
Abstract
Investigations of migraine comorbidity have confirmed its association with diverse psychiatric conditions. This association appears to be strongest for major depression and anxiety disorders (particularly panic and phobia), but increased comorbidity has also been reported with substance abuse and certain mood disorders. This literature also indicates that greater psychiatric comorbidity exists for migraine sufferers with aura than without. Some support is found for the notion that psychiatric comorbidity is higher in transformed migraine than in simple migraine (particularly in the case of chronic substance abuse). However, research into the possible mechanisms underlying these associations remains limited. Studies examining the order of onset and the cross-transmission of migraine and psychiatric disorders in families have been unable to distinguish fully between causal and common aetiological models of association. The conclusions are discussed in light of both methodological and conceptual issues relevant to understanding migraine comorbidity.
Introduction
For more than a century, clinicians and researchers alike have noted the possible relationship between migraine and diverse psychological characteristics, including tendencies toward depression, perfectionism, and repressed aggression. Although most of this literature has been based on clinical observations and case studies, recent research applying more rigorous scientific methodology has confirmed several of these associations (for reviews, see 1–5). However, it remains difficult to compare across all previous investigations due to differences in nosology and case definition. In addition, previous reviews of this literature have not consistently addressed certain manifestations of migraine, such as the ‘transformed’ subtype that characterises a significant proportion of this population. The purpose of the present review is to provide a detailed summary of studies conducted since 1988 that have in general applied the International Headache Society (IHS) criteria to diagnose migraine (6), and that have examined psychiatric syndromes such as defined on axis I of the Diagnostic and Statistical Manual of Mental Disorders (DSM) (7, 8). Investigations were identified using both the Medline database and bibliographies of the published literature. The first and second sections of this review summarize the research concerning the general association between psychiatric disorders and migraine in general population and in clinic-drawn samples, respectively. The third section addresses the specific investigations that enable a comparison between the causal and common aetiological mechanisms underlying these associations.
General population studies
Since the introduction of the IHS criteria, nine studies of community-drawn samples have examined the association between migraine and psychiatric disorders. Table 1 presents the major methodological characteristics and principal findings of these studies. Table 2 presents the magnitude of association for those studies reporting their findings in terms of odds ratios. As indicated by the tables, all cross-sectional investigations of psychiatric disorder prevalence in ‘migraine’ compared with ‘non-migraine’ samples found an increased risk of anxiety disorders, particularly panic disorder (PD) and phobias. As for other anxiety syndromes, one study (9) found an association between migraine and obsessive-compulsive disorder (OCD) as well as generalized anxiety disorder (GAD), but these associations were not replicated in a subsequent investigation (10). Both of these investigations were of high methodological quality (including rigorous sampling criteria in a community setting, use of structured interviews and application of DSM–III-R diagnostic criteria). The reasons for this discrepancy therefore remain uncertain.
Population-based studies of migraine comorbidity with psychiatric disorders (IHS criteria)
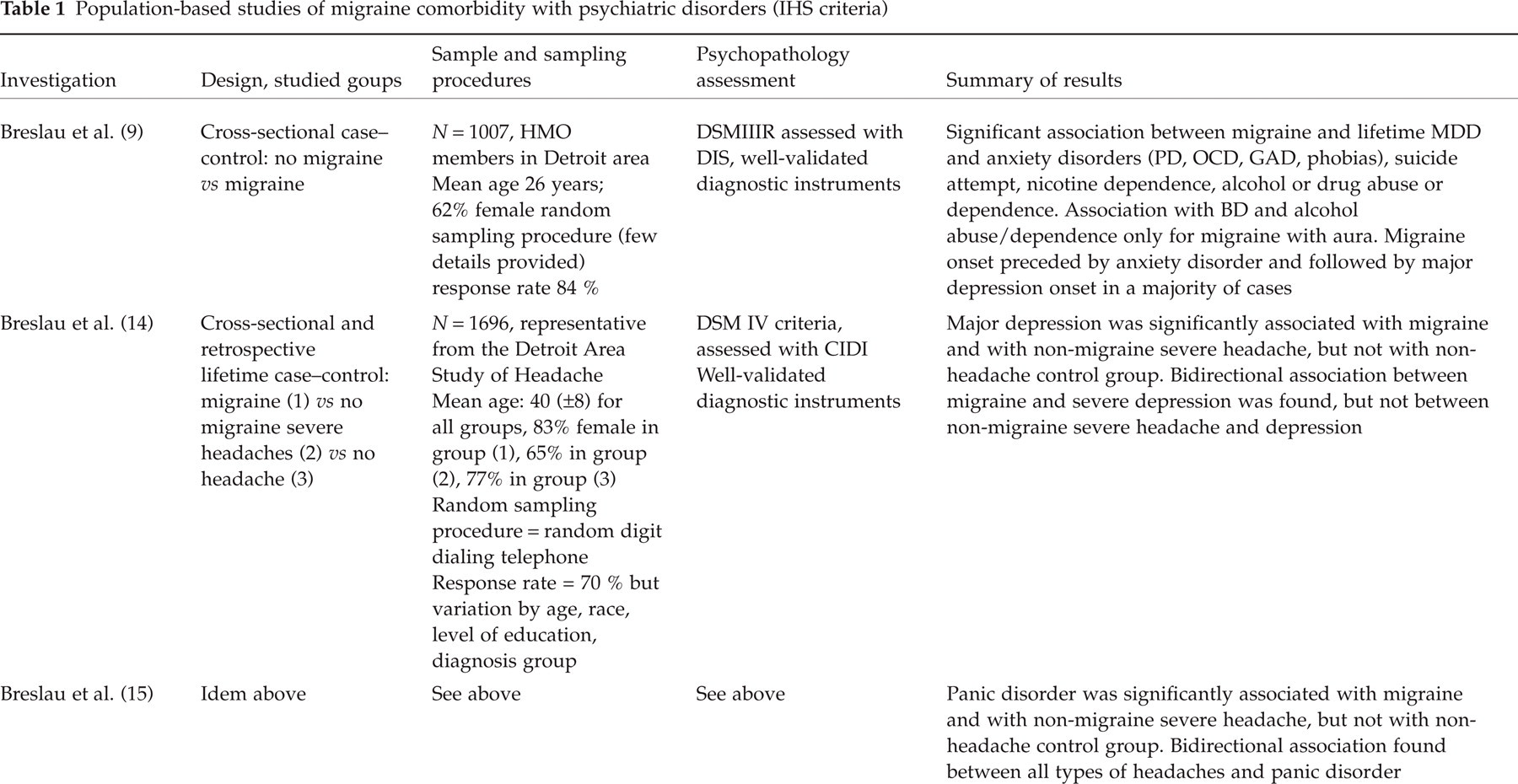



DSM, Diagnostic and statistic manual; DIS, diagnostic interview schedule; PD, panic disorder; OCD, obsessive compulsive disorder; CIDI, composite international diagnostic interview; Ph D, phobic disorder; SPIKE, structured psychopathological interview and rating of the social consequences for epidemiology; GAD, generalized anxiety disorder; HAD, hospital anxiety depression scale.
Lifetime comorbidity of psychiatric disorders and migraine from population-based studies using IHS criteria (odds ratios and 95% CI)

NS, Not significant.
Aside from one exception, previous investigations of mood disorders have been highly consistent in reporting an increased prevalence of major depressive disorder (MDD) in patients with migraine. The one discrepant study (11) was characterized by several methodological differences or limitations that may explain why no association with MDD was found. These include the fact that the sample was not representative of the general population or of clinic settings (i.e. it was comprised of a cohort of young adults selected for ‘high psychopathological risk’ defined by scores on a general symptom checklist), and the cohort studied was notably younger and had a different sex composition than the other published investigations. Moreover, the assessment of cases was based on the SPIKE, a structured diagnostic interview designed for epidemiological studies but that has not been used in other investigations of this topic. It is therefore unclear to what extent diagnoses established by the SPIKE may differ from those of more commonly used instruments. In a population of subjects aged over 65 years, Wang (12) found that the risk of current depression (based on scales designed for use in elderly subjects but inadequate for assessing diagnostic criteria) was much greater in migraine sufferers than in non-migraine patients. Finally, a recent controlled study conducted in a community setting (13) confirmed the higher risk of current depression among those suffering from migraine. A major focus of this study concerned the influence of migraine and depression on quality of life, and the findings clearly demonstrate that migraine and depression exert a significant but independent impact. Concerning other forms of mood disorder, Breslau (9) reported that migraine with aura was associated with bipolar disorder (BD). While an association between migraine and BD was not observed by Swartz (10) or Merikangas (11), these latter studies did not differentiate between migraine with and without aura. In addition, Breslau reported an association between migraine with aura and suicide attempts (9), a finding which persisted even after adjustment for major depression. This result is also consistent with other work indicating that psychiatric comorbidity may occur more frequently in migraine with aura than in migraine without aura (14).
In cross-sectional investigations, substance-related disorders have been examined in only three studies. Breslau (9) found an increase risk of alcohol and drug abuse in migraine sufferers, while Merikangas (11) and the Epidemiological Catchment Area Study (10) did not. Since substance abuse is highly comorbid with BD, it is possible that the increase of substance abuse in the Breslau study (9) could potentially be accounted for by comorbidity with BD.
With the exception of two investigations (12, 13), all previously described samples were also followed prospectively for periods ranging from 14 months to 13 years (10, 11, 14–17). In general, the prospective analyses not only confirmed many of the cross-sectional findings, but were also able to examine the risk of psychiatric disorder onset in persons already affected by migraine. For both Breslau (16) and Merikangas (18), the risk of panic disorder onset during the follow-up period was greater for people with migraine than for those without. Merikangas (18) also found that the risk of phobia onset during the follow-up period was greater for migraine sufferers but, in contrast to Breslau (16), she did not find a significant association between migraine and mood disorders (with the exception of brief recurrent depression). A possible explanation for this discrepancy is that the first evaluation of the Merikangas study took place in 1979, before the adoption of IHS criteria, and may therefore have differed in terms of case definition. In the one investigation to examine psychiatric disorders as a risk factor for the onset of migraine, Swartz (10) reported that the presence of phobic disorders at the first assessment in 1981 was predictive of the incidence of migraine at the follow-up assessment administered between 12 and 15 years later. Finally, it is important to note that the only study to compare migraine sufferers from the general population with those from treatment settings found no significant differences between the two groups, at least in terms of the severity of anxiety and depression scores (19). This finding is surprising, and may be explained by the use of the Hospital Anxiety Depression scale (HAD) which measures only general emotional distress and does not allow a diagnosis of anxiety or mood disorders.
In summary, investigations in the general population provide generally consistent support for an increased risk of depressive and anxiety disorders in persons with migraine compared with those without (and without other forms of headache). Less consistent but suggestive evidence has been reported for other forms of comorbidity (such as with bipolar disorder and substance abuse/dependence), but most forms of comorbidity appear to be increased in migraine with aura compared with migraine without aura. Methodological concerns must be carefully examined, in particular the use of rating scales that do not allow for psychiatric diagnoses. Unfortunately, most studies have focused on anxiety and major depressive disorder comorbidity, whereas there is a lack of information concerning more controversial issues including substance-related disorders, bipolar disorders, and somatoform disorders.
Investigations of clinical samples with migraine and comparisons with other types of headache
Table 3 summarizes the methodological characteristics and principal findings of studies that have been conducted in clinic-drawn samples since the introduction of the IHS criteria. In contrast to the majority of case–control investigations previously reviewed, these studies compare migraine with other forms of headache (tension headache, chronic daily headache, transformed migraine, and daily headaches with chronic substance abuse). Of the three studies to have compared patients suffering from migraine and tension headache (20–22), none reported any significant differences in terms of psychiatric comorbidity. On the other hand, the three studies which compared chronic headache and migraine patients demonstrated a higher risk of psychiatric disorders in the former (20, 23, 24). This risk seems to be particularly increased in patients suffering from transformed migraine (25). In the study by Verri (23), the authors underscore the high frequency of comorbidity between anxiety and depression in all groups of patients. However, mood disorders were more frequent in patients who had had chronic headache for more than 5 years (as opposed to shorter durations). It is also notable that this study compared chronic headache patients with low back pain patients. Interestingly, the headache patients suffered more frequently from all psychiatric disorders, with the exception of somatoform conditions. This finding strengthens the hypothesis that the excess of psychiatric morbidity found in headache patients is specific to that population and is not simply the result of the presence of chronic pain. However, as this study by Verri included both migraine patients who suffered from tension headache between episodes and patients suffering from chronic tension headache, the sample is less homogeneous and the findings should be interpreted accordingly.
Clinic-based studies of migraine comorbidity with psychiatric disorders: comparison among headache types (IHS criteria)

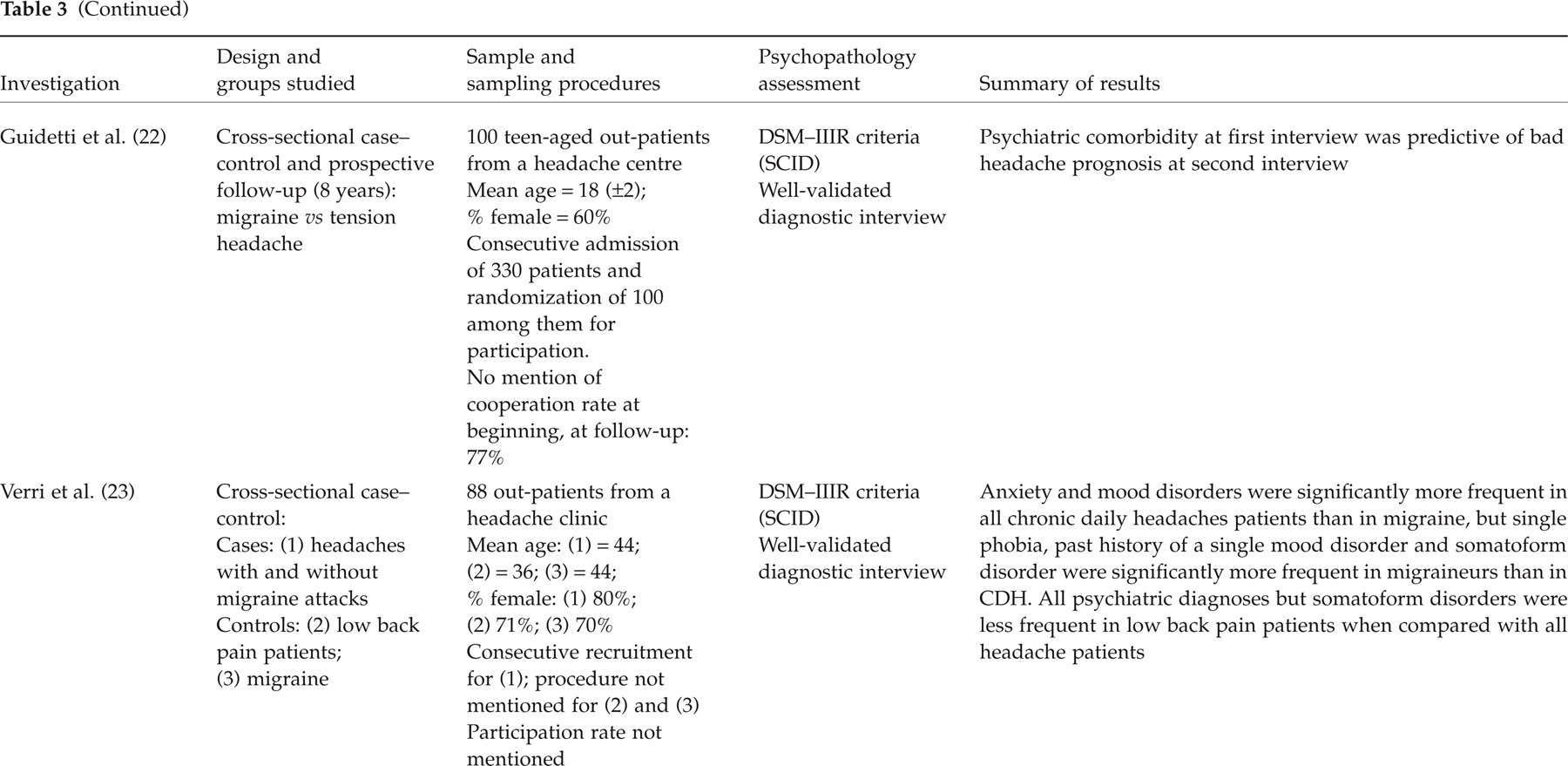

CDH, Chronic daily headache; SADS, schedule for affective disorders and schizophrenia; DSM, diagnostic and statistical manual; FH RDC, family history-resaarch diagnostic criteria; SCID, structure clinical interview for DSM–IIIR; HAMD, Hamilton depression scale; HAMA, Hamilton anxiety scale; MINI, mini international neuro-psychiatric interview.
Two investigations presented in Table 3 compared migraine sufferers with daily headache patients with chronic substance abuse (20, 24). The study by Mitsikoskas (20) found that major depression was twice as frequent in patients abusing analgesics. Radat (24) demonstrated an excess risk of suffering from major depression, panic disorder and social phobia in those suffering from transformed migraine with chronic substance use, even after adjustment according to age and gender. Thus, the group differences were attributable neither to the greater age of those suffering from transformed migraine, nor to the higher number of women in the sample. Unfortunately, these studies did not assess the frequency with which a DSM psychiatric diagnosis of substance abuse/dependence could be applied to patients using analgesics containing psychoactive agents. Finally, Juang (25) compared patients suffering from transformed migraine with those suffering from chronic tension headache. He demonstrated a higher frequency of anxiety in transformed migraine patients after adjustment for age and gender. Here again, however, the role of substance abuse or dependence criteria was not examined.
In summary, no difference has been demonstrated between migraine patients and tension headache sufferers in terms of the prevalence of psychiatric comorbidity. On the other hand, there is a consensus that those with migraine are at reduced risk of suffering from anxiety and mood disorders compared with patients suffering from chronic headache. In addition, studies comparing migraine patients with headache patients with chronic substance use have shown that anxiety and mood disorders are more frequent in the latter, and that this difference is particularly true for patients with transformed migraine compared with simple migraine or chronic tension headache.
Investigations of comorbidity mechanisms
An overview of the research looking into the comorbidity between migraine and psychiatric disorders has also provided some insight into the potential causes of these associations. Three basic mechanisms of comorbidity have been considered in this literature: (i) that psychiatric disorders are a causal factor in the development of migraine; (ii) that migraine is a causal factor in the development of psychiatric conditions (e.g. repeated and intense pain leads to anticipatory anxiety, perceived loss of control, and other behavioural or cognitive risk factors for psychiatric syndromes); and (iii) that a common shared aetiological factor may explain the co-occurrence of both syndromes without a causal association between them (e.g. a common genetic factor concerning neurotransmitter or other biological abnormalities) (26). These mechanisms have been compared most frequently through longitudinal studies of the order of onset of each condition, the changes in severity of one disorder if another is present, and the co-transmission of these disorders within families. Although no study to date has investigated the correlation between the severity of migraines and the severity of anxiety or mood disorders, some limited information exists concerning the relationship between the frequency of psychiatric comorbidity and the severity of migraine. Mitsikoskas (20) demonstrated that the severity of headache was not associated with depression or anxiety, but that there was a significant association when considering the frequency and duration of the attacks. The follow-up of these patients over 6 months similarly demonstrated a correlation between the evolution of headaches and anxiety or depression. Unfortunately, however, both cross-sectional and prospective analyses combined all types of headache and were not differentiated by diagnostic group. Concerning the order of onset of specific disorders, Merikangas (11, 27) found for most patients that the age of onset of anxiety preceded that of migraine, which in turn preceded that of depression. Merikangas also demonstrated that the ages of onset of each disorder were significantly correlated. In the retrospective study by Breslau (16), anxiety was also shown to precede migraine in most patients, which in turn preceded depression similarly to what Merikangas had observed. Swartz (10) studied psychiatric disorders as possible risk factors for the onset of migraine during a 13-year prospective follow-up and found that only a history of phobic disorder was predictive of the onset of migraine. The fact that no predictive role was found for mood disorders would therefore support other studies (11, 16, 27) in arguing against the hypothesis that they are aetiologically tied to migraine onset. Moreover, the 14-month prospective study by Breslau et al. (16) demonstrated that the risk of onset of a depressive disorder or panic disorder during the follow-up period was slightly greater in people with a past history of migraine compared with individuals with active migraine (15.4%vs 13%). These findings seem to refute the idea that a salient unidirectional pattern of association characterizes these forms of comorbidity. In the same way, Breslau and colleagues (14, 28) recently performed a Cox proportional hazard model and found no preferential order of onset for depression or panic relative to migraine. It is nonetheless notable that Breslau did find a preferential order of onset of major depressive episodes in relation to severe non-migraine headache. Finally, Guidetti (22) performed an 8-year follow-up of a cohort of children suffering from migraine and tension headache. Anxiety was found to be a predictor of the persistence of headache in both migraine and tension headache patients. However, this latter finding cannot be interpreted as specific to anxiety, as it is unclear if childhood anxiety might constitute a precursor to adult mood disorder.
In summary, these investigations concur in indicating that only phobic disorders appear to predict the onset of migraine, and that a bidirectional chronology exists between migraine and depression or panic disorder. The lack of clear predictive relationships between these syndromes raises the possibility either of a symmetrical causal link (each disorder being a risk factor of the other), or of a common genetic or environmental risk factor. In one of the first investigations comparing these modes of association, Merikangas (29) examined 133 depressed subjects, 82 normal controls, and the first-degree relatives of both groups enrolled in the Yale University Family Genetic Studies of Depressive Disorders. This study was not originally designed to address migraine and, as a result, IHS criteria were not applied. By using bi-variate polygenic threshold analysis, Merikangas found a cross-transmission that favoured an environmental factor over a genetic one, but the results were not significant. In any case, a subsequent investigation by the Yale University Family Genetic Study of Migraine (Table 3) did apply IHS criteria, which suggested that no cross-transmission between migraine and anxiety or depressive disorders in families existed (11). Some evidence was nonetheless found for an increased risk of migraine among relatives of bipolar patients compared with relatives of non-bipolar patients, but the risk of bipolar disorder was not increased in the relatives of non-bipolar migraine sufferers (30). These findings suggest a non-symmetrical cross-transmission between bipolar disorder and migraine, but no conclusive support was found for common aetiological factors in the transmission of the two disorders. In summary, therefore, the reviewed investigations do not favour a common genetic connection between MDD and migraine, and the nature of their association remains debatable for bipolar disorder.
Conclusion
A review of investigations that have applied IHS criteria leads to a number of conclusions about the comorbidity of migraine and psychiatric disorders. The consensus is that migraine sufferers are at higher risk of depression and certain forms of anxiety (in particular panic and phobic disorders). These findings appear particularly salient for migraine with aura as opposed to migraine without aura. Suggestive but inconclusive evidence also exists that indicates a potential association between migraine and bipolar disorder or substance abuse syndromes. Most of these studies were not originally designed to explore the comorbidity between migraine and psychiatric disorders, and are extensions of specific psychiatric research programmes. When comparing headache subtypes, most forms of psychiatric comorbidity appear to be equally frequent in migraine and tension headache. On the other hand, psychiatric comorbidity is greater for people suffering from chronic headache and medication overuse headache. In this latter clinical group, few comparisons have been made between different types of headache with regard to DSM substance-related disorders, and the lack of official recognition by the IHS first edition of certain forms of migraine, such as the transformed subtype, may have hindered work on this topic. The question of comorbidity between migraine and substance-related disorders should therefore remain a priority for future research. If such comorbidity is confirmed, one might suppose the existence of a predisposition for medication abuse among migraine sufferers.
Aside from the generally consistent literature concerning specific forms of psychiatric comorbidity in migraine, the review indicates that the mechanisms underlying these associations remain poorly understood. Although previous studies suggest that there is a correlation between frequency of headache and frequency of anxiety or depressive disorders, no clear correlation has been found between the severity of migraine and anxious or depressive symptoms. In addition, the possibility of a preferential order of onset of psychiatric disorders in relation to migraine appears unlikely, with the exception of some forms of anxiety disorder. Our current inability to distinguish between causal and common aetiological models for these associated syndromes is further explained by the relative dearth of family studies on this topic. Future research concerning the magnitude, specificity, or causes of these forms of comorbidity would benefit from applying careful distinctions of disorder subtypes as well as consideration of temporal issues in the development of study designs. Others issues concerning comorbidity in clinical practice also merit further attention, such as how comorbidity may affect migraine prognosis, lead to chronic substance use, or how modifications in treatment strategies may address comorbid conditions.
Finally, the clinical implications of psychiatric comorbidity among migraine sufferers are numerous and underscore the need for vigilance when managing migraine, particularly with regard to mood disorders and eventual addictive behaviour. Such information may explain which patients are most likely to experience an evolution of migraine into more problematic syndromes (i.e. transformed migraine with chronic substance use), and provide clearer indications for both pharmacological and psychological treatment. For example, amitriptyline has often been prescribed in the case of migraine and depression comorbidity. Considering that amitriptyline must be used in higher doses (125–150 mg p.d.) to treat depression than to prevent migraine (31), the frequent adverse effects at such dosages have led to its discontinuation as a treatment for this form of comorbidity. Although Selective Serotonin Reuptake Inhibitors (SSRIs) are a first-line treatment of depression and have an efficacy equivalent to tricyclic antidepressants (32), the evidence for SSRI efficacy in migraine prophylaxis is controversial (33, 34). It has therefore been proposed that a tricyclic antidepressant be combined with a SSRI for comorbid migraine and depression (35). Similarly, the efficacy of divalproex is established in the prophylactic treatment of migraine (36) as well as for bipolar disorders (37), and therefore may be particularly indicated for patients with this form of comorbidity (1). Concerning psychological interventions, the efficacy of relaxation, biofeedback, and cognitive-behavioural therapy (CBT) have all been demonstrated in the prophylaxis of migraine (38, 39). For anxiety disorder comborbidity, relaxation should be prioritized, especially with patients for whom stress is clearly identified as a precipitating factor of migraine attacks. By contrast, depression associated with migraine does not appear to predict improved efficacy of relaxation (40). These therapeutic techniques also rely on the education of migraine patients, as a collaborative alliance between doctors and patients is essential to migraine treatment. CBT may be particularly useful in attaining this goal and is indicated for patients with problematic use of acute migraine medications (thus being at risk for medication overuse headaches). In the light of these findings and clinical implications, the collaboration between psychiatrists, psychologists and neurologists in headache clinics is of clear importance, especially as psychiatric disorder comorbidity has a direct impact on therapeutic decisions.