
Abstract
The aim of this large, cross-sectional, population-based study was to examine the association between sick leave and headache. Between 1995 and 1997, all 92 566 adults in Nord-Tr⊘ndelag County in Norway were invited to participate in a health survey. Out of 73 327 invited individuals <67 years old, a total of 38 192 (52±) responded to questions about headache, work situation and sick leave during the past year. Associations between sick leave, headache and migraine included were assessed in multivariate analyses, estimating prevalence odds ratios (ORs) with 95± confidence intervals (CIs). There was an increasing prevalence of sick leave with increasing frequency of migraine and non-migrainous headache. The prevalence of sick leave >8 weeks during the past year was more than three times higher among individuals with headache >14 days per month (20±) compared with those without headache (6±). The results may indicate that better treatment of individuals with chronic headache may have beneficial economic implications.
Introduction
Headache is a very prevalent disorder and particularly affects adults in their most work productive ages around 20–50 years old (1, 2). Headache suffering may lead to reduced work capacity which results in indirect costs to society (3). Sick leave due to headache may be easier to assess than reduced work productivity and some population-based studies have reported that 7–15% of working individuals had been absent from work in the previous year due to headache (3–6). Most studies have evaluated sick leave among migraine patients and the number of days missed per year in migraine patients seems to vary between 2 and 6, with an average of 2.5 working days per year (7–9). The impact of non-migrainous headache and headache frequency on sick leave is less known. As far as we know, no population-based study has evaluated sick leave in headache patients compared with headache-free individuals.
The aim of this large population-based study was to evaluate the association between sick leave and headache diagnosis and between sick leave and frequency of headache.
Materials and methods
Population
Between 1995 and 1997, all inhabitants aged ≥20 years in Nord-Tr⊘ndelag county in Norway were invited to participate in the Nord-Tr⊘ndelag Health Study (the HUNT study). The invitation letter was sent by mail enclosed with a three-page questionnaire (Q1) and an information folder. The Q1 was to be completed prior to the screening and returned at attendance to the screening site. A second questionnaire (Q2) was handed out at the screening site and should be completed and returned by mail. Among the wide range of topics, the questionnaires included questions about headache, working situation and sick leave. The study population, including both participants and non-participants, has been described in detail previously (1, 10, 11).
Headache diagnosis
The headache questions in Q2 were designed mainly to determine whether or not the person suffered from headache, the frequency of headache, and to diagnose migraine according to a modified version of the migraine criteria of the Headache Classification Committee of the International Headache Society (IHS) (12). Subjects who answered ‘yes’ to the question ‘Have you suffered from headache during the last 12 months?’ were classified as headache sufferers. Based on the data from the subsequent 12 headache questions (1, 13), they were classified into two groups with either migraine or non-migrainous headache. The diagnoses were mutually exclusive. Persons were classified as migraineurs if they reported having migraine or fulfilled the following three criteria: (i) headache attacks lasting 4–72 h (<4 h was accepted for those who reported frequent visual disturbances before headache); (ii) headache with at least one of the following characteristics: (a) pulsating quality, (b) unilateral location, (c) aggravation by physical activity; (iii) during headache, at least one of the following: (a) nausea, (b) photophobia and/or phonophobia. Persons who did not fulfil the criteria for migraine were classified as headache sufferers with non-migrainous headache. Headache frequency was divided in three categories; <7days/month, between 7 and 14 days/month and >14 days/month. The classification of subjects in the present study has been previously described in detail and the questionnaire-based diagnoses have been validated by interview diagnoses (13). In short, for migraine, the positive predictive value (PPV) was 84% and the negative predictive value (NPV) was 78%, for non-migrainous headache the PPV was 68% and the NPV was 76%, and for headache >14 days, the PPV was 71% and the NPV was 90% (13).
Musculoskeletal complaints and psychiatric disorders
Individuals who answered ‘yes’ to the question ‘Have you during the last year continuously for at least 3 months had pain and/or stiffness in muscles and joints?’ in Q1 where defined as having chronic musculoskeletal complaints (MSCs) (14).
Self-rated level of anxiety and depression was measured by the Hospital Anxiety and Depression Scale (HADS). Individuals with HADS anxiety scores ≥11 and/or depressive scores ≥11 were defined as having anxiety and/or depression (15).
Sick leave
In Q2, the participants were asked if they had had sick leave during the past year. Those who responded ‘yes’ where then asked to indicate the number of days with sick leave, with three choices of response: ≤2 weeks (‘short-term’), 2–8 weeks (‘intermediate’), and >8 weeks (‘long-term’). In Q1, individuals who reported chronic MSC were also asked if the musculoskeletal pain had forced them on sick leave during the past year and a positive answer was used to assess the internal consistency of self-reported sick leave.
Working situation
In Q1, the participants were asked to tick off one or several out of the following six alternatives: (i) paid work, (ii) self-employed, (iii) full-time household workers, (iv) in military service or student, (v) unemployed or made redundant, or (vi) receiving social security or disability pension. They were also asked to state the number of working hours per week, and individuals working more than 30 h per week were classified as full-time workers. In Q2, the participants reported their occupation (10 categories). They were also asked if they had been without income from work during the past year.
Response rate
Out of 92 566 eligible individuals, 64 560 (70%) participated. A total of 73 327 invited individuals were <67 years old (the upper pension qualifying age in Norway) and of these, 38 192 (52%) responded to questions about headache, working situation and sick leave during the past year. Of these 38 192 individuals, 29 369 (77%) had had paid work during the past year (Fig. 1).
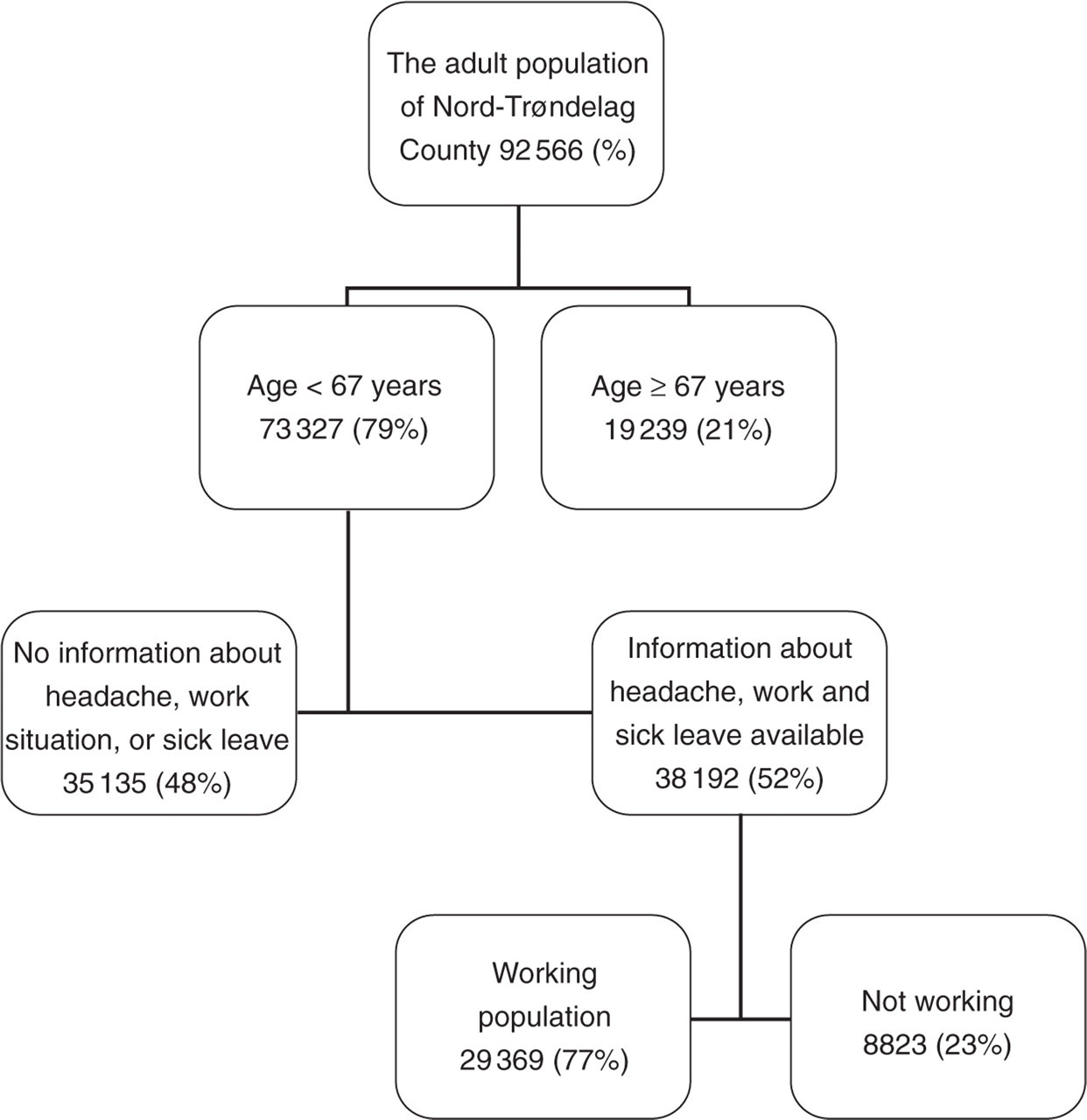
The population according to type of participation.
Ethics
The study was approved by the Regional Committee for Ethics in Medical Research and by the Norwegian Data Inspectorate.
Statistical analysis
Differences between proportions were analysed by χ2 tests. For continuous variables, differences between means were tested with analyses of variance (one-way
The internal consistency between self-reported sick leave due to chronic MSCs in Q1 and their response to the question about sick leave in Q2 was evaluated. In the multivariate analyses using multiple logistic regression, we estimated the prevalence odds ratio (OR) for the association between the specific headache subtypes and the sick leave categories. The precision of the OR was estimated with 95% confidence interval (CI). We evaluated potential confounding by adjusting for gender, age (5-year categories), years of education (three categories: <10, 10–12 and >12), occupation type (white and blue collar workers), self-rated level of anexity and depression, and chronic MSCs. Potential confounding factors were included in the multiple logistic regression analyses separately or together, but were excluded from the final analyses if the OR changed by <0.1. Gender, age, educational level, anxiety and depression and chronic MSCs stood out as important confounders and all final analyses were therefore adjusted for these factors.
When appropriate, sick leave categories were treated as a continuous variable and were incorporated in a two-sided test for trend to evaluate the probability of a linear relation between sick leave categories and headache (‘dose–response relationship’).
The participants were asked about total sick leave (not specifically about sick leave due to headache). A rough estimate of the sick leave due to headache was calculated by subtracting the proportion with sick leave in those who suffered from headache from the proportion of sick leave in the headache-free individuals. We also calculated a rough estimate of number of days with sick leave in total and due to headache during the previous year. In this calculation, the mean number of days with sick leave in the three categories (short-term, intermediate and long-term) could not be estimated directly. In lieu of that, we used two different mean numbers of days, a minimum estimate, and probably a more realistic one. For short-term sick leave (<2 weeks) the estimated mean number of days were 1 day (minimum) and 7 days, for ‘intermediate’ sick leave (2–8 weeks) 14 days (minimum) and 35 days and, finally, for long-term sick leave 57 days (minimum) and 70 days, respectively.
Statistical analyses were performed using the Statistical Package for the Social Sciences, version 13.0 (SPSS, Chicago, IL, USA).
Results
Proportion of sick leave
Among 29 369 individuals with paid work during the previous year, 12 592 suffered from headache and, of these, 7020 (56%) reported sick leave during the past year. The proportion with sick leave was significantly higher among migraineurs (59%) than among those with non-migrainous headache (54%) and headache-free individuals (44%) (P < 0.001). In all age groups the proportion with short-term (<2 weeks) and long-term (>8 weeks) sick leave was higher for individuals with migraine and non-migraineous headache compared with headache-free persons (P < 0.01) (Fig. 2).

Unadjusted prevalence of sick leave (%) by age among individuals with migraine, non-migranous headache and headache-free persons.
For both genders the proportion with intermediate and long-term sick leave increased with increased headache frequency (Fig. 3). The highest proportion of long-term sick leave during the past year was found among women with headache >14 days per month (21%).

Unadjusted prevalence of sick leave (%) by headache frequency among women and men.
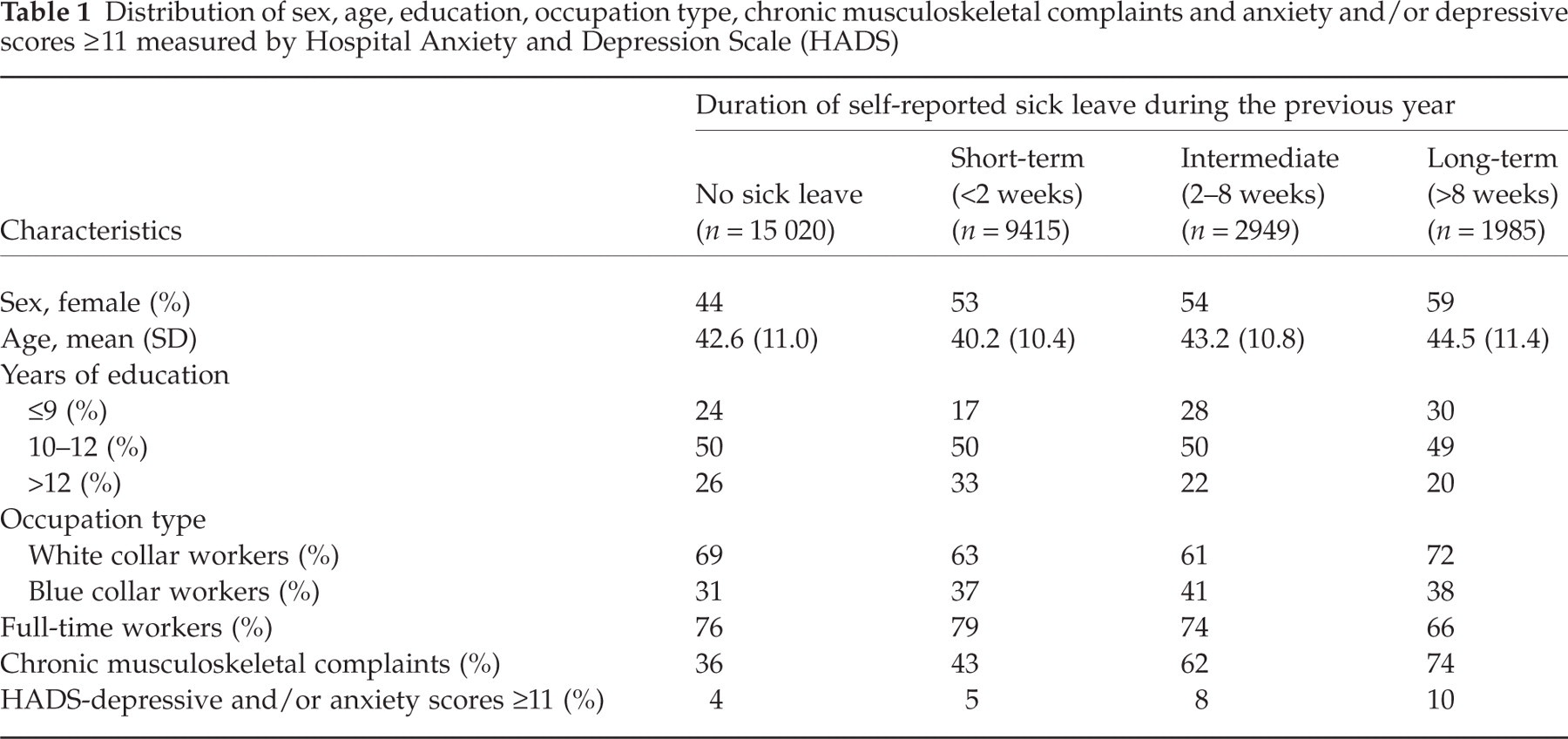
As demonstrated in Table 1, the group of individuals with sick leave >2 weeks during the past year were older, had a higher proportion of blue collar workers and individuals with low educational level, were less likely to be full-time workers, had more chronic MSCs and experienced more anxiety and depression measured by HADS compared with those without sick leave. Individuals without headache or chronic MSCs and with HADS scores <11 had the lowest prevalence of sick leave between 2 and 8 weeks (6%) and for >8 weeks during the past year (3%), whereas the highest prevalence was found among the 631 individuals with headache combined with chronic MSCs and with HADS scores ≥11 (20% and 18%, respectively) (Fig. 4).
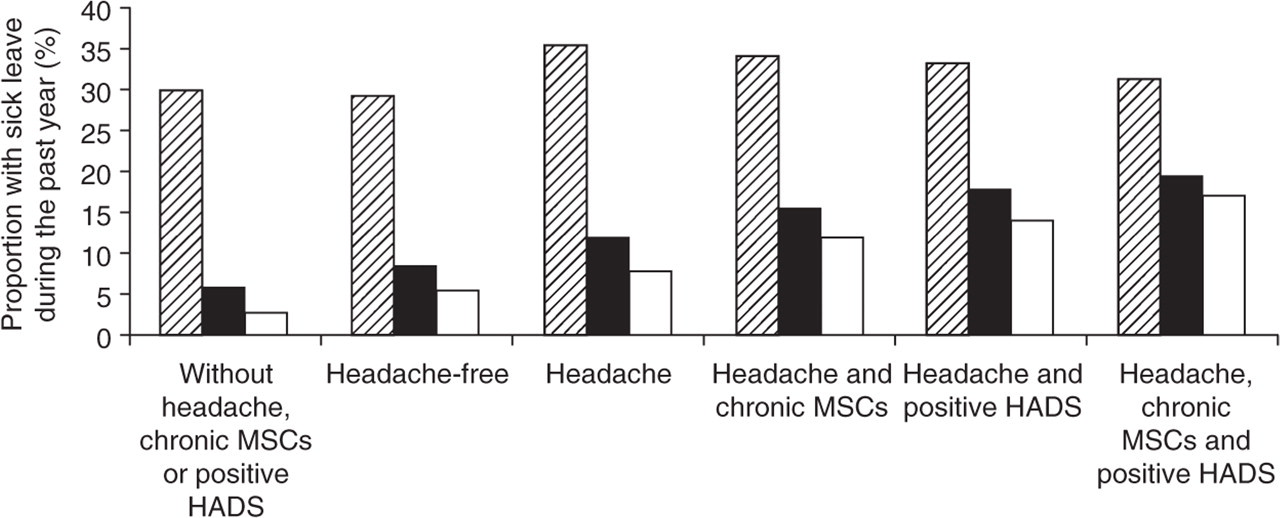
Unadjusted prevalence (%) of sick leave (<2 weeks, 2-8 weeks, and >8 weeks during the past year) in different diagnostic categories separated by presence or absence of headache, chronic musculoskeletal complaints (MSCs) and Hospital Anxiety and Depression Scale (HADS) depressive scores and/or anxiety scores ≥11 (= positive HADS). Hatched, sick leave <2 weeks; ▪, sick leave 2–8 weeks; □, sick leave >8 weeks.
Distribution of sex, age, education, occupation type, chronic musculoskeletal complaints and anxiety and/or depressive scores ≥11 measured by Hospital Anxiety and Depression Scale (HADS)
In the multivariate analyses, adjusting for such confounding factors as gender, age, education, chronic MSCs and psychiatric disturbances, there was a linear trend (P < 0.001) for increasing prevalence of sick leave with increasing frequency of headache (both migraine and non-migrainous headache). Long-term sick leave (>8 weeks) during the past year was more than three times more likely (OR = 3.5, 95% CI 2.7, 4.5) among individuals with headache >14 days past month compared with those without headache (Table 2).
Prevalence odds ratio (OR) of sick leave (<2 weeks, 2–8 weeks and >8 weeks during the past year) amongst subjects with migraine and non-migranous headache related to headache frequency and compared with headache-free individuals (adjusted for gender, age, education level, chronic musculoskeletal complaints and depression and anxiety disorders)

Total number =28 830 individuals (out of 29 369, 539 headache sufferers did not report headache frequency).
Internal consistency
The internal consistency of self-reported sick leave was evaluated among the 3459 individuals who answered ‘yes’ to the question about sick leave due to chronic MSCs in Q1. Of these, a total of 3188 (92%) also confirmed sick leave in Q2.
Sick leave due to headache
Among the 29 369 working individuals, a total of 9415 (32%) reported sick leave for <2 weeks, 2949 (10%) for 2–8 weeks, and 1985 (7%) for >8 weeks. Headache sufferers reported a higher prevalence of sick leave than headache-free individuals and the difference in prevalence was 6.2% for <2 weeks’, 3.4% for 2–8 weeks’ and 2.5% for >8 weeks’ sick leave during the past year, respectively. Supposing that headache was the main medical reason for this difference, the number of individuals with sick leave due to headache were 781 (<2 weeks), 428 (2–8 weeks) and 315 (>8 weeks), respectively. If the mean number of days with absence from work was 7 days among those with <2 weeks’ sick leave, 35 days among those with 2–8 weeks and 70 days for those with >8 weeks during the past year, a total of 42 497 working days was lost due to headache the past year, or 1447 working days per 1000 employed person in a year, or 14% of the total 308 070 working days lost because of sick leave during the previous year. Among the headache patients the estimated mean number of days lost per year due to headache was 3.4 days (Table 3). Individuals with migraine and non-migrainous headache for >14 days per month both had approximately 2 weeks with lost work days due to headache (Table 3).
Number of lost work days per year due to headache in different headache categories

In the rough estimates we assumed that headache was the main medical reason for this difference in prevalence of short- and long-term sick leave between headache patients (migraine or non-migrainous headache) and headache-free individuals. The calculations were based on the following mean number of days: 7 days for short-term sick leave (<2 weeks), 35 days for ‘intermediate’ sick leave (2–8 weeks) and 70 days for long-term sick leave (minimum estimates based on 1, 14 and 57 days, respectively).
A minimum estimate supposing the mean number of days with sick leave to be 1, 14 and 57 days, respectively, gave 24 728 working days lost due to headache the past year, or 842 working days per 1000 employed person in a year, or 15% of the total 161 861 work days lost because of sick leave during the past year. Based on the minimum estimates, the mean number of days lost per year due to headache was 2.0 days (Table 3).
Discussion
In this large, unselected population-based, cross-sectional study, duration of sick leave was positively associated with frequency of migraine and non-migrainous headache. The highest proportion of long-term sick leave was found among headache sufferers with coexisting chronic MSCs and psychiatric disorders.
This is the first population-based study demonstrating an increasing proportion of intermediate and long-term sick leave with increasing headache frequency. In accordance with the present study, subjects with chronic tension-type headache reported more lost workdays compared with subjects with episodic tension-type headache in a study from the USA (16). Similarly, persons with frequent migraine worked fewer days per week than migraineurs with less frequent headache in a 3-month diary study (17). Furthermore, the number of headache days was found to be a strong predictor of unemployment rates in a 2-year follow-up study (18).
In our study, the highest proportion of long-term sick leave was found among headache sufferers with coexisting chronic MSCs and psychiatric disorders. This finding was expected because MSCs and psychiatric disorders are the two most common reasons for sick leave in Norway (19) and because chronic headache is strongly associated with musculoskeletal pain (14) as well as with anxiety and depression (15).
The strengths of this study were the large and unselected population and the use of validated headache diagnoses, but there are also limitations to be taken into account. Since our estimates were based on data from 52% of the adult population in Nord-Tr⊘ndelag, one may question to what degree the results can be generalized. The fact that neither headache, working situation, nor sick leave was the primary objective of the study makes selective participation unlikely. Individuals who responded were more likely to be women and middle aged than were non-responders and participation was lowest in the age group 20–29 years (1). A non-participation study was performed in a 2.5% random sample of the non-attendants and the main reasons for not attending in the age group 20–67 years were lack of time, having moved out of the county or having forgotten the invitation. Particular selection by health status was present only among the elderly >70 years old (11). However, a minor group of individuals aged 40–67 stated that the main reason for not attending was that they were too busy at work and, among these, sick leave behaviour could have been different. Thus, generalization of the present results should be made with some caution.
Questionnaire-based headache diagnoses are less accurate than interview-based diagnoses (13), which may introduce misclassification bias. Most likely, possible differences between migraine and non-migrainous headache sufferers are underestimated owing to the presence of migraine subjects in the non-migrainous headache group and vice versa, making the two groups seem more similar than they actually are. Misclassification may not be a big problem, however, because the prevalence of migraine in the current population is consistent with data from other population-based studies in western countries (2).
One may also question the validity of the questionnaire-based information about sickness absence. Lack of a central register in Norway with specific data on medical reasons for sick leave made it difficult to validate the self-reported information. However, the internal consistency of the positive responses to the question about sick leave was very good, since 92% of the individuals who reported sick leave due to chronic MSC in Q1 confirmed such sick leave in Q2.
The proportion of self-reported sick leave during the past year was 12% higher (56% vs. 44%) among headache sufferers compared with headache-free individuals. This percentage is similar to that found in two other Scandinavian population-based surveys in which the proportions of sick leave during the previous year due to headache were 13% and 14%, respectively (3, 5). In a population-based study from England, 15% reported sick leave from work or reduced ability to work due to headache during the last 3 months in a population-based study (6). In the present study the prevalence of short-term sick leave (<2 weeks) was 6.2% higher among headache sufferers than among headache-free individuals (35.6% vs. 29.4%). Interestingly, 6.2% of short-term absence from work was due to headache in a previous prospective study among employees in Norwegian factories (20).
Both previous and the present population-based studies dealing with the relationship between sick leave and headache are cross-sectional and based on retrospective self-reported data. Recall problems are probably not different among headache sufferers from those among headache-free individuals. Thus, the present data based on an unselected population allow us to give a rough estimate of the number of days lost from work in the preceding year because of headache. We found that a total of 42 487 (minimum 24 728) working days was lost due to headache the past year, or 1447 (minimum 842) working days per 1000 employed persons in a year. In comparison, the total number of loss of workdays per year due to headache was found to be 1090 days per 1000 persons in Denmark and 1327 days per 1000 persons in England (5, 6). The suggested 42 487 lost working days due to headache represent an approximate 0.6% of working days for all employed respondents, which is nearly identical to what has been found in England (0.5%) (6).
We estimated that migraine patients lost 4.4 days (minimum 2.6 days) per year due to headache. In accordance with our minimum estimate, on average, 2.5 days per year were lost due to migraine based on data from four different studies (9). On average, persons with non-migrainous headache lost 2.8 days (minimum 1.7 days) due to headache. Few other population-based studies have evaluated sick leave days in those with non-migrainous headache. However, based on data reported in the study from the USA, subjects with tension-type headache lost 0.9 days per year (16).
In most previous studies on headache-related sick leave, the participants were asked specifically about absence due to headache. In the present study, participants were asked about total sick leave and the proportion with sick leave due to headache has been calculated by subtracting the proportion in those with headache from the proportion in headache-free individuals. The fact that similar figures were found with both methods should corroborate the findings that approximately 12–15% of the working European population have sick leave due to headache every year.
The overall costs due to headache are not easy to estimate. In Norway sick leave costs about €4 billion per year and, based on the present data, sick leave due to headache may cost Norwegian society approximately €0.5 billion per year. Migraine, with a 1-year prevalence of 14% in the adult population, has in a recent review been estimated to cost €590 per year per patient in some western European countries (8, 21). Because indirect costs constitute approximately 90% of the total cost of migraine (9) and because sick leave represents a major factor of the indirect costs, better headache treatment increasing the working capacity will have huge economic implications.
Conclusion
Our study has demonstrated a higher prevalence of short and long-term sick leave during the last year among headache sufferers compared with headache-free individuals. Duration of sick leave was positively associated with frequency of migraine and non-migrainous headache. The impact of headache on sick leave is substantial and represents a considerable burden to society.
Acknowledgements
The Nord-Tr⊘ndelag Health Study (The HUNT study) is a collaboration between the HUNT Research Centre, Faculty of Medicine, Norwegian University of Science and Technology (NTNU), the Norwegian Institute of Public Health and Nord-Tr⊘ndelag County Council.