
Abstract
Background
Headache-related sick leave is increasing in Norway. In cooperation with the Norwegian Labour and Welfare Administration we established the first Norwegian multidisciplinary headache clinic for patients with current or recurrent sick leave due to headaches. The primary objective of this study was to evaluate treatment effects on headache frequency and sick leave, and secondly to identify predictors for improvement and return-to-work.
Methods
A team comprising neurologists, nurses, physiotherapists, psychologists, and job specialists treated patients aged 18–67 years with headache-related sick leave. Validated questionnaires and semi-structured interviews were conducted at baseline, 3, 6, and 12 months. Mixed effects linear and logistic regression was performed with headache days and sick leave as outcomes.
Results
One hundred and one patients completed the 12-month follow-up. The median monthly headache days decreased from 24 (Interquartile range [IQR], 15.5–30) at baseline to 10 (IQR, 4–20) at 12 months (p < 0.001). Headache-related sick leave declined from 53.5% to 33.7% (p < 0.001). Migraine diagnosis and long-term sick leave at baseline negatively predicted for return-to-work, while female sex and low baseline headache frequency predicted favorable clinical outcomes.
Conclusion
Multidisciplinary treatment reduced headache frequency and increased work attendance. Our findings have potential implications for healthcare policy and resource allocation.
This is a visual representation of the abstract.
Introduction
Migraine and tension-type headache (TTH) mainly affect people during their peak productive years and are associated with substantial societal costs (1). In Europe, indirect costs related to work absenteeism and reduced productivity constitute most of these societal expenses (2,3). In a US study, people with migraine missed nine more workdays per year compared to those without migraine (4). In Norway, people with chronic headache (i.e., ≥15 headache days per month) aged 30–44 lost on average 9.7 workdays over the last three months and 33% were on long-term certified sick leave (> one year) (5). Data from the Norwegian Labour and Welfare Administration show increasing medical certified sick leave rates due to migraine over the past 20 years (6).
Headache disorders are comorbid with a range of conditions, of which several are known risk factors for disease progression and a barrier for improvement (7,–9). These include poorly optimized acute headache treatment, acute medication overuse, anxiety and depression, other chronic pain conditions, sleep problems, obesity, physical inactivity and financial constraints (10,–17).
Despite the availability of pharmacological treatments, many patients experience insufficient treatment response or intolerable side effects (18). Additionally, while non-pharmacological approaches like cognitive behavioral therapy, patient education, relaxation training, physiotherapy, and sleep management show promise; rigorous controlled studies are lacking (18). Some studies suggest that a multimodal approach combining pharmacological and targeted non-pharmacological therapies, delivered by a multidisciplinary team, is more effective than single-modality treatment (10,18,–24).
Studies from Germany and Denmark indicate that multidisciplinary headache treatment is cost-effective and reduces sick leave due to headache (25,26). Given the scarcity of multidisciplinary headache clinics within the public health care system in Norway, we established a multidisciplinary headache clinic in collaboration with the Norwegian Labour and Welfare Administration with special focus on work attendance.
The primary objective of this study was to evaluate the effect on headache frequency and sick leave. Secondly, we studied predictors for clinical improvement and return-to-work.
Methods
Design, setting and study population
This prospective observational study was conducted between September 2020 and December 2022 at Department of Neurology, Akershus University Hospital, Norway. Norway has an all-covering national health insurance, and hospitals are almost exclusively publicly financed. Akershus University Hospital serves approximately 630,000 residents in eastern Norway, this study only included patients aged 18–67 residing in the municipalities Lørenskog and Lillestrøm (population: 130,000). The patients were either referred by their general practitioner, a neurologist or were self-referred. Inclusion criteria were current or recurrent sick leave due to headache. Exclusion criteria were insufficient Norwegian language proficiency or a 100% disability pension. All physicians (general practitioners and specialists in private practice or hospitals) in Norway may certify sick leave of up to one year. The employer covers the first 16 days, after which the Norwegian Labour and Welfare Administration covers the salary costs for up to one year. If the patient's health condition prevents them from working full time, but does not require a complete absence from work, a partial sick leave can be issued. During a partial sick leave, you one can work part-time or with reduced working hours.
Intervention
The multidisciplinary headache team consisted of neurologists with special interest in headache, physiotherapists, headache nurses, psychologists, administrator and job specialists from the Norwegian Labour and Welfare Administration. Patient progress in the project and the specific tasks for the team members are illustrated in Figures 1 and 2. Non-pharmacological interventions for headache disorders can be delivered in different ways and on different schedules. We used existing knowledge from our own and the Norwegian population, available international evidence and looked to expert opinions and guidelines from other countries when we designed the team and the intervention (7,9,12,27,–30).
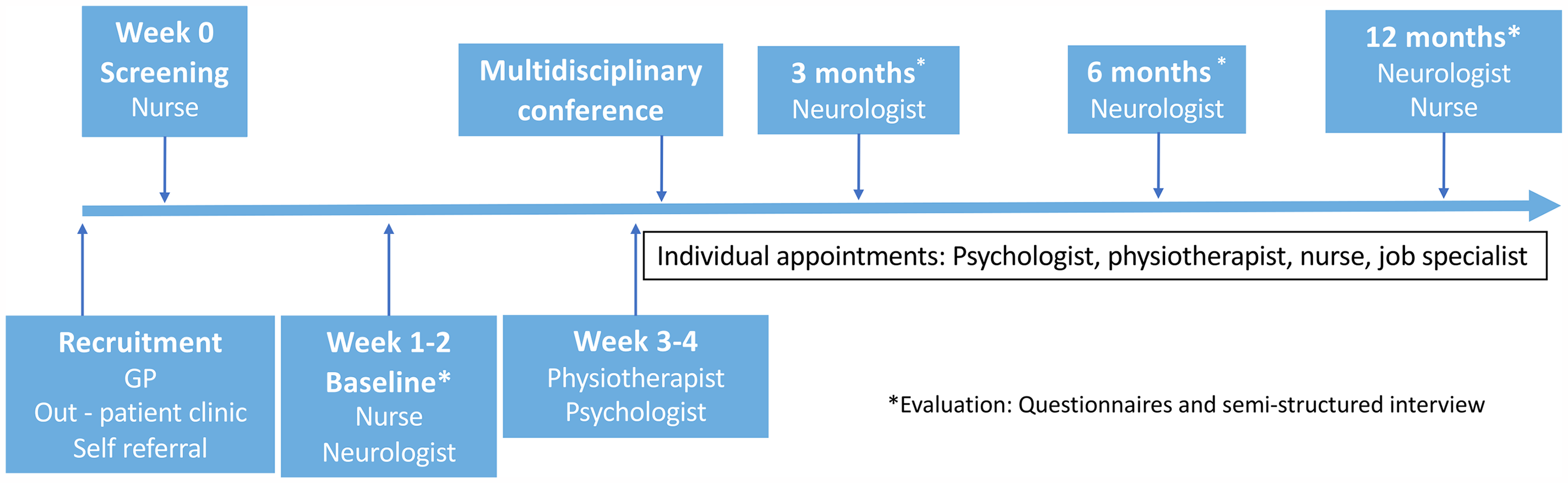
Patient progress during follow-up.

Role and tasks of the multidisciplinary team.
After referral, all patients were contacted by telephone by a nurse who screened for eligibility. The patients had their first appointment with the neurologist and the headache nurse in the clinic within 1–2 weeks after referral. The main tasks for the neurologist were to provide correct headache diagnoses according to the International Classification of Headache Disorders 3rd edition (ICHD-3) and initiate appropriate pharmacological treatment. If secondary headaches were suspected, additional diagnostic testing (i.e., magnetic resonance imaging, blood samples, etc.) was performed. After the initial consultation, all patients were seen by the neurologist at 3, 6 and 12 months to assess the efficacy of the treatment and make any necessary adjustments.
Within two weeks after the initial visit, all patients had their first visit with the physiotherapist and the psychologist. The physiotherapist focused on musculoskeletal factors contributing to headache, providing individualized advice on relaxation, strength, and endurance exercises. Passive treatments were avoided. The psychologist addressed psychosocial factors, comorbid psychiatric disorders, and provided personalized psychotherapeutic interventions, including cognitive behavioral therapy and psychoeducation to manage stress, pain, and emotions. Follow-up by the physiotherapist and the psychologist was based on the patient's individual need and included regular individual in-person sessions.
The nurses were “the hub” of the team. They participated in first consultations with the neurologist, lead the multidisciplinary team conferences and had telephone consultations when needed between neurologist-visits. Patients with medication overuse headache had additional consultations with the headache nurses during withdrawal.
Patients were referred to a job specialist appointed by the Norwegian Labour and Welfare Administration in cases where working conditions were considered a significant contributor to headache and sick leave, or when the patients’ headache was not compatible with their current type of work tasks or occupation. The job specialists collaborated with the patient and employer to identify strategies and accommodations that would facilitate the patient's continued employment.
The administrator oversaw logistics and scheduling to ensure timely appointments. After the first appointment with the neurologist, nurse, psychologist and physiotherapist, an individual plan for each patient was made in a multidisciplinary team conference.
Data collection
At the initial consultation, the neurologists conducted a semi-structured interview to gather information on demographics, headache characteristics, treatment history, and comorbidities. Shorter versions of this interview were repeated at 3, 6, and 12-month follow-up visits.
Additionally, patients completed self-administered questionnaires at each follow-up. The questionnaires comprised of validated questionnaires as well as questions about headache frequency and intensity, and sociodemographic data, including occupation, and medically confirmed sick leave. All patients used electronic headache diaries during the follow-up period.
Psychological distress was assessed with the Hospital Anxiety and Depression Scale (HADS) (Mapi Research Trust, Lyon, France, https://eprovide.mapi-trust.org), validated for use in a Norwegian population (31). This scale consists of 14 items measuring symptoms of anxiety and depression experienced during the last week. Seven questions specifically address symptoms of anxiety (HADS-A) whereas the other seven questions pertain specifically to symptoms of depression (HADS-D). The items are rated on a 4-point scale (0–3), yielding two scores, one for anxiety and one for depression, each ranging from 0 and 21. A HADS subscale score (i.e., HADS-A or HADS-D) ≥8 indicates considerable symptoms of anxiety or depression (31).
Patients also responded to the simple yes/no question: “Are you in control of your headache?”
Statistics
We used Wilcoxon's signed-rank test to compare continuous data and McNemar's test for categorical variables from baseline to 12-month follow-up. Statistical analyses were performed using IBM SPSS Statistics (Version 29.0.0.0 (241) SPSS Inc., Chicago, IL).
We additionally performed mixed effects linear regression with days of headache at 3, 6 and 12 months as outcome, adjusting for baseline headache frequency and other predictors at baseline (migraine, sex, age, preventive medication and HADS). We performed mixed effects logistic regression with sick leave at 3, 6 and 12 months as outcome, adjusting for baseline sick leave and other predictors at baseline (sex, age, months on sick leave, chronic musculoskeletal pain and HADS). Additional analyses were performed with mixed effects negative binomial regression with days of headache at 3, 6 and 12 months as outcome and mixed effects linear regression with percentage (0–100%) of sick leave at 3, 6 and 12 months as outcome. All analyses were performed starting with the six predictors mentioned and number of predictors were reduced based on values of Akaikes information criterion (AIC). All regressions were performed with the package lme4 in RStudio (version 2024.04.1), using R (version 4.4.0).
Ethics
The study was approved by the Regional Committee for Medical Research Ethics South-East Norway (B/97324, May 19, 2020) and the Data Protection Officer at Akershus University Hospital. All participants provided written informed consent.
Results
Baseline
A total of 119 patients were screened, 111 met to the baseline visit and 101 completed the 12-month follow-up (Figure 3). The ten patients who did not complete the 12-month follow-up were comparable to the completers in terms of headache diagnoses, headache frequency, comorbidity, age, and sex; however, only one was currently on 100% sick leave at baseline. All the results are presented for the 101 patients who completed the study.
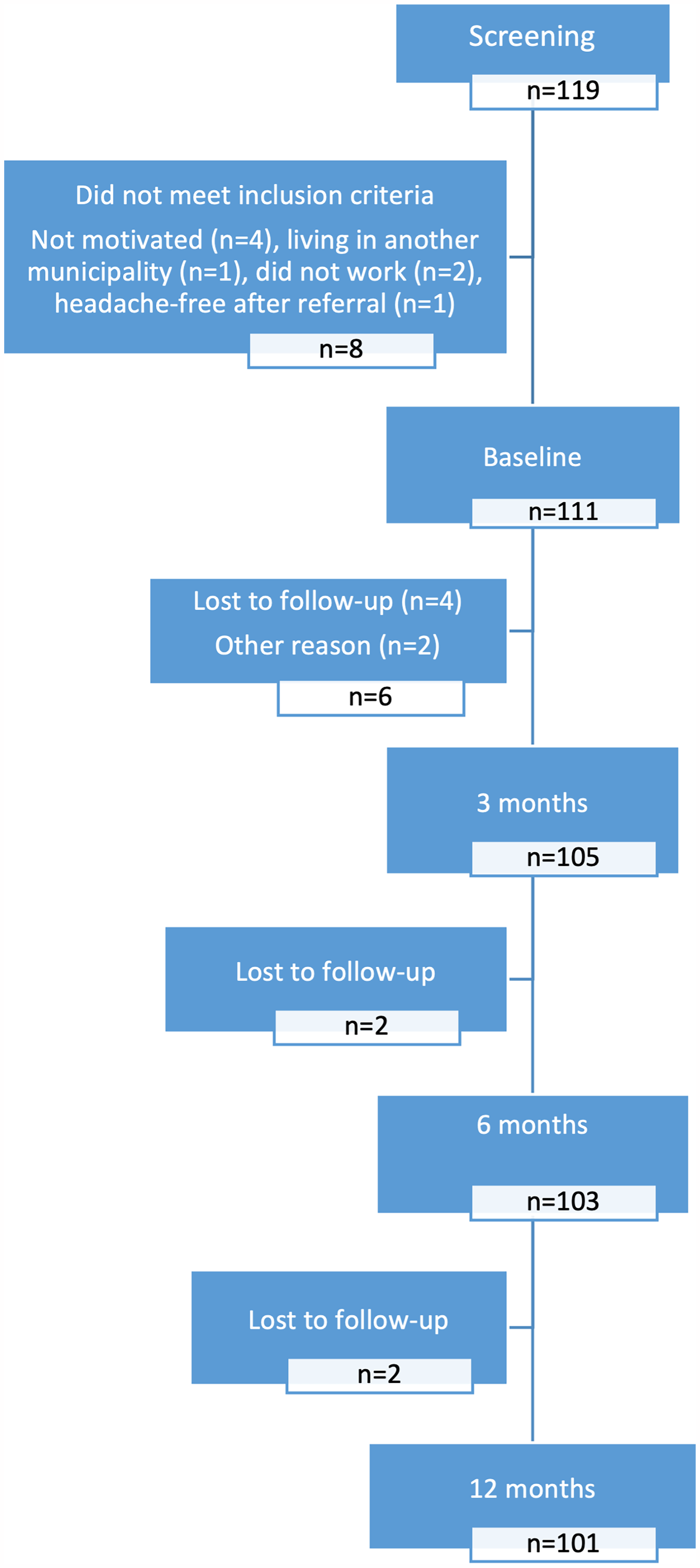
Flow chart of the study.
Eighty-seven (86.1%) patients were women, with a mean age of 38.5 years (SD 11.5) (Table 1). Migraine was the main headache diagnosis in 84 (83.2%) patients, followed by TTH in 14 (13.9%) patients. The co-occurrence of migraine and TTH was found in 18 patients and in four of these patents TTH was the main diagnosis. The patients had on average had headache for 17.6 (SD 11.9) years and 81 (80.2%) had chronic headache, defined as ≥15 headache days per month at baseline. According to the ICHD-3 criteria, 16 patients (15.8%) had medication overuse headache. All patients with acute medication overuse had chronic migraine.
Baseline demographic and clinical characteristics of completers (n = 101).

≥15 headache days per months.
According to ICHD-3.
Some patients used more than one preventive drug.
Of the 101 patients, 67 (66.3%) had previous experience of preventive pharmacological treatment. The most common treatments were candesartan (46.5%), amitriptyline (44.6%) and beta-blockers (42.6%). The main reasons for discontinuation were lack of efficacy (62% for candesartan, 45% for amitriptyline and 76% for beta-blockers) and side effects (19% for candesartan, 27% for amitriptyline and 14% for beta-blockers). In addition, four patients had discontinued treatment with CGRP monoclonal antibodies, and 11 patients had discontinued treatment with onabotulinum toxin due to lack of efficacy.
Sixty-seven patients (66.3%) had used non-pharmacological treatments such as physiotherapy, chiropractor, acupuncture, and different kinds of complementary and alternative treatments for headache (Table 1). However, 15 (14.8%) had only tried non-pharmacological treatments, and 19 (18.8%) had not tried any treatment at all. At baseline, 46 (45.5%) of all patients and 40 (48.2%) of those with chronic headache were on preventive medication. Notably, 45 (44.6%) had never consulted a neurologist.
The most common comorbidities were anxiety and chronic musculoskeletal pain (Table 1). At baseline, 54 (53.5%) currently had medically confirmed sick leave because of headache, with a median duration of 8.5 (SD 10.7) months.
Headache, sick leave and psychological distress
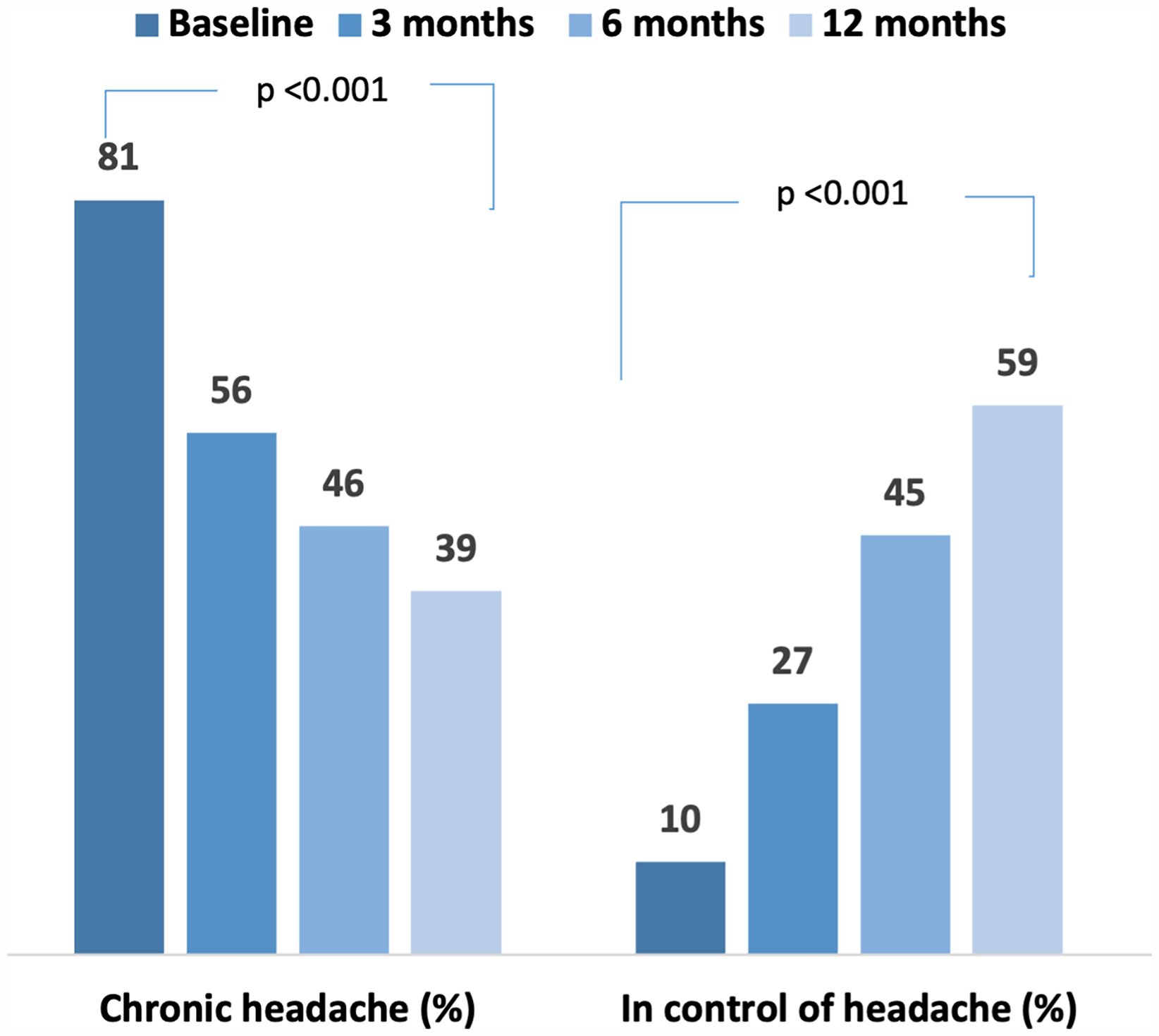
The median number of headache days per month decreased from 24 (interquartile range [IQR], 15.5–30) at baseline to 10 (IQR, 4–20) at 12 months (p < 0.001) (Table 2). Similarly, the proportion of patients with chronic headache declined from 81 (80.2%) to 39 (38.6%) (p < 0.001) (Figure 4). A significant reduction in the number of medication days and pain intensity scores were also observed (Table 2). A total of 51 (50.5%) had at least 50% reduction in the number of headache days and 36 (35.6%) had at least 75% reduction in headache days per month.
Changes from baseline through the follow-up period.
Course of headache and psychological distress (n = 101).

Baseline vs 12 months. Wilcoxon Signed rank test.
HADS-A and HADS-D; The Hospital Anxiety and Depression Scale Anxiety (A) and Depression (D).
The number of patients on sick leave due to headache decreased gradually and significantly from 54 (53.5%) at baseline to 34 (33.7%) after 12 months (p < 0.001) (Figure 5). The proportion of patients on partial sick leave after 12 months was higher than the proportion of those on 100% sick leave.

Changes in 100% sick leave (blue) and partial (orange) from baseline through the follow-up period.
We observed a significant reduction in HADS-A scores from baseline to 12 months from 8 (IQR, 4–10) at baseline to 7 (IQR, 4–9), p = 0.004. Likewise, there was a significant reduction in HADS-D scores from 6 (IQR 3–9) to 5 (IQR 2–8), p = 0.005.
An increasing proportion of patients reported that they were in control of their headache (Figure 4).
Predictors
Headache frequency at baseline and sex were significant predictors of headache days in a linear regression model (Table 3). Our results suggest that being female is a strong predictor of greater reduction in headache days (beta = −5.29, 95% CI: −8.45, −2.13), p < 0.001. In additional analysis utilizing that headache frequency is count data, negative binomial regression revealed a strong association between migraine diagnosis and higher headache frequency at 12 months (Online Supplemental Table S1). Pharmacological preventive treatment did not significantly improve the model fit according to AIC and was therefore excluded from the analysis. While baseline HADS scores had some explanatory value according to AIC, these were not statistically significant.
Predictors for headache days per month, mixed effects linear regression model (n = 101).

HADS; Hospital Anxiety and Depression Scale.
Predictors for sick leave, mixed effects logistic regression model (N = 101).

HADS; Hospital Anxiety and Depression Scale.
Logistic regression analysis of headache-related sick leave revealed a significant association between the duration of sick leave at baseline and sick leave at 12 months (OR = 1.03, 95% CI 1.02, 1.04) (Table 4). Migraine was also associated with increased risk of sick leave at 12 months (OR 3.36, 95% CI 1.30, 9.38). Linear regression analysis, examining the percentage of sick leave at 12 months, utilizing that in Norway one can have gradual sick leave (i.e., 10–90%), showed a significant increase in individuals with a migraine diagnosis and longer baseline sick leave periods (Online Supplemental Table S2). Although sex, age and baseline total HADS score emerged as potential explanatory variables in AIC-based analyses, these associations did not reach statistical significance.
Discussion
Our findings indicate that treatment in a multidisciplinary headache team effectively reduces headache frequency, sick leave, and psychological distress among patients with frequent or recurrent sick leave due to headache. Female sex and lower baseline headache frequency were associated with better clinical outcomes. Conversely, migraine and long-term sick leave at baseline were predictors of persistent sick leave after 12 months. Our study demonstrates the feasibility of establishing multidisciplinary headache teams within Norway's public healthcare system.
Interpretation and comparison with other studies
Our findings align with previous studies demonstrating that a multidisciplinary approach reduces headache burden, psychological distress and sick leave due to headache (25,26). A reduction of 14 headache days per month is highly clinically significant and was accompanied by a reduction in symptoms of anxiety and depression, which are common comorbidities in people with headache (29). While direct comparisons with others are challenging due to varying methodologies and healthcare systems, our results are comparable to those reported from Germany and Denmark (25,26). Notably, in Germany a 30% reduction in healthcare costs compared to standard care was reported, while the Danish study noticed a two-day reduction in monthly sick leave days (25,26).
While most research on multidisciplinary headache treatment originates from tertiary headache centers–which are unavailable in Norway–our patient cohort, included due to headache-related sick leave, presented with comparable severity. This was evidenced by a high prevalence of chronic headache (80%), a long headache history (mean 17.6 years), and extensive prior experience with various pharmacological and non-pharmacological treatments (22,26,–30). Consistent with findings in other conditions (32,33), we found that long-term sick leave at baseline predicted poorer work participation outcomes at 12 months, emphasizing the importance of early intervention for individuals on sick leave. Because multidisciplinary headache teams are typically situated within tertiary centers–where patients often face lengthy waiting times–accessing this care can be problematic. The combination that these patients experience of significant disability and this delay can contribute to workforce dropout, underscoring the need to provide multidisciplinary treatment at a lower level of the healthcare system (34).
In contrast to previous studies (23–26), a significant majority (82%) of our patients had migraine as their main diagnosis, with 71% experiencing chronic migraine. This prevalence is higher than reported in earlier studies, which may be due to differences in classification used (ICHD-2 vs. ICHD-3). Somewhat surprisingly, a migraine diagnosis was associated with worse headache outcome in this population, despite the availability of new pharmacological preventive treatments for migraine (35). The proportion of patients with medication overuse headache was somewhat lower in our study (16%) compared to the 25–34% reported by others (24,26). This difference could be attributed to increased awareness among patients and healthcare providers, local treatment practices or simply by coincidence. No headache types were excluded in the present study, but due to the limited number of participants, migraine and TTH were the most common diagnoses. Other primary and secondary headache diagnoses may also benefit from multidisciplinary headache treatment. Despite the high prevalence of chronic headache, only 45.5% of patients received preventive pharmacologic treatment at baseline. Pharmacological underuse is a well-known problem in for chronic headache patients in Norway (30). A recent study from the Norwegian Prescription Register reported that only 55.9% of people who had taken triptans ≥ 16DDD in three consecutive months (used as proxy for chronic migraine) received a prescription for a preventive medication in the same year (33).
Our patients presented with a high burden of comorbidities, including chronic musculoskeletal pain, anxiety, depression and insomnia. These conditions often coexist with chronic headache and can significantly influence headache treatment outcomes (13,27). Two-thirds had previously tried various pharmacological and non-pharmacological treatments, though not in a coordinated way. The tailored individual approach from coordinated therapists, including the involvement of job specialists, likely contributed to the significant reduction in headache-related sick leave observed over the 12-month follow-up period. Addressing headache together with the comorbidities within a work-focused multidisciplinary framework may have additional benefits, as psychological and musculoskeletal disorders account for a substantial proportion of sick leave in Norway and other European countries (6,36).
The patients in our study had more consultations with the psychologist than the physiotherapist, which was similar to a German study reporting that 43% of patients were seen by a psychologist compared to 11% by a physiotherapist (37). Our patient had baseline HADS values in the range of what is often considered cut-off for clinically relevant anxiety and depression (31). This underscores the importance of addressing psychological factors when establishing a multidisciplinary headache team.
The majority of our patients were women (86%), which is more than expected from prevalence figures (38), but aligns with the observation that women with migraine are more severely affected and more likely to seek medical attention (39). Our inclusion criteria, which focused on patients with current or recurrent sick leave, may additionally have contributed to the higher proportion of women, as women in Norway and most other European countries have higher rates of sick leave compared to men (36). Half of our female patients were employed in sectors such as education and healthcare, traditionally female-dominated fields often characterized by demanding, inflexible work environments. While research suggests that sex-differences in sick leave are not solely due to occupational factors (6), these professions may pose additional challenges for individuals with headache disorders. However, similar to the Danish study, female sex was a strong predictor for clinical improvement (26). This result might have been influenced by the above-mentioned sex differences in both sick leave and medical-seeking behavior, potentially leading to inclusion of more severely affected men. This may also be a by chance finding because of few included men. We may also have designed our intervention to be more attractive to women, or we could have addressed issues that are more relevant to women.
A high number of headache days at the beginning of the study was a predictor of a high number of headache days after 12 months. This is not surprising as these patients already have a greater headache burden on admission to multidisciplinary treatment and this finding has been reported by others (26). This group may be particularly suitable for multidisciplinary treatment as they require a combined approach of non-pharmacological and pharmacological treatment.
Strengths and limitations
Controlled study designs are difficult to apply in multidisciplinary headache treatment, due to multiple and individualized interventions (26). Analogous to previous studies, we do not have a control group for comparison with standard care, our results will therefore likely overestimate the causal effect of the intervention. However, given our patients’ long-standing history of headache (almost 18 years), it is unlikely that the observed improvements were due to spontaneous remission. Similar to previous studies, our interventions were not standardized, and all patients received a personalized combination of multiple pharmacological and non-pharmacological treatments. Consequently, it is difficult to attribute specific outcomes to each type of intervention. Based on the lack of a control group, cost-effect-analyses could not be performed. However, we hope to conduct a controlled trial where both individual and societal outcomes will be included. We did not measure work presentism. This is a relevant measurement, especially for chronic conditions whose symptoms and intensity vary from day to day, such as migraine and headaches (2). No work presentism instrument validated for headache exists, but this should be developed and included in future studies to get an even more detailed picture of headache related costs and work presentism/absenteeism. Due to few cases without migraine and a small number of men, we could not perform subgroup analyses based on different headache diagnoses or present results for men and women separately. Exclusive participation of highly motivated patients could easily bias our results towards more positive outcomes. However, the patients were not invited but referred to our clinic–either by their general practitioners, by our outpatient clinic, by private neurologists or self-referred.
Methodological strengths of the present study are that data was collected prospectively, and the diagnoses were set by headache specialists, ensuring that the diagnoses are accurate and consistent. Further, few patients were lost to follow-up.
Lessons learned and suggestions for the future
The project was conducted during the COVID-19 pandemic and due to restrictions, many appointments in the clinic were delayed or cancelled (40). Despite these obstacles, half of the patients no longer required multidisciplinary follow-up (i.e., additional and coordinated consultations with other therapists) after the six-month consultation with the neurologist. Consequently, we have now shortened the multidisciplinary follow-up period from 12 to six months in our clinic. Follow-up by the neurologist for pharmacological treatment is continued as long as needed. To optimize resource allocation, headache nurses are now providing individual consultations and follow-up, reducing the need for neurologist appointments. Additionally, we have implemented a limit of five consultations with physiotherapists and psychologists to accommodate more patients. Patients requiring specialized or long-term therapy will be referred to appropriate external providers.
To further enhance our services for the future, we have developed a group-based intervention led by psychologists, incorporating sessions with neurologists, physiotherapists, nurses, and job experts. This seven-week program, consisting of seven sessions of 2.5 h each, will be evaluated separately.
Conclusion
Our findings demonstrate that treatment in a multidisciplinary headache team effectively reduces headache burden and improves work attendance among patients on sick leave due to headache. Traditionally, multidisciplinary care has been considered a “last resort” for severe, treatment-resistant headache in tertiary care. Our study suggests that earlier intervention, while patients are still employed and not on disability benefits, may help to reduce the headache burden for a large group of patients. This approach has important implications for healthcare policy and resource allocation.
Clinical implications
Treatment within a multidisciplinary headache team effectively reduces headache frequency, sick leave, and psychological distress in patients with present or recurrent headache-related sick leave Female sex and lower baseline headache frequency were associated with better clinical outcomes Migraine diagnosis and long-term sick leave at baseline predicted persistent sick leave after 12 months.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251332572 - Supplemental material for Multidisciplinary headache treatment with work-focus in Norway: An observational study
Supplemental material, sj-docx-1-cep-10.1177_03331024251332572 for Multidisciplinary headache treatment with work-focus in Norway: An observational study by Oda V Lunder, Torbjørn Wisløff, Linn-Marie Wølneberg, Aina Kristin Paulsen, Linda Hagen Aasbakken, Inger Louise Hole, Ingvild Vøllo Eliassen, Kjersti Aaseth, Espen S Kristoffersen and Kjersti G Vetvik in Cephalalgia
Footnotes
Acknowledgements
Special thanks to job specialists Wenche Frimann-Jakobsen og Odd-Arne Sandvik from the Norwegian Labour and Welfare administration and physiotherapists Merete Sørdahl and Mari Norrøne who participated in the multidisciplinary team in the initial phase of the project.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KGV has received honoraria for lecturing and/or participation in advisory boards from Novartis, TEVA, Roche, Pfizer, Lundbeck, Eli Lilly and Abbvie. ILH has received honoraria for lecturing from Abbvie and TEVA. AKP has received honoraria for lecturing from Abbvie. KA has received honoraria for lecturing from Lundbeck. ESK, OVL, L-MW, LHA, IVE and TW have no conflict of interest to disclose.
Ethical statement
The study was approved by the Regional Committee for Medical Research Ethics South-East Norway (B/97324, May 19, 2020) and the Data Protection Officer at Akershus University Hospital. All participants provided written informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Akershus Universitetssykehus, (grant number Strategic research allocations (grant number 2024/).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.