
Abstract
Background
Persistent post-traumatic headache (PPTH) is a disabling sequela of traumatic brain injury (TBI). Many individuals seek behavioral interventions to supplement pharmacological treatment. This systematic review describes behavioral interventions for treatment of PPTH and psychosocial factors related to outcomes in adults.
Methods
A systematic search for behavioral interventions for adult patients who suffered headache attributable to mild TBI was conducted across PubMed, CINAHL, Scopus, PsycINFO and Cochrane Library in June 2024. Studies were excluded if they (a) did not evaluate outcomes related to PPTH pain; (b) evaluated pediatric populations; (c) used animal models; (d) evaluated interventions other than behavioral modalities; and (e) TBI was moderate or severe. Risk of bias was assessed for included randomized controlled trials (RCTs) using Cochrane's Risk of Bias II (RoB2).
Results
The search and evaluation process identified 12 articles evaluating 2293 individuals with PPTH. Study designs included randomized controlled trials (n = 4) and observational studies (n = 8). Behavioral intervention modalities included cognitive behavioral therapy (n = 5), education/counseling (n = 3), exercise (n = 2) and integrated managed care (n = 2). Three included RCTs were assessed to have low risk of bias and one had some concerns of potential bias.
Conclusions
Cognitive behavioral interventions within interdisciplinary systems of care may be the optimal combination. Mutual maintenance may explain and contextualize the high comorbidity between PPTH and affective distress. Treatment for PPTH in adults with mild TBI should incorporate treatment for psychological distress.
Trial Registration
This systematic review was registered in Prospero (CRD42024556014).
This is a visual representation of the abstract.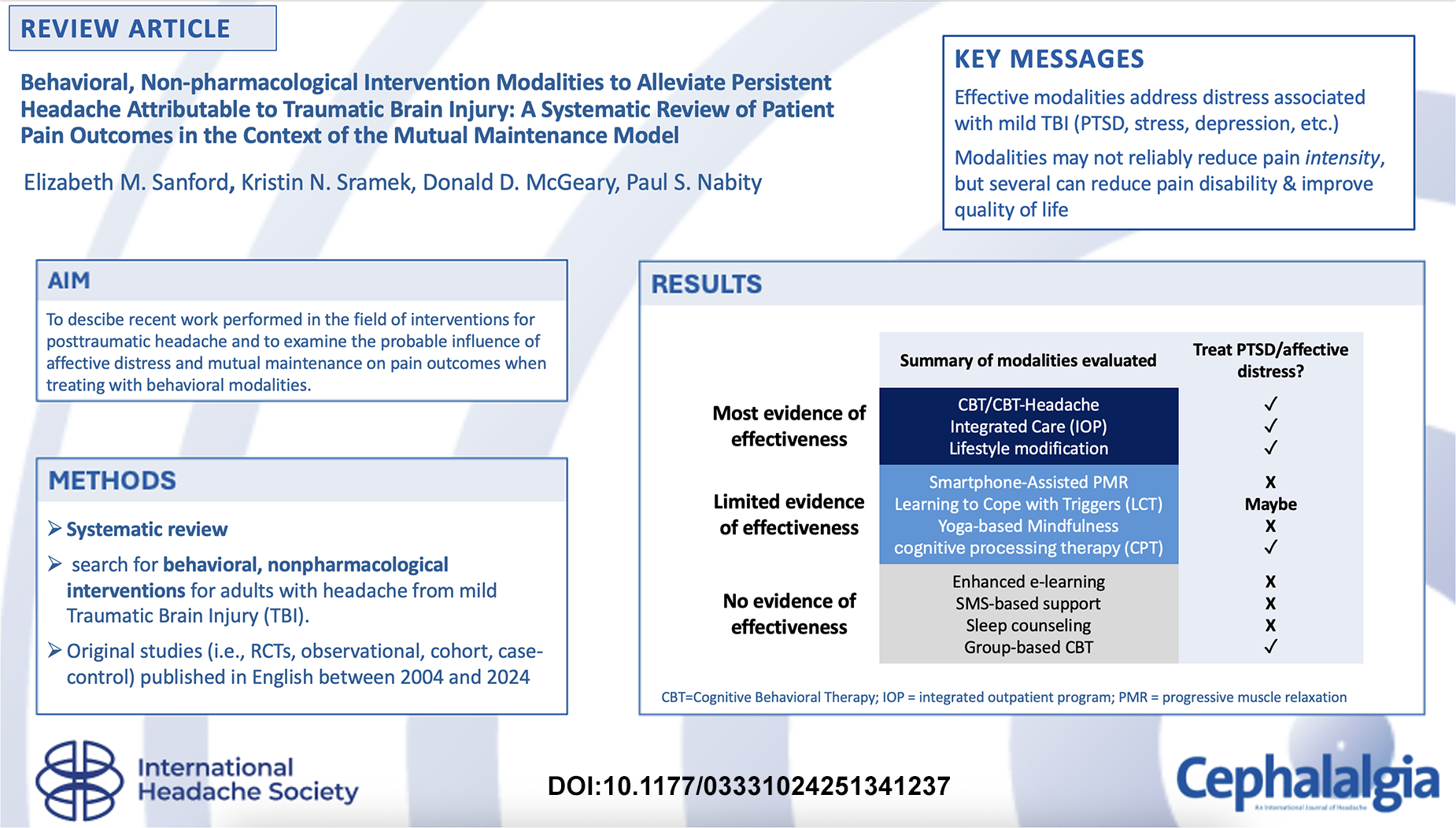
Keywords
Introduction
Post-traumatic headache (PTH) is a predominant sequelae of traumatic brain injury (TBI) (1–3). The International Classification of Headache Disorders, 3rd edition (ICHD-3) defines PTH as a secondary headache attributed to brain injury/concussion from blast or blunt trauma (4) that develops within a week of injury, although some suggest a longer period (5). While acute PTH often improves within three months of injury, headaches that persist longer than three months meet criteria for persistent PTH (PPTH). PPTH pain is typically characterized in terms of similarity to headache pain from a primary headache disorder, usually as “migraine-like” or “tension-type” (4) or a mixed phenotype that incorporates features of both.
PPTH is uniquely challenging to treat because it often presents with a variety of psychosocial symptoms, and the severity of these symptoms appears to be related to severity of headache pain. PPTH etiologies, development characteristics and long-term persistence may be unique due to their strong relationships to affective distress and mood disturbance. Pena et al. (6) reported that individuals with PPTH had greater depression and anxiety and worse postconcussive symptoms than healthy controls. Similarly, Kristoffersen et al. (7) found that psychological distress, neuroticism and disability were highly prevalent among individuals with PPTH. Chaput et al. (8) suggested that pain catastrophizing characteristics such as rumination, magnification and helplessness were positively related to pain severity and psychological distress after a mild TBI (mTBI).
There is evidence that these psychiatric effects are related to psychological trauma. Elder et al. (9) reported that rats with mTBI induced by blast developed behavior analogous to post-traumatic stress disorder (PTSD). According to Kjeldgaard et al. (10), PTSD was present in 30% of cases of PPTH among Danish civilians, whereas Theeler et al. (11) reported that PTSD was present in more than 40% of soldiers with PPTH after concussion sustained in battlefield conditions. Holtkamp et al. (12) suggested that, if mTBI is sustained in a combat-related context, it may lead to extreme physical and psychological injuries, such as PPTH and cognitive, somatic or behavioral comorbidities. Comorbid affective distress and chronic physical symptoms may be bi-directionally related (13). The Mutual Maintenance Model explains the relationship between chronic pain and PTSD as a shared process in which one condition perpetuates or even amplifies the other (14,15).
Despite the well-recognized role of psychological comorbidity in PPTH, these headaches are often treated with analgesic or abortive drugs alone, which do not address the psychiatric comorbidities that may underpin expression and maintenance of PPTH (16). There is limited evidence of the effectiveness of frontline pharmacotherapies for PPTH and ample evidence that drugs may be overused, cause complications and negatively impact medical comorbidities (17). Behavioral interventions targeting PPTH pain may be effective as a supplementary or alternative strategy to headache polypharmacy due to their ability to safely address patient-centered PPTH outcomes (18), and the broad-spectrum of associated positive effects may ameliorate comorbid conditions or symptoms that can exacerbate headache. Regardless, there are no widely accepted guidelines for the use of non-pharmacological interventions for PPTH.
The present systematic review aimed to describe the effects of evidence-based non-pharmacological-behavioral interventions (e.g. mindfulness, meditation, education/training, cognitive behavioral therapy) for PPTH across an array of outcomes, including adverse effects, overall headache impact, quality of life, pain intensity, headache days per month and headache-related disability.
Methods
Search strategy
The review investigation team conducted a systematic search in June 2024 in five bibliographic databases: PubMed, CINAHL, Scopus, PsycINFO and Cochrane Library. The team searched for studies evaluating the effects of behavioral, non-pharmacological interventions to manage PTH in adults with keywords for PTH/PPTH, concussion and TBI.
The search algorithm is detailed in the supplemental material. Inclusion of manuscripts was limited to published, peer-reviewed literature because these sources are most likely to inform clinical practice guidelines. This systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines (19,20) and used the PRESS guideline statement (21). We used search terms, including variations, permutations and Medical Subject Headings terms related to (a) traumatic brain injury, (b) post-traumatic headache and (c) non-pharmacological or behavioral self-management strategies for headache pain. Other than the stipulated search terms, no other filters were applied to ensure a sensitive search strategy that was consistent with Cochrane Handbook's recommendations (22). The database search was supplemented with a manual search for additional studies itemized in previously published systematic reviews (23–25) detailing non-pharmacological treatments for PPTH to ensure completeness of the present systematic review process.
Eligibility, selection and analysis
The search was conducted to identify original studies (i.e. randomized controlled trials [RCTs], observational, cohort, and case–control studies) published in English between 2004 and 2024 to ensure that the included studies reflect the current knowledge of PPTH. Studies with patients who suffered headache attributable to mTBI were included. Studies were screened for general appropriateness and were excluded if (a) PPTH-related pain outcomes were not evaluated; (b) a pediatric population only was evaluated; (c) animal models were used; (d) interventions other than self-management behavior modalities were evaluated; or (e) patients had diagnosed moderate to severe TBI. Single-subject case studies, conference proceedings or poster abstracts, protocols, proposals, letters, commentaries, book chapters, letters, methods papers, systematic reviews, and meta-analyses were excluded.
Two investigators independently screened all titles and abstracts by means of Rayyan software (26). Records that met criteria were retrieved for full article evaluation. Conflicts were resolved by consensus between reviewers and, when necessary, adjudicated by the final author. Risk of bias was assessed for RCTs only, using Cochrane's Risk of Bias II (RoB2) (22,27). A descriptive analysis of the results was provided. This systematic review was registered in Prospero (CRD42024556014) where the protocol may be accessed.
Results
As shown in Figure 1, the database search yielded 598 records. After 227 duplicates (38%) were removed, 371 records were evaluated independently for potential inclusion. The team identified 20 reports from the database search and 16 reports from the citation and manual search. Of the 36 reports assessed, 24 were excluded. Twelve studies met the final inclusion criteria.
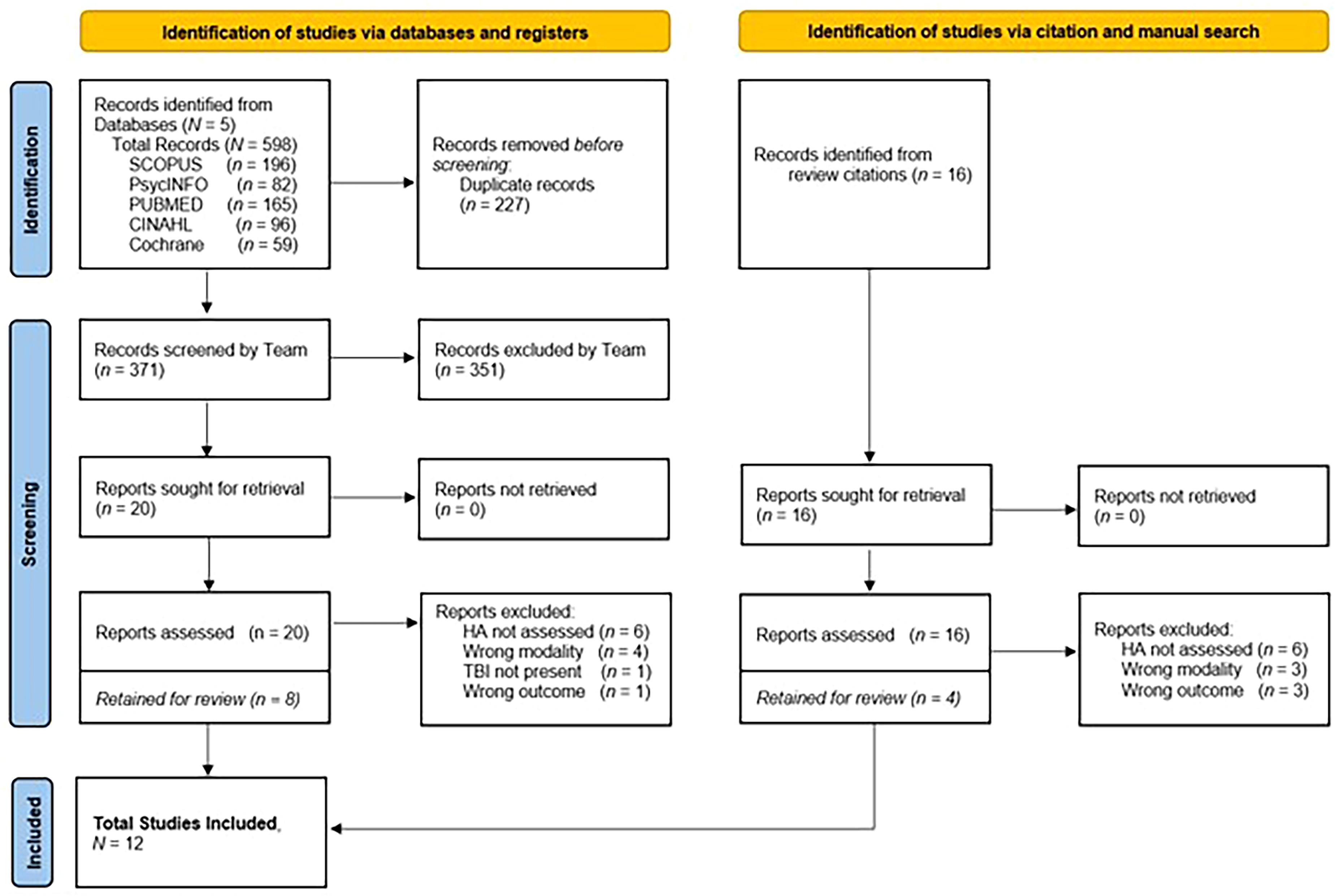
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flow diagram of study selection processes.
Study populations included civilian patient populations across multiple nationalities (n = 7) and active-duty US military or veteran populations (n = 7). Eleven studies evaluated behavioral treatments in populations reporting only persistent PTH; one study reported on findings from a mixed sample with acute PTH as well as PPTH. Study designs included RCTs (n = 4) and observational (n = 8). Non-pharmacological, behavioral interventions included cognitive behavioral therapy modalities (CBT, n = 5), education or counseling (n = 3), exercise (n = 2) and multi-modal or integrated care (n = 2). Observational studies were reported in Table 1. RCTs are reported in Table 2.
Overview and description of included observational studies.

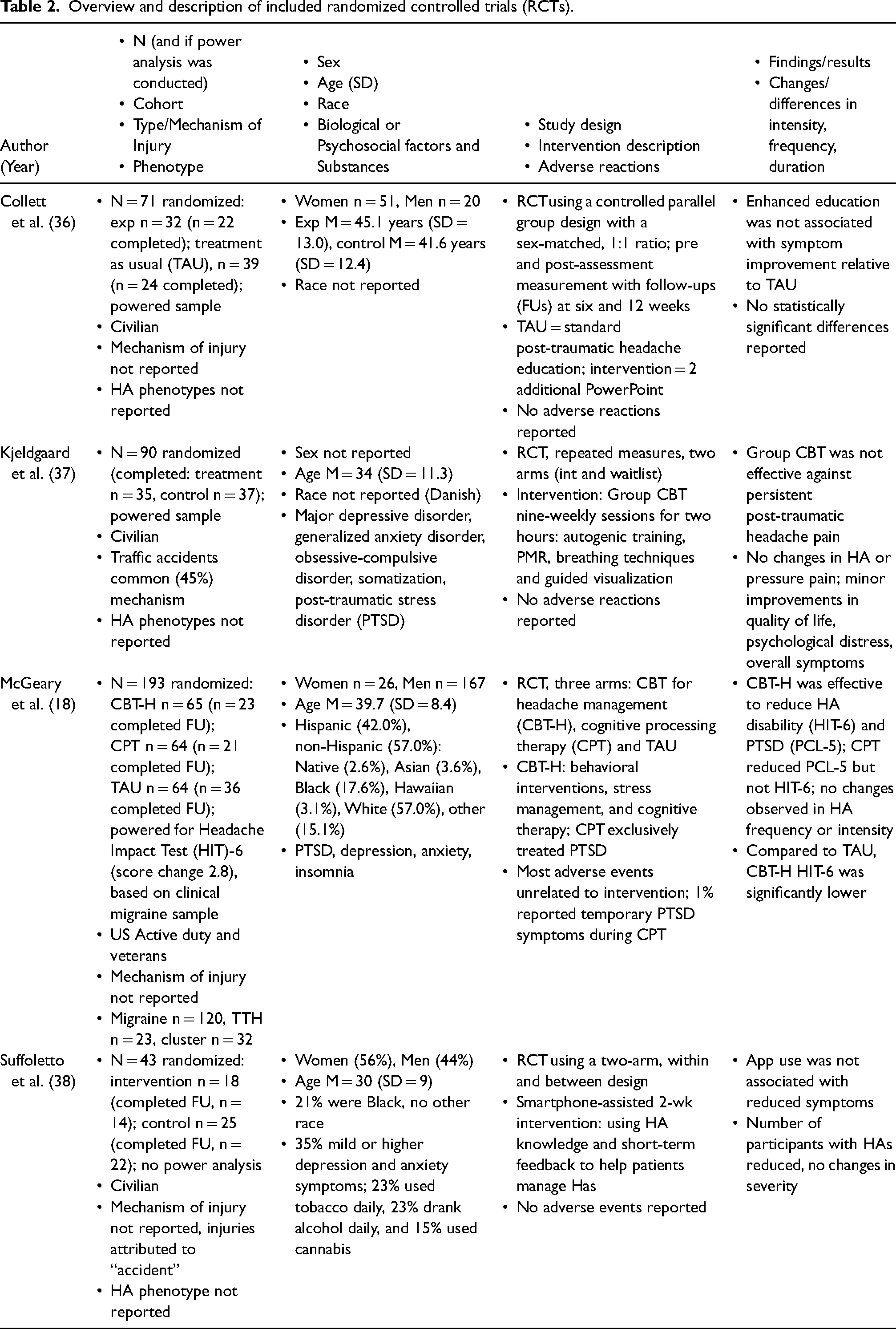
Overview and description of included randomized controlled trials (RCTs).
Cognitive behavioral interventions (n = 5)
Most of these CBT studies evaluated a combination of different approaches, including behavioral interventions, cognitive restructuring and stress management/relaxation paradigms. Treatment delivery varied and included individual and group formats as well as treatments delivered in-person and those delivered through an interactive health application.
Gurr and Coetzer (31) piloted a study to evaluate a CBT-based intervention for PPTH after mTBI. Of the 41 participants (8.9% mild, 26.9% moderate, 63.4% severe self-ratings of headaches), 20 completed the intervention and 13 completed the follow-up. Study completers reported greater headache intensities, and many participated in other intervention programs in the same facility, which the investigators suggest could have resulted in higher expectations of the PPTH intervention. Participants reported statistically significant improvements in headache-related disability, intensity, frequency and duration as well as reduced anxiety and depression, particularly among follow-up completers. These results suggest there was a strong mutual relationship between reducing emotional distress and headache, which CBT was effective in exploiting. The study was limited by its single-arm design, small sample (n = 20), inconsistent self-report data at each measurement time, unstandardized diagnostic interviews and absence of medication control.
McGeary et al. (18) compared CBT for headache management (CBT-H) and cognitive processing therapy (CPT), which is another CBT modality designed specifically for treating PTSD in patients with mTBI and PPTH; these were compared to treatment as usual (TAU). CBT-H was more efficacious than TAU in reducing both headache related disability and symptoms of PTSD. CPT was more efficacious than TAU at reducing symptoms of PTSD after mTBI, but not headache-related disability. There were no statistically significant changes in headache frequency or intensity for either study intervention, potentially due to the study being powered to detect Headache Impact Test-6 (HIT-6) score change (2.8 points). The study's strengths included a design that followed the gold standard for RCTs assessing outcomes from clinical behavioral interventions: they powered their sample, used validated outcome measures and conducted sensitivity analysis to control for planned dropout; while patients could not be practicably blinded, assessment administrators and statisticians were blinded to patient condition. With these rigorous controls in place, the design was assessed to have low risk of bias (Figure 2).

“Traffic light” visualization of results of bias assessments conducted for each included RCT using Cochrane's Risk of Bias II (RoB2) instrument. Visualization was rendered using the RoB2 tool (https://mcguinlu.shinyapps.io/robvis).
Kjeldgaard et al. (37) evaluated group-based CBT to treat pain perception, psychological symptoms and quality of life in patients with mTBI and PPTH. Of 90 randomized participants, 72 completed the final assessment (35 of wait list control and 37 of treatment group). The overall RCT design was relatively strong with a large, powered sample and random allocation procedures. Some baseline imbalances in clinical symptoms between groups were reported, but differences were not statistically significant. While neither patients nor administrators could be blinded, dropout was roughly equal in both arms, and no study deviations were reported that were likely to be attributable to knowledge of study arm. This RCT was assessed to have low risk. However, while slightly improving some psychological distress outcomes (i.e. hostility, depression, anxiety) and quality of life, group-based CBT showed no efficacy against headache frequency or intensity.
Usmani et al. (35) evaluated the feasibility of a smartphone-assisted progressive muscle relaxation (PMR) application for patients with mTBI and PPTH. Among participants who performed PMR four or more times a week, headache days per month significantly decreased over three months. However, non-adherence was frequent and appeared to be related to issues with the application: obstacles to adherence included time constraints, difficulty concentrating or forgetfulness, app glitches and repetitiveness. This was a feasibility trial, and so the focus was primarily on participant use of the app, rather than efficacy of the intervention to reduce headaches. Depression and anxiety were measured but not directly treated with the intervention. The design lacked rigor, the sample was small, there was no comparison group, and data collection was hampered by high dropout and non-adherence.
Silverberg et al. (34) treated four women with PPTH associated with mTBI using Learning to Cope with Triggers (LCT), an exposure therapy model that reframes headaches as learned responses to stimuli, emphasizing identification of headache triggers and targeting strategies to either avoid or acclimate to them. The most common triggers reported were computer screens, light and noise; participants reported experiencing a headache nearly every day throughout the study period. Half of the participants reported at least one standard deviation decrease in average headache intensity and a clinically significant reduction (>50%) in headache days with moderate-to-severe pain at post-treatment. The study findings were limited by a small, homogeneous sample; further research is warranted.
PPTH management counseling (n = 3)
These studies addressed education and/or health-behavior counseling for headache after a TBI and appeared to show little effect for PPTH. Education options included headache-specific education, reassurance, and education on management of conditions likely related to headache (e.g. insomnia).
Collett et al. (36) evaluated enhanced headache education for PPTH using a series of PowerPoint educational presentations available through an e-learning platform, compared to TAU for patients with PPTH associated with mTBI. A powered RCT design, with limited direct interaction between participants and study personnel, and standardized administration were strengths of this design. The design used variable-size block assignment to conceal group allocation from participants and clinicians; attempts were made to track time spent with the presentations. A 35% attrition rate undercut power: only 46 of 71 enrollees completed the follow-up. Post-hoc analysis revealed that the baseline average Rivermead Post Concussion Symptoms Questionnaire (RPQ) scores of dropouts were higher than those who completed the follow-up, suggesting that missingness may not have been random in either group. This RCT was assessed to have some concerns of bias arising from missing outcome data. There was no evidence that enhanced education using an e-learning PowerPoint platform was efficacious in treating PPTH.
Suffoletto et al. (38) examined the feasibility of providing education and behavioral support via SMS text multiple times a day to reduce the number or severity of post concussive symptoms in patients with mTBI. A convenience sample of 43 participants was enrolled and randomly allocated to control or intervention group. About half endorsed a history of concussion prior to sustaining the injury associated with PPTH, and 35% endorsed depression and/or anxiety. Both control and intervention groups received the same text messages and assessments; in the intervention group only, participant responses to texts triggered feedback, symptom-specific education, reassurance and symptom management guidance. PTSD, depression and anxiety were measured but were not treated with the intervention. The study strengths included the RCT design, a novel and scalable intervention approach, high rate of SMS symptom assessment completion, minimal direct interaction with study personnel and low risk of bias. There were no statistically significant differences between the treatment and control group in headache severity, ability to concentrate or irritability/anxiety over the 14-day app-assisted period. The short treatment window with no follow-up, minimalist intervention approach, absence of any method to measure participant engagement with the platform, lack of treatment for psychological symptoms and the small unpowered sample may have contributed to these results.
Ruff et al. (33) used an intervention that included sleep hygiene counseling with nightly prazosin to evaluate if improving sleep could reduce headache pain in veterans with blast-related mTBI. Headache pain and sleep quality did improve among those who took prazosin, but not among those who received sleep hygiene counseling only. The observational design was strengthened by multiple within-subjects measurements. However, concurrent antidepressant treatments and prazosin, drugs commonly prescribed to treat symptoms related to PTSD, may have confounded the results (i.e. indirectly treating PPTH by treating the PTSD in a mutual maintenance relationship).
Exercise and physical activity (n = 2)
Two studies evaluated physical activity for PPTH management. Results from both suggest that, generally, greater levels of reported activity were associated with lower distress, though further research is needed to assess impact of exercise for headache outcomes.
Mercier et al. (32) evaluated the associations between physical activity, sedentary behavior, symptom burden and quality of life in adults with persistent post-concussive symptoms after mTBI (including headache). Sedentary individuals experienced lower overall functioning, more severe headaches, greater fatigue, and heightened depression and anxiety compared to their active counterparts. While the study's strengths include a large sample, comprehensive outcome measures and practical insights into the benefits of meeting activity guidelines, its reliance on retrospective self-reported data, cross-sectional design and selective population limits the ability to establish causation or generalize findings.
Betthauser et al. (29) evaluated feasibility of a yoga intervention to reduce headache burden in veterans with PPTH after mTBI. Alcohol use, major depression and PTSD were prevalent in the sample. Treatment completers reported moderate-to-high satisfaction, although less than half of the participants completed at least 75% of the sessions. Both the intervention and control groups reported reduced headache disability over time with no between groups statistic reported. Limitations included poor retention, a small sample, limited quantitative data and limited reporting on post-treatment outcomes.
Multimodal or interdisciplinary (n = 2)
Some studies used multiple non-pharmacological interventions packaged as an integrated PPTH management program or interdisciplinary service. Multimodal and interdisciplinary treatments tend to be more intensive than standalone CBT treatments.
Baker et al. (28) evaluated a one-year lifestyle modification program for active-duty military personnel or dependents presenting with PTH. This sample was a heterogeneous mix of patients recruited to participate in the program as early as one month post injury up to ≥10 years since their injury. No relationship was evaluated between length of headache persistency after mTBI and treatment outcomes. Approximately two-thirds of the sample reported depression, anxiety, PTSD, and/or other psychological disorders. An integrated holistic approach addressing both physical and psychological aspects of PPTH was a strength of the program, but it was a weakness of the study, making any attempt to isolate which interventions were efficacious functionally impracticable. The small sample (n = 25) limited the generalizability of the findings. Reliance on retrospective self-report introduced potential bias, and the lack of controls for potential confounds, such as treatment for comorbid psychiatric disorders and high variability in time elapsed since injury, made it difficult to determine if the improvements were due to any specific intervention or natural remission.
DeGraba et al. (30) evaluated an integrated outpatient program (IOP) for active duty service members with mTBI and comorbid psychiatric and pain disorders, including headaches. Among those patients with persistent headaches (n = 935), over two-thirds reported significantly reduced headache disability by discharge. However, among those who provided a six-month follow-up (n = 89), significant loss of gains was reported. Strengths of the study included a large sample, use of validated outcome measures, and follow-ups at one, three and six months post-treatment. Similar to the above study, IOP integrated several evidence-based interventions, so specific modality(ies) that produced results could not be identified. There was no control group for comparison. Selection bias may have also influenced results because participants were highly motivated and were referred by their commands to the program.
Discussion
This systematic review synthesizes the findings of 12 studies of behavioral, non-pharmacological interventions for PPTH. Overall, the methodological rigor of published studies was low with a few exceptions that favored CBT and self-management strategies. Outcomes varied widely across the studies included in this review, which is likely attributable to differences in methodological quality and the broad effects of non-pharmacological interventions. A brief summary of the findings and conclusions of the investigators is provided in Figure 3. Consistent with prior reviews (39), sample sizes across the studies were generally small. However, several studies with larger samples reported beneficial effects of behavioral interventions for headache, suggesting that future studies with similarly robust sample sizes are likely to confirm effects for some treatments (18). Many behavioral therapies were designed specifically to address emotional and cognitive comorbidities that affect pain outcomes indirectly (40). These interventions have received increased attention in chronic pain research over the past few decades because of their broad-spectrum effects as well as their safety compared to pharmacotherapies. The manifest dangers of long-term use of opioid medications have prompted further interest in non-pharmacological treatments broadly (41). CBTs and multimodal and/or interdisciplinary programs have demonstrated impressive outcomes across various measures in the present review, including headache-related disability, pain intensity and quality of life. These findings are generally consistent with other reviews that recommend multimodal treatment for PPTH, especially when pharmacotherapies are combined with non-pharmacological interventions (25). Broad-spectrum behavioral PPTH treatments administered with or without complementary pharmacotherapies are likely to efficaciously address coping with pain and emotional distress at the same time, while reducing headache disability and headache days per month. More research is needed to confirm this.

Summary of modalities evaluated in the present systematic review, as well as whether treatment for affective distress was incorporated into each intervention, and primary conclusions. CBT = cognitive behavioral modalities; CBT-H = CBT for headache management; HA = headache; IOP = integrated outpatient program; LCT = Learning to Cope with Triggers; PE = prolonged exposure; PMR = progressive muscle relaxation; PTSD = post-traumatic stress.
PPTH and primary headache disorders may share common pathways and superficially similar clinical presentation but may not be effectively managed using the same treatments (31). In general, pharmacological treatments for migraine may demonstrate only limited effectiveness against PPTH pain (42–45). The high incidence of affective distress (e.g. PTSD, depression, anxiety and sleep problems) in the sampled 12 articles suggests it may share a strong, potentially mutual, relationship with PPTH. Comorbid affective conditions may diminish the effectiveness of many pharmacotherapies currently prescribed for PPTH. With the Mutual Maintenance Model as a framework, some patients who have chronic pain with psychological etiologies may require interventions that incorporate treatment for psychological distress. This interpretation may explain why several of the CBT modalities sampled here tended to be effective against multiple patient pain outcomes (18,37), even without pharmacotherapy. It may likewise suggest an explanation why even frequently-prescribed pharmacotherapies have been found to be only inconsistently effective as standalone treatments for PPTH (42–45). For best management of PPTH pain, it may be helpful to reframe and treat persistent headache associated with mTBI as a somatic symptom of exposure to a psychological stressor. Integrated approaches that help patients manage both the physiological and psychological dimensions of PPTH may be optimal for improving patient outcomes.
There are potential alternative mechanisms of PPTH that have not been discussed to this point. Structural brain abnormalities after a TBI may account for many behavioral changes, pain and adverse symptoms; however, this may be true primarily among individuals who sustain moderate or severe TBIs. Inflammation has also been implicated as a mechanism in the development of PPTH (46), but there is little consistent evidence in support of the inflammation model for treatment of PPTH. As noted above, many pharmacotherapies that are prescribed for persistent headaches target neuro-inflammation (non-steroidal anti-inflammatory drugs, monoclonal antibodies, propranolol, etc.), but these show inconsistent effect against PPTH (42–45). While it is possible that inflammation may be modestly reduced by CBT or mindfulness-based stress reduction methods (47,48), treating inflammation has not been shown as a reliable mechanism of improvement for PPTH. However, while there is support for models that show improvements in PPTH-related functioning mediated through reductions in anxiety (18,49), this apparent relationship may be more consistent with the Mutual Maintenance Model than a neuroinflammation model.
Modalities with promising PPTH treatment outcomes
CBT-based modalities demonstrated the most promising results for treating PPTH, particularly in reducing headache-related disability, improving psychological well-being and enhancing quality of life. We acknowledge that CBT in the sampled papers does not appear to reduce pain intensity, but using these techniques did demonstrate efficacy in reducing pain days and duration while improving quality of life. Across the five CBT approaches included in this review, a spectrum of therapeutic components was implemented, such as relaxation techniques, psychoeducation, stress management and cognitive restructuring with the goal of helping patients better cope with both pain and the psychological distress associated with PPTH.
Notably, in one trial (18), CBT-H outperformed TAU in reducing both headache-related disability and PTSD symptoms, and it outperformed another CBT modality (i.e. CPT). Interdisciplinary pharmacological, educational and stress management strategies were associated with reductions in PPTH pain severity and fewer pain episodes (28). Of the described CBT modalities, LCT (34) appears to be the least studied, but the results of the case series suggests the effects of implementation of LCT in patients with PPTH could be transformational. It is theoretically grounded as an exposure therapy, and it ticks all the necessary boxes for self-management of symptoms. Appropriately powered RCTs are urgently needed to make any further claims, but LCT may be the most exciting prospective cognitive behavioral treatment modality; moreover, the field appears to be wide open for researchers searching for novel behavioral treatments for PPTH. Interdisciplinary outpatient programs were also associated with improved headache related disability, with the added benefit of reduced psychiatric comorbidity and polypharmacy (30). However, there is limited evidence of the durability of these interventions to sustain long term improvements in headache outcomes; most of the sampled articles did not provide six-month and beyond follow-up outcomes. DeGraba et al. (30) did report post concussive outcomes at six months, but headache improvement was not sustained long term. Integrated care appeared to produce excellent results while in the program but more follow-up data with these interventional studies are needed to determine the long-term durability of these improvements.
Treatment delivery modality of CBT and integrated programs for PPTH appears to be important to successful treatment. The education-based treatments (33,36,38) had lackluster results, while studies using direct CBT or integrated approaches showed improvements for PPTH. Education may be necessary but not sufficient to produce behavior change. Self-efficacy is also needed (50); education modalities may not be sufficient by themselves to support patient self-efficacy, while CBT and related techniques may be well-suited to promote it. In fact, headache management self-efficacy has been shown to be a predictor for improvements in PPTH-related disability (49).
Psychosocial factors associated with PPTH and treatment outcomes
PTSD was the most common psychiatric comorbidity present among study samples included in this review. The Shared Vulnerability and Mutual Maintenance models (16) explain how PPTH and PTSD may perpetuate one another and limit the effectiveness of treatments. Significant overlap exists between chronic pain and PTSD, including sleep disturbances, attentional biases, avoidance, negative affect, decreased physical activity, anxiety and sensitivity coinciding with negative perceptions of illness and ineffective coping strategies (13). Shared pathways, such as the dysregulation of the stress response, can reinforce their co-occurrence. A meta-analysis (51) concluded that stress from psychological trauma exacerbated headache pain induced in laboratory conditions due in no small part to mechanistic moderators such as lowered pain thresholds and increased central sensitization related to affective distress.
Hypervigilance and intrusive thoughts associated with PTSD may increase stress, which may trigger or intensify headaches. Persistent headache pain may also heighten anxiety and stress responses, thereby magnifying problems associated with disability. Specifically, PTSD symptoms were found to be significantly associated with headache disability and unemployment status among individuals with mTBI (52). Unemployment can allow for increased time to ruminate if individuals are not engaged in meaningful activities. García et al. (53) found associations between unemployment, brooding (rumination on negative thoughts and feelings), and six-month PTSD symptom severity for individuals after a workplace accident. Cognitive-behavioral interventions for head pain typically aim towards increasing activities that are meaningful as part of increasing overall functioning.
Injury mechanisms of PPTH, such as car accidents, blasts in combat conditions and physical violence, are often traumatic events that can lead to expression of PTSD symptoms. In a trial of CBT for PPTH in veterans (54), 96% had service-connected PTSD subsequent to a blast injury. In such cases, post-traumatic headache pain could serve as a frequent reminder of the traumatic event, exacerbating symptoms. However, it remains unclear whether PPTH and PTSD conditions are more difficult to treat when both are due to the same event.
The generalizability of study results between disparate populations may seem to be a limitation of the articles in the present review, but we argue that generalizability might not be as much of a problem as it may seem. We acknowledge that different mechanisms of injury are predominantly associated with different populations; for example, blast-related trauma is more associated with military populations, and vehicular or sports-related blunt trauma is associated with civilian injuries. In addition, military personnel with mTBI are also more likely to have psychiatric comorbidities than civilians, such as PTSD and depression. However, Nabity et al. (54) found that there were no differences between people with PPTH from blast-only versus blunt-only head traumas, although individuals with blunt-blast compound injuries were significantly more likely to have 15 or more headache days per month. With these qualifications noted, a corollary of the Mutual Maintenance Model is that findings related to pain interventions should be generalizable to any population in which negative affect was associated with pain. The frequency of PTSD or negative affect associated with mTBI represented across studies in the present review may be a common enough through-line to generalize findings, even between disparate military or civilian populations. In those civilian studies where PTSD was not reported, the high observed incidence of depression and/or anxiety associated with mTBI may have been sufficient to perpetuate post-traumatic headaches, and vice versa.
The frequency of comorbid PTSD and PPTH vis-a-vis the shared vulnerability and Mutual Maintenance Model suggests that addressing both conditions together may be critical for effective treatment. CBT may be well-suited to target the various cognitive and emotional processes that underlie the mutual maintenance of these conditions. McGeary et al. (18) found that CBT-H, which addressed both PPTH and PTSD together, was highly effective against both. CBT-H, in conjunction with interdisciplinary care may be the best combination for PPTH rehabilitation: global, integrated approaches that implement CBT modalities were shown to improve both PPTH and PTSD (28,30). However, RCTs are needed to determine the degree of efficacy of interdisciplinary approaches to PPTH and comorbid PTSD.
Designing research to enhance downstream adoption of nonpharmacological interventions
As the research into behavioral and non-pharmacological interventions for PPTH continues to grow, it is vital to ensure that treatments under study are thoughtfully designed and packaged to maximize use in the clinical space. Currently, there is general agreement that non-pharmacological treatments are underutilized for headache management, despite their potential efficacy and comparative safety (55). Reasons for underuse vary but may include stigma associated with seeking treatment for headache, scarcity of practitioners trained in these modalities, time constraints and financial burden or insurance limitations (41,56). To address these obstacles, investigators are encouraged to engage headache patients in the development or adaptation of non-pharmacological interventions for PPTH. This may allow them to directly identify and address perceptions of stigma. As much as possible, investigators are encouraged to minimize the complexity of non-pharmacological treatments (which should ease training burden) and incorporate implementation science toolkits early in treatment development to ensure downstream adoption (57).
Strengths and limitations
As with any systematic review, there is a chance that some relevant articles were missed in the review process. A gray literature search was conducted to help minimize the risk of excluding articles published in English. A prior systematic review (25) covered non-pharmacological interventions for PPTH management; however, they focused on a five-year period and primarily on neurostimulation interventions. By contrast, the present review covers a greater breadth of behavioral interventions over a longer period and includes a deeper discussion about relevant comorbidities such as PTSD.
Additionally, the studies sampled may have been under-represented by findings from civilian populations and over-represented by findings using military ones. PPTH researchers may be recommended to devise more studies with civilian mTBI populations. We posited that mutual maintenance may promote generalizability between civilian and military populations, but to our knowledge, this has not been tested empirically. It may be further advisable in future PPTH studies to control for military exposures (e.g. sample patients equally from civilian and military/veteran populations or healthcare systems).
The present review focused almost exclusively on behavioral treatments for persistent PTH, with one exception noted above (28). Studies evaluating behavioral, non-pharmacological treatments for post traumatic headache in the acute phase of mTBI were scarce. This gap in the literature may be a function the widely held understanding that mTBI often goes unreported. Time to onset of headaches may be highly variable. In most cases of mTBI, symptoms resolve within three months. In that three-month window, pharmacotherapy may be prescribed for headaches, so patients may not be motivated to seek behavioral alternatives until much later. In fact Baker et al. (28) noted that the overall positive results may have been due to normal symptom remission in their mixed acute and persistent headache population. Overall, the review process revealed very few studies evaluating behavioral, non-pharmacological treatments for headaches within three months of mTBI that met the other stipulated inclusion criteria.
Conclusions
Previous evidence showed that PPTH is not satisfactorily managed with the available pharmacological options alone. Behavioral interventions may be effective in augmenting or supplementing traditional drug therapies to manage PPTH symptoms and related disability. Individuals who engaged in CBTs were less disabled and enjoyed improved quality of life. Several psychosocial factors that are associated with PPTH were identified and discussed in this review. Studies evaluating the effectiveness of non-pharmacological or behavioral interventions should implement treatment for comorbid PTSD and/or affective distress. Future research should be aimed at understanding how these psychosocial factors influence treatment outcomes as well as the long-term durability of headache symptom improvements after behavioral, non-pharmacological interventions.
Effective behavioral interventions for PPTH may incorporate cognitive behavioral treatment (CBT) modalities because they address the affective distress often associated with mTBI. Subjective pain intensity has not been reported to be reliably reduced using any behavioral modality reviewed here, however, CBT and related interventional strategies are effective in reducing headache-related disability and improving quality of life outcomes.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251341237 - Supplemental material for Behavioral, non-pharmacological intervention modalities to alleviate persistent headache attributable to traumatic brain injury: A systematic review of patient pain outcomes in the context of the mutual maintenance model
Supplemental material, sj-docx-1-cep-10.1177_03331024251341237 for Behavioral, non-pharmacological intervention modalities to alleviate persistent headache attributable to traumatic brain injury: A systematic review of patient pain outcomes in the context of the mutual maintenance model by Elizabeth M. Sanford, Kristin N. Sramek, Donald D. McGeary and Paul S. Nabity in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by the US Department of Defense through the US Army Medical Research and Materiel Command, Congressionally Directed Medical Research Programs, Psychological Health and Traumatic Brain Injury Research Program award (E01 HT9425-23-1-1046) (PI: Donald D. McGeary, PhD).
Author contributions
Study concept and design: Elizabeth Sanford
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.