment of one criterion): unilateral headache without side-shift (I). In group A and B, the neck pain was invariably unilateral at onset, but could eventually spread across the midline during particularly severe and protracted attacks.
Cluster headache and tension type headache were excluded on the basis of the diagnostic criteria established by the IHS in 1988 (10). Chronic paroxysmal hemicrania, and hemicrania continua were thought to be unlikely alternatives (2), but as far as the latter is concerned it should be emphasized that no formal indomethacin test was carried out (16), for which reason this diagnostic alternative cannot be completely excluded.
At a later stage, the diagnostic criteria for CEH (9), migraine (M) (10) and headache associated with disorders of neck (HN) (10) were assessed on the basis of a detailed work-up.
The original diagnostic criteria for CEH (9) were ‘pooled’, as shown in Table 1. They were then identified and counted in the single patient. This was done in order to assess the number of criteria needed for a headache stemming from the neck to be diagnosed as CEH.
Pooled form (1–7) of the diagnostic criteria for cervicogenic headache proposed by Sjaastad et al. (1990); in each case the number of the original diagnostic criteria is given in brackets

Criterion 6 embraces two criteria, namely (a) and (b); these two criteria were ‘pooled’ after the enrolment of the patients due to the lack of pain, in some of them, at the time of interview, and thus it was impossible to carry out a nerve blockade So, in this context, the fulfilment of one criterion suffices.
X-rays of the cervical spine were carried out in order to evaluate an abnormal posture or flexion-extension impairment. In case of reduction of intervertebral space, patients underwent a preliminary CT scan, in order to evidence a disc protrusion/herniation, and eventually a spine MRI.
In most of the patients a proper GON anaesthetic blockade was not carried out, the pain being less than 50% of the maximum at the time of consultation.
Statistical analysis
Data were analysed using the statistical program SPSS 6.3 for Windows. The chi-square (according to the one-tail Fisher's exact test correction) was employed to compare the single items making up the diagnostic criteria.
Sensitivity and specificity of the diagnostic criteria were also calculated considering, respectively, patients presenting a symptom included in the diagnostic criteria (sensitivity), and patients not presenting an appropriate symptom and who thus did not satisfy the criteria (specificity).
Results
With reference to our inclusion criteria, 65.2% of the patients (86/132) had a unilateral headache (I) and in 87.9% (n = 116), the pain started in the neck (VI). Eighteen patients (Group A = 8, Group B = 6 and Group C = 4) were not included in the final evaluation because cervical spine X-rays were not available. Therefore, the results relate to 114 patients: Group A (I + VI), 62 (54.4%); Group B (VI), 40 (35.1%); and Group C (I), 12 (10.5%).
Table 2 shows the relative frequency of the diagnostic criteria for CEH in patients belonging to Groups A, B and C, respectively (9).
Relative frequency of diagnostic criteria for cervicogenic headache in patients belonging to Groups A, B and C

P < 005, two-sided Fisher's exact test comparing group A and B.
See text.
It is possible that the external pressure exerted in our study has been too mild.
Major symptoms and signs
Pain was induced by neck movements and/or sustained awkward head positioning, or by external pressure (II-a-1 and II-a-2) in 52% of the patients in Group A, in 40% in Group B and in 50% in Group C. Neck pain spreading to shoulder and arm ipsilaterally (II-b) was present as a rather vague, non-radicular pain in one-third to one-half of the patients (Table 2). The range of motion in the cervical spine was clinically reduced (at least 25% reduction in one or more passive movements of the neck) in a high percentage of patients (Group A = 84%, Group B = 80%, Group C = 67%) (II-c). No statistically significant differences emerged between the reported data recorded in the three groups of patients.
Pain characteristics
The pattern of the pain episodes in the three groups of patients was non-clustering; pain episodes of varying duration, or fluctuating continuous pain, was present in 62% of patients in Group A vs. 40% in Group B (P = 0.04, two-sided Fisher's exact test) and 17% in Group C (Table 2). Pain was moderate, non-excruciating, usually of a non-throbbing nature, in 73% of the patients belonging to Group A vs. 55% in Group B (P = 0.08, two-sided Fisher's exact test) and 50% in Group C (Table 2).
Other important criteria
Of the Group A cases in whom the procedure was carried out, the anaesthetic blockade of the GON was positive in only 17% (4/24). (Negative blockades: 20/24 in Group A; 18/18 in Group B and 8/8 in Group C). In 64 patients, anaesthetic blockade was not carried out, the pain being less than 50% of the maximum at the time of consultation.
A history of neck trauma, of the whiplash type, sustained prior to the pain onset was present in a relevant number of patients (Table 2).
Various attack-related phenomena
In the present series of patients, the minor (and more rarely occurring) diagnostic criteria were fulfilled in more than one-third of the patients (Table 2) only as regards dizziness in groups B-C.
Diagnostic criteria
Table 3 shows the relative frequency of the diagnoses CEH, M, HN (see Methods) when the diagnostic criteria are applied to the three groups of patients. A higher frequency of CEH diagnosis was found in Group A compared with Group B (respectively: 55% vs. 20%; P < 0.001, Fisher's exact test) as one should expect from the hypothesis. It is also remarkable that no patients in Group A had a HN diagnosis, while in Group B 25% of the patients fulfilled the criteria for HN. The distribution of patients with diagnoses of CEH associated with M or HN is not statistically different in Groups A and B. Moreover, the number of non-classifiable patients is relatively higher in Group C than in patients in Groups A and B. No patient in any of the three groups presented a diagnostic overlap between M and HN.
Diagnosis in patients belonging to Groups A, B and C

P < 0001, Fisher's exact test. CEH=cervicogenic headache; M=migraine without aura; HN=headache associated with neck disorders; CEH and M, CEH and HN=satisfied the diagnostic criteria of both headache categories. Non-classifiable=insufficient criteria for CEH, HN, M.
Taking the seven ‘pooled’ diagnostic criteria for CEH (see Methods and Table 1), 74% (n = 46) of the patients in Group A (including also CEH + M and CEH + HN patients) fulfilled at least five of them (three criteria in addition to the two obligatory criteria) compared with 35% (n = 14) of the Group B (Group A vs. Group B P = 0.0028, chi-square) and 17% (n = 2) of the Group C patients (Group A and B vs. Group C P = 0.000, chi-square) (Fig. 1). Fulfilment of at least five of the seven criteria seems to constitute a reliable cut-off point at which headache patients can be diagnosed as CEH, provided the head pain is unilateral and is starting in the neck (‘possible’ CEH).

Frequency of the pooled diagnostic criteria (4) for CEH in Groups A, B and C.
Patients diagnosed as CEH in Group A fulfilled 3.53 ± 0.51 criteria in addition to the inclusion ones, whereas M patients fulfilled far fewer criteria: 1.25 ± 0.46 (P < 0.001, one-way
Mean number of diagnostic criteria for CEH (in addition to the inclusion criteria) in patients belonging to Groups A and B

CEH vs. M in Group A and B; CEH vs. HN in Group B: P < 0001, one-way
CEH vs. the corresponding value in Group B: P = 0006, one-way
Sensitivity and specificity levels of the single diagnostic criteria in CEH patients are shown in Table 5 and Fig. 2. The temporal pattern (IV) and the moderate, non-pulsating headache (V) presented high sensitivity and specificity (≥ 75). Similarly, the shoulder–arm symptom criterion has a good specificity and acceptable sensitivity. It is worthy of note that the other symptoms and signs of neck involvement (excluding a reduced range of motion in the cervical spine) showed high specificity, but rather low sensitivity. Similarly, minor symptoms and signs presented very low sensitivity but high specificity. The anaesthetic blockade of the GON carried out in this study seems to be a specific but not a sensitive criterion.

Sensitivity and specificity in patients fulfilling the CEH criteria (Group A upper panel, Group B lower panel).
Sensitivity and specificity of diagnostic criteria in patients fulfilling the CEH criteria

Inclusion criterion.
Relationship with previous trauma
A head/neck trauma (whiplash type) had been sustained in 44 (71%) Group A patients, in 34 (85%) Group B patients and in 12 (100%) Group C patients; no statistically significant difference was found between the CEH patients of Group A and those of Group B as regards the number of previous traumas sustained (Table 6). In all cases, either the headache antedated the trauma or an interval of over 2 months (23.6 ± 27.3 months) had elapsed between trauma and headache onset. The interval between whiplash injury and headache onset was significantly shorter (P < 0.005; one-way
Frequency of head/neck trauma (whiplash) in anamnesis

Number of patients having sustained neck trauma.
Total number of patients fulfilling the criteria for diagnosis.
Radiological findings
In our series, 49.1% patients had a normal X-ray of the neck. The presence of a spinal abnormality was significantly higher in Group B (30/40; 75%) than in Group A (16/62; 25.8%) (P < 0.001; Fisher's exact test) patients (Table 7). In Group C four of 12 (33.3%) had abnormal X-rays. In patients with radiological abnormalities (a requirement in the IHS classification), either a rectilinearization (X-rays) or disc protrusion/herniation (CT scan) was found. These findings were present with the same frequency on both the symptomatic and non-symptomatic sides (Table 7), indicating that an ordinary cervical spine X-ray is not really a sensitive enough method for a diagnosis of CEH. Cervical spine rectilinearization without disc herniation was the only finding in Group C. No significant distribution of the radiological abnormalities was found in patients within the diagnostic Groups A and B. Since Group C had only four cases of abnormal radiological findings, two of whom had the diagnosis of CEH + M, no statistical evaluation was carried out in this group. However, our findings have to be considered with caution because, due to ethical reason, a control material could not be collected.
Frequency of cervical spine X-ray abnormalities in patients belonging to Groups A and B (due to the limited number of patients in group C, namely 12, these patients have not been inserted)
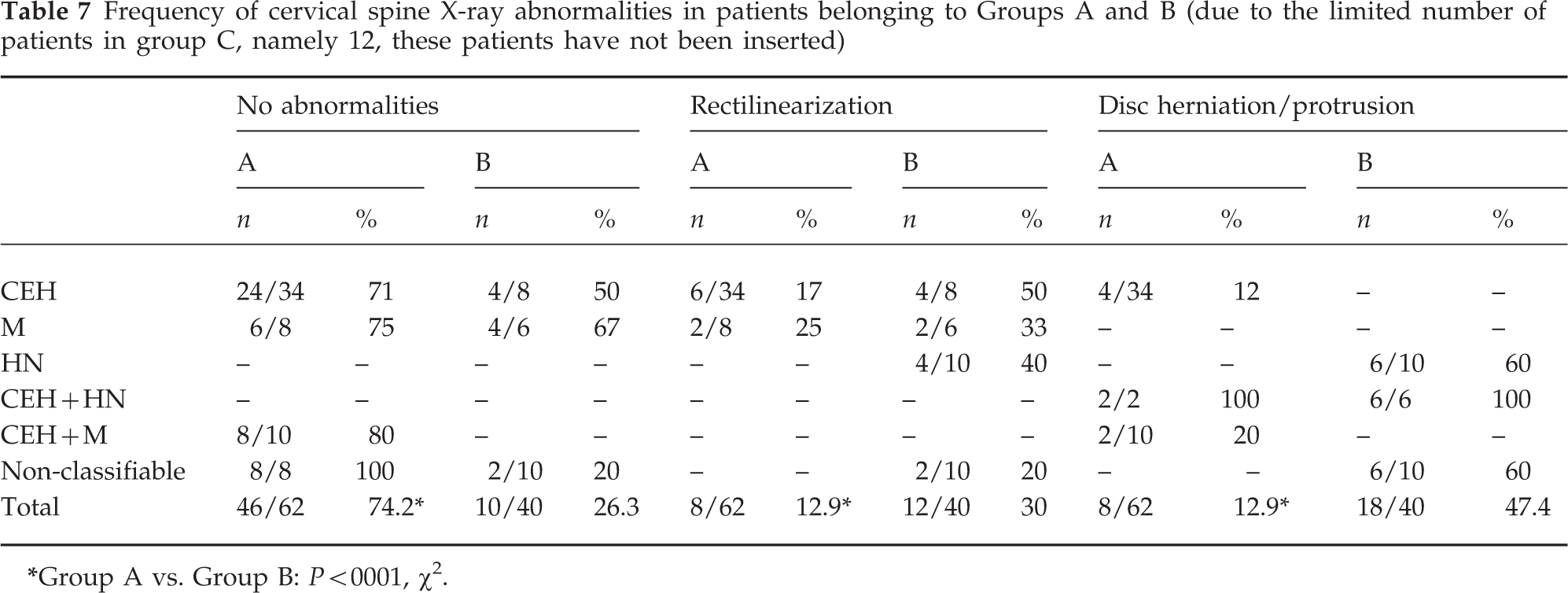
Group A vs. Group B: P < 0001, χ 2.
Discussion
Headache related to the cervical spine is often misdiagnosed and treated inadequately because of confusing and varying terminology (17). Not all headache patients with relevant neck symptoms (i.e. signs and symptoms of neck involvement) can be properly classified using the IHS criteria. The original diagnostic criteria for CEH have been questioned, mainly due to the relatively limited number of patients described; even the very existence of this entity/syndrome has been questioned. In a recent review, Leone et al. (18) criticized various advances made in the field of CEH. The unfortunate conclusion reached by these authors, i.e. that of non-existence of CEH, we consider as unwarranted. This conclusion can largely be criticized due to the overt shortcoming of the study methodology (i.e. non-prospective studies) and to various misunderstandings (of the concepts of ‘unilaterality of pain’, of clinical examination of ‘neck range of motion’, etc.) (3, 19). The lack of objective information in this field is due to the relatively small number of prospective studies published.
The present study indicates that application of the two criteria used in the classification of our Group A represents a putative initial step that might allow the identification of ‘possible’ CEH patients; the application of a further three diagnostic criteria increases considerably the likelihood of correctly identifying ‘probable’ CEH cases. Therefore, the criterion of unilaterality, as described in the revised classification of CEH (20), may seem to be a crucial diagnostic piece of evidence. Unilaterality of pain as defined in the original criteria was probably too ‘strict’ a criterion, while the revised, somewhat ‘loosened’, definition seems in our experience to be more acceptable nosographically.
Applying the original CEH diagnostic criteria, we identified 42/114 (37%) patients with CEH; 16/114 (23%, respectively: 9% HN and 14% M) fulfilled the criteria for an IHS diagnosis of HN (n = 10) and M (n = 16), while the other 26 would be attributed the IHS diagnosis of ‘headache not fulfilling the listed criteria’ (migraine-like?). Moreover, there was, in our series, no overlapping of diagnostic criteria between M and HN. However, 20/114 (17%) patients satisfied the criteria for both CEH and M or for both CEH and HN (IHS). In these cases, it was hard to assess with precision during the clinical interview, whether these were concomitant or overlapping diagnoses.
CEH is steadily gaining credence as a diagnostic alternative, and the criteria currently applied do allow a clear distinction to be drawn between CEH and CPH, hemicrania continua and chronic daily headache (21). Nosographic difficulties apart, CEH is becoming increasingly accepted thanks to improvement of the therapeutic approach (22, 23).
Clinical evidence of neck involvement was present in the majority of our sample (60/114; 52.6%) and the percentage was even higher when considering those members of our population who fulfilled also the criterion of unilateral headache (42/62; 67.7%). The IHS classification criteria do not constitute an adequate basis for the proper nosographic evaluation of these patients.
Applying the original classification criteria of Sjaastad et al. (9), headache patients can be classified as cervicogenic on the basis of the presence of many characteristic diagnostic criteria.
However, as shown in the present paper, CEH still can overlap with migraine, on the one hand, and with headache associated with disorders of the neck (IHS) on the other. Furthermore, using the current IHS diagnostic criteria for headache (24) there remain a relatively small number of patients that cannot be classified at all.
When seeking to distinguish M from CEH, ‘migrainous’ symptoms, like nausea and photophobia, represent a clinical challenge, especially when they are not marked. Moreover, in the migrainous population of Blau and MacGregor (25), two-thirds of their patients reported neck symptoms during attacks, and 43% recognized neck pain as a trigger factor for migraine attacks. However, findings from studies where one has failed to use a CEH category should be treated with caution.
Another diagnostic difficulty emerges when headache arising from the neck occurs simultaneously with M or TH. According to Pffaffenrath and Kaube (26), 56% of their patients had CEH in combination with other headaches. In the present study (Table 3) a coexistence of CEH with either M or HN has been found in 17% of the cases.
According to the original diagnostic criteria for CEH, a positive response to appropriate anaesthetic blockades of the GON, or of the facet joints, is essential for a positive diagnosis of CEH. In this study, we were unable to perform blockades in every case due to the pain severity. This diagnostic test could reduce the number of CEH cases associated with other headache forms and represent a diagnostic tool in the differential diagnosis of CEH vs. other unilateral headaches (27–29). In doubtful cases, patients should undergo diagnostic facet joint blocks, and, if necessary, provocative and analgesic discography, at appropriate levels, in an attempt to identify other sources of the pain (30).
No specific radiological abnormalities (by plain X-rays of the cervical spine) were identified in CEH by Pffaffenrath et al. (31) or by Fredriksen et al. (32), which underlines, at the present time, the fundamental importance of basing the diagnostic work-up of such patients on the clinical picture. Our data also support previous notions indicating that radiological abnormalities, when present, are probably not specific for CEH. It is admittedly a drawback that an age-matched control series could not, for ethical reasons, be obtained in the present study.
The frequency of headache with CEH characteristics 1 year after the traumatic event was 3% in the Oslo whiplash study (33). However, further prospective data are needed to clarify the role of whiplash in CEH. In our experience, CEH is not likely, in principle, to be a post-traumatic headache, since the frequency of head/neck trauma is not significantly higher in CEH subjects than in patients with other kinds of headache (i.e. M or HN). At least, it is unlikely to be the sole factor in most cases. However, it is not the percentage of traumas that counts, but the type of trauma in a given patient.
We feel that the number and the relative importance of the diagnostic criteria for CEH (‘major criteria’, ‘pain characteristics’, ‘other important criteria’) (9) constitute, at the present time, a relevant aspect in identifying patients. Our data indicate that at least five out of the seven ‘pooled’ criteria should be present in order to establish a diagnosis of CEH. Moreover, if pain first is experienced in the neck and then spreads to the fronto-ocular area and it is unilateral, the chance of correctly identifying patients as CEH instead of HN sufferers increases significantly (Table 3). Therefore, our findings confirm the importance of unilaterality and pain distribution as a mandatory requirement for CEH diagnosis.
In the type of patients selected with the two inclusion criteria employed in our study, temporal pattern and quality of the pain seem to be the two criteria showing the highest sensitivity and specificity. A similarly high specificity was found as regards symptoms and signs of neck involvement (in particular pain, of a rather vague, non-radicular nature, elicited by external pressure over the GON and ipsilateral discomfort in neck, shoulder or arm), the importance of which has been stressed in the revised classification criteria (20). This is partly in accordance with the view of Vincent (34), who also validated the sensitivity and specificity of the criteria for CEH, M and tension-type headache.
The revised diagnostic criteria for CEH developed by the Cervicogenic Headache International Study Group (20) probably constitute an important step forward, even though they need to be validated in large series of patients. Moreover, we already foresee the time when further areas of interest will be studied (personality factors, markers of neck movements, etc.) and experimental models will be available (effect of trauma, late whiplash syndrome) allowing CEH to be better characterized. However, our data should be considered with caution because the case selection could have an entrance bias, as the study was carried out in a headache centre population series of patients.
Footnotes
Acknowledgements
This paper was supported by a grant from the Ministry of Public Health 57.2/RF93.28. We wish to thank Mrs Paola Castellotti for laboratory assistance.