
Abstract
Background
Occipital neuralgia (ON) describes severe, paroxysmal occipital nerve pain. This review synthesizes data on the epidemiology and clinical features of ON.
Methods
A systematic search of PubMed and Embase databases was conducted from 1988 to 2024. Two investigators independently screened titles, abstracts and full-text articles, and conducted a risk of bias assessment. Meta-analyses were performed using a random-effects model, and between-study heterogeneity was assessed using the I² statistic.
Results
Fifteen clinic-based studies, comprising 579 patients with ON, were eligible. No population-based studies were identified. Of these, three clinic-based studies examined the relative frequency of ON among adults evaluated for headache or facial pain, with reported rates ranging from 0.6 to 24.4%. Pooled estimates revealed that ON presents in the fifth decade of life and afflicts females (73%). Common clinical features were unilateral pain (81%), a stabbing quality (59%) and severe intensity (54%). Pain affected the greater occipital nerve (98%) with accompanying hypoesthesia (73%). A history of co-existing migraine was common (46%) and a proportion had a history of neck trauma (30%). The between-study heterogeneity was considerable for most clinical features assessed.
Conclusions
ON shows female predominance and links with migraine and neck trauma. Identified features can aid diagnosis and management, but high heterogeneity calls for population-based research to clarify the epidemiology of ON.
This is a visual representation of the abstract.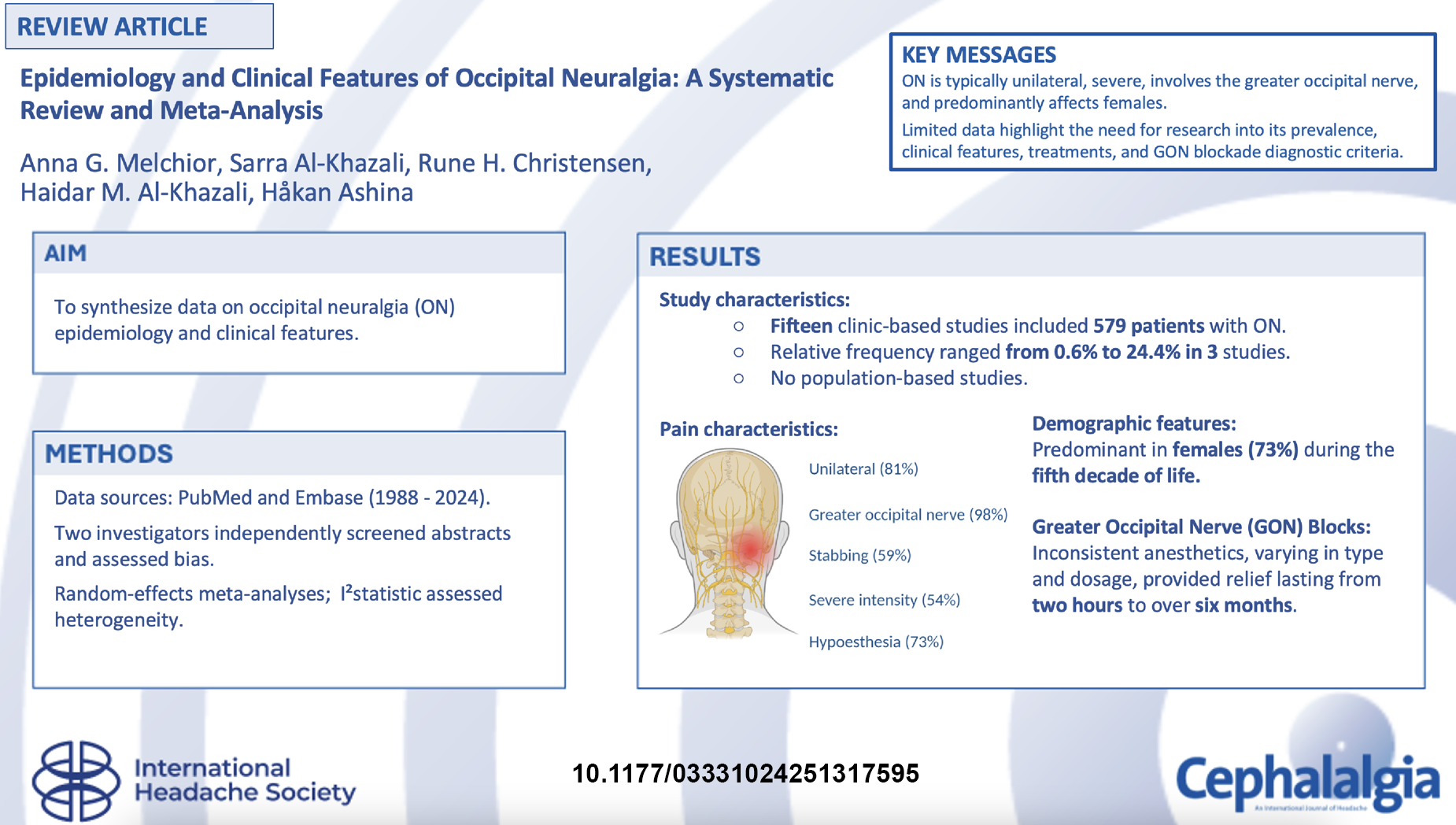
Keywords
Introduction
Occipital neuralgia (ON) is a disabling neurologic disorder characterized by severe, paroxysmal, stabbing pain originating from the occipital region. 1 This disorder is considered to be caused by irritation or compression of the greater, lesser or third occipital nerves. 1 Despite its disabling nature, the prevalence of ON and its clinical features remain inadequately quantified in the literature. 2 A better clinical characterization of ON is thus essential to avoid diagnostic delay and suboptimal care.
ON was first described in 1821 3 but remains an unfamiliar disorder for most healthcare professionals, including primary care practitioners. 4 This might be attributed to uncertainties regarding its epidemiologic patterns and typical clinical presentation. Current observational studies often differ in terms of design, subject selection and assessment methods, leading to incongruent results. A systematic review and meta-analysis of these studies can synthesize the available evidence, providing comprehensive estimates of ON prevalence and its individual clinical features.
This systematic review aims to analyze observational studies reporting on the prevalence and relative frequency of ON and its individual clinical features. Through pooling data from available population-based or clinic-based studies, we seek to clarify the epidemiologic patterns of ON, map common clinical features and explore potential factors influencing the identified estimates.
Methods
Classification
ON is classified as a type of facial pain, defined as a neuralgia without distinguishing between idiopathic, classical or secondary etiologies. This is unlike other neuralgias such as trigeminal neuralgia or glossopharyngeal neuralgia, where “classical” indicates vascular compression observed in imaging or surgery. 1 In the International Classification of Headache Disorders, 1st edition (ICHD-1), ON was characterized by stabbing pain in the occipital nerve distribution, which could be relieved by local anesthetic blocks 5 (Table 1). ICHD-2 maintained this classification but placed increased emphasis on diagnostic blocks. 6 However, both editions did not describe pain intensity or recurrence.5,6 In the ICHD-3β, criteria for pain intensity, recurrence and dysesthesia/allodynia from scalp or hair were included. 7 These criteria are also listed in the latest ICHD-3, showing minimal evolution in the diagnostic criteria for ON. 1 Notably, all ICHD editions highlight the importance of diagnostic blocks but fail to specify dosage, anesthetic type or injection site.1,5–7
Diagnostic criteria for occipital neuralgia according to different editions of the international classification of headache disorders and the international association for the study of pain.

ICHD = International Classification of Headache Disorders.
Terminology
To ensure clarity and precision in our reporting, we employ specific terminology to accurately describe the nature and source of the data analyzed. For observational data from population-based studies, we use the term “prevalence” to describe the proportion of cases with ON in the adult general population. In clinic-based observational studies, we use the term “relative frequency” to indicate the proportion of adult patients with ON among those evaluated for headache or facial pain. For the proportion of specific clinical features among patients with ON, we use the term “relative frequency”. The proportions are reported as percentages.
Search strategy
This study was pre-registered with PROSPERO (identifier: CRD42024539063) and conducted in accordance with the reporting guidelines for Meta-Analyses of Observational Studies in Epidemiology (MOOSE). 8 PubMed and Embase were searched from 1 January 1988 to 1 May 2024 for observational studies reporting data on adults with ON. The full search strategy is detailed in the supplemental material (Table S1). No language restrictions were applied to minimize potential publication bias. Reference lists of the initially identified articles were also manually searched for additional eligible studies.
Selection criteria
Studies were considered eligible if they included observational data on the prevalence of ON or its clinical features in the adult general population. Alternatively, studies were included if they reported observational data on the relative frequency of ON or relative frequency of its clinical features in adult patients evaluated for headache or facial pain in a clinical setting.1,5–7 The diagnosis of ON had to be made in accordance with any edition of the ICHD (Table 1). The full list of inclusion and exclusion criteria is detailed in the supplemental material (Table S2).
Study selection and data extraction
Two investigators (AGM and SAK) independently conducted the risk of bias assessment for studies on the prevalence in population-based studies and relative frequency in clinical samples of adult patients with headache or facial pain. A pre-designed extraction sheet was then used by the two investigators to extract data independently. Any disagreements were resolved by consulting a third investigator (RHC). The supplements provide a full overview of the data items recorded for each study deemed eligible for inclusion (see supplementary material, Table S3).
Risk of bias assessment
The Joanna Briggs Institute Critical Appraisal Instrument for Studies Reporting Prevalence Data was used to evaluate the risk of bias. 9 Two investigators (AGM and SAK) independently carried out the risk of bias assessment. Risk of bias assessment was only performed for the primary outcome of prevalence or relative frequency of ON. In case of disagreement, a third investigator (RHC) was consulted. The nine-item instrument has a range from 0 to 100%, with higher scores indicating a lower risk of study bias (see supplemental material, Table S4).9,10 Studies were then categorized as high risk (≤49%), moderate risk (50–69%) or low risk (≥70%). 9
Statistical analysis
Eligible studies were classified as either population-based or clinic-based, and data were analyzed separately for each category. The primary outcomes included: (I) the prevalence of ON in adult population-based studies and (II) the relative frequency of ON in adults evaluated for headache or facial pain in clinic-based studies. The secondary outcomes included the relative frequency of individual clinical features in adults with ON from both population-based and clinic-based samples, as well as the pooled mean of continuous clinical features such as sex, age of onset, pain intensity and quality.
A random-effects meta-analysis was performed for each outcome provided that there were data from at least two studies, each with a minimum of five participants, resulting in a total sample size of at least 10 participants. The random-effects meta-analysis accounted for between-study heterogeneity, and the inverse variance method on logit-transformed data was used to calculate pooled estimates, which were reported with 95% confidence intervals (CIs). Between-study heterogeneity was assessed using the I² statistic, with values of 75% or higher indicating considerable heterogeneity. 11
In meta-analyses with 10 or more studies, we explored between-study heterogeneity using random-effects meta-regression. If necessary, we performed a sensitivity analysis by excluding one study at a time to evaluate the influence of each individual study on the overall results. All analyses were performed with R, version 4.1.0 (R Group for Statistical Computing, Vienna. Austria), using the “meta” (https://CRAN.R-project.org/package=meta) and “metafor” (https://CRAN.R-project.org/package=metafor) packages.
Results
The database search identified 1577 records (Figure 1). Of these, 801 were deemed irrelevant and 454 were duplicates. Thus, 322 articles were screened by title and abstract, of which 31 underwent a full-text review. During title and abstract screening, an additional six studies were identified but were excluded because full-text access was unavailable. Attempts were made to contact the corresponding authors for three of these studies, whereas no contact information could be found for the remaining three. Ultimately, 15 clinic-based studies met the eligibility criteria and were included in the qualitative and quantitative analyses. 12–26 The literature search did not identify any population-based studies investigating the prevalence or clinical features of ON in accordance with ICHD criteria. Two studies were written in Spanish,17,26 and data extraction was supported by one investigator (RHC) proficient in the language.

PRISMA flow chart.
Among the 15 included studies, three reported on the relative frequency of ON in adults evaluated for headache or facial pain in clinical settings.17,21,24 Furthermore, all studies provided relative frequencies of individual clinical features of ON (Table 2).12–26 Eight of the 15 studies recorded data retrospectively,12,13,15,17,21,22,25,26 and the remaining seven studies recorded data prospectively.14,16,18–20,23,24 All included studies applied ICHD criteria when diagnosing ON.12–26 Specifically, eight studies reported using the ICHD-2 criteria,13,14,16,17,20,22,23,26 two studies used a combination of ICHD-2 and ICHD-3β criteria,19,21 two studies used only the ICHD-3β criteria,12,18 two studies used the ICHD-3 criteria,15,24 and one used the IHCHD-1 criteria.25
Clinic-based studies reporting the relative frequency of individual clinical features in occipital neuralgia.
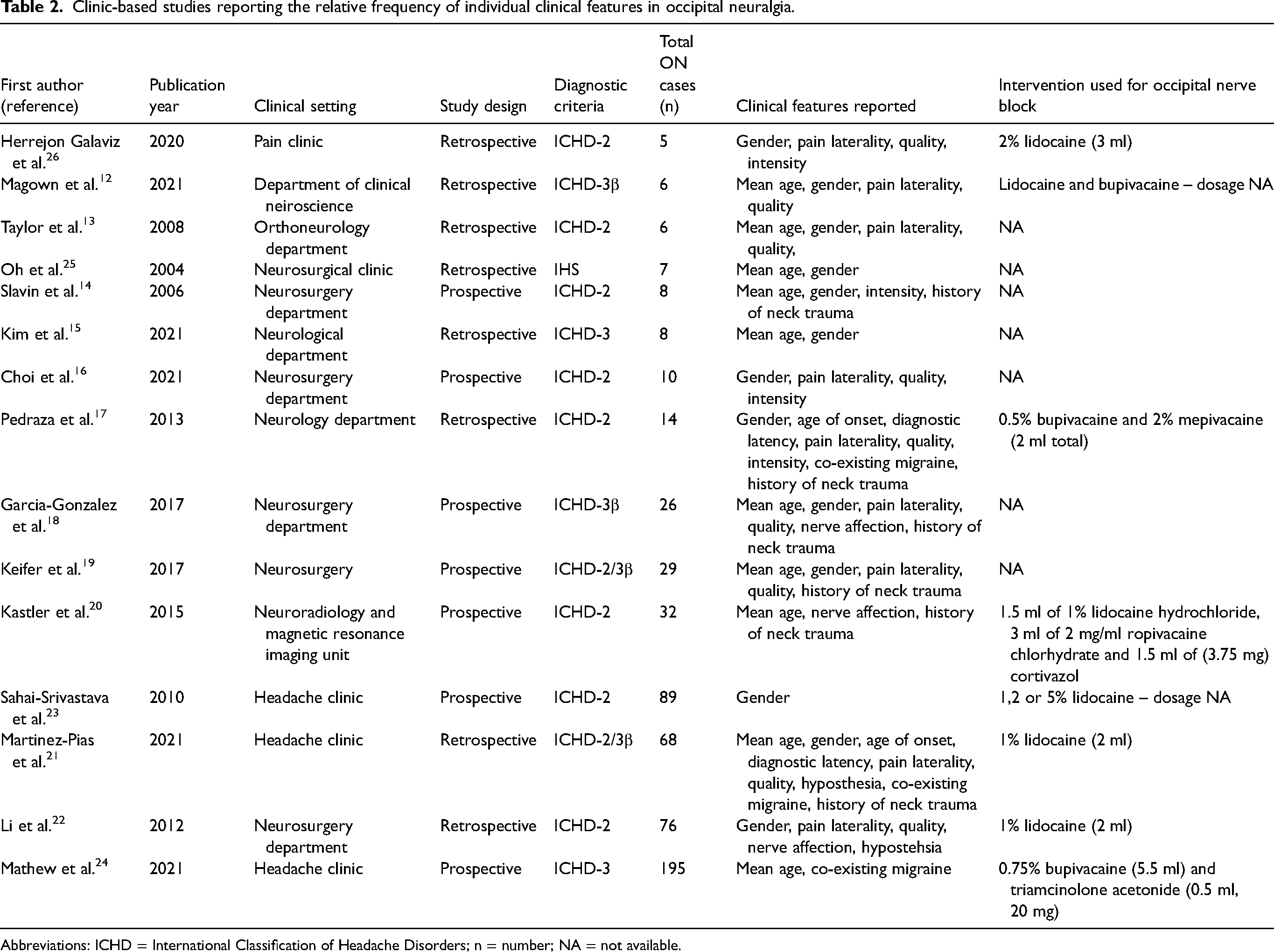
Abbreviations: ICHD = International Classification of Headache Disorders; n = number; NA = not available.
Six studies were conducted in neurosurgery departments,14,16,18,19,22,25 three in headache clinics,21,23,24 two in neurology departments,15,17 one in a pain clinic, 26 one in an ortho-neurology department 13 and one in a neuroradiology department, 20 and the last study was conducted in a department of clinical neuroscience. 12
Six studies examined the use of pharmacological treatments. Non-steroidal anti-inflammatory drugs19,26 was the most commonly reported, followed by paracetamol,19,26 benzodiazepines,19,21 amitriptyline,17,21 gabapentin17,21 and onabotulinumtoxinA.14,15,19
The use of greater occipital nerve (GON) blocks was not reported in four studies.13,15,18,19 The remaining eleven studies provided information on the efficacy of the GON block, with results varying considerably.12,14,16,17,20–26 Notably, Galaviz et al. 26 reported that a patient experienced pain relief within two hours of the block. The longest duration of pain relief was observed by Martinéz-Pías et al., 21 who noted improvements lasting up to six months or more. The most frequently used local anesthetic was 1% lidocaine, typically administered in a 2-ml dose.21,22 In addition, Mathew et al. 24 reported using the highest amount at 6 ml, consisting of 5.5 ml of 0.75% bupivacaine and 0.5 ml of triamcinolone acetonide (20 mg).
Relative frequency of ON in adult patients with headache or facial pain
Three clinic-based studies, comprising a total of 277 patients, reported on the relative frequency of ON among adults evaluated for headache or facial pain in a tertiary care setting (Table 3). The pooled relative frequency of ON was found to be 2.83% (95% CI = 0.21–28.6%; I² = 99.7%) (Figure 2).17,21,24 Given the considerable heterogeneity observed (I² = 99.7%), the studies were deemed incomparable. A visual inspection revealed that two of the three included studies reported a pooled relative frequency of ON below 2%, whereas the remaining study by Mathew et al. 24 reported a relative frequency of approximately 24%. Furthermore, all three studies failed to report the participation (response) rate among patients.17,21,24 Even after excluding Mathew et al. 24 in a sensitivity analysis (Figure 3), the heterogeneity remained high (I² = 83.7%).

Relative frequency of occipital neuralgia in adults evaluated for headache or facial pain in clinical settings. CI = confidence interval; ON = occipital neuralgia.

Sensitivity analysis of occipital neuralgia in adults evaluated for headache or facial pain in clinical settings. CI = confidence interval; ON = occipital neuralgia.
Clinic-based studies on the relative frequency of occipital neuralgia.
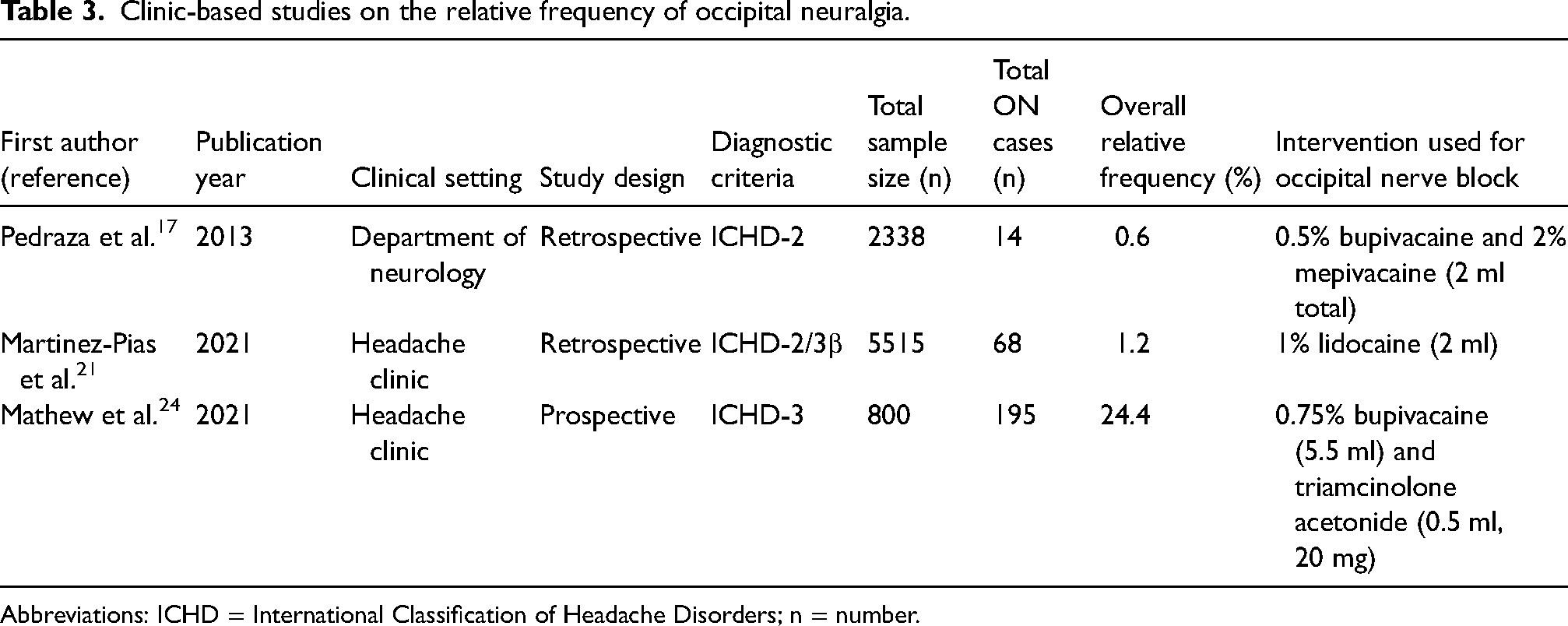
Abbreviations: ICHD = International Classification of Headache Disorders; n = number.
Mathew et al. 24 conducted a retrospective study investigating the relative frequency of ON within a headache clinic from 2010 to 2015. The authors collected data on demographics, diagnoses and the presence of an occipital nerve irritation sign (Tinel's sign). Greater and lesser occipital nerve blocks were performed to confirm the diagnosis of ON according to ICHD-3 diagnostic criteria. All physical examinations and nerve blocks were conducted by a board-certified headache specialist. The procedure involved using 5.5 ml of 0.75% bupivacaine and 0.5 m; of triamcinolone acetonide (20 mg) per side for both the greater and lesser occipital nerves. However, the criteria for defining a positive response to the blockade were not specified. The authors found that ON was present in 24.4% (195 out of 800) of patients referred with headache as the primary complaint. Among these, only 15.5% had ON without any comorbid headache disorders. However, the study did not report the participation (response) rate, which refers to the proportion of individuals who were invited to participate in the study and actually agreed to do so.
Martínez-Pias et al. 21 conducted a retrospective study aimed at illustrating the main characteristics of individuals with ON diagnosed in a headache clinic from 2008 to 2018 using ICHD-2 and 3β criteria. A detailed medical history was obtained from each patient, including the diagnosis of other co-existing headache disorders. If a patient presented with another headache disorder, its characteristics were differentiated from those of ON. However, the study did not specify the type of personnel who carried out these assessments. Magnetic resonance imaging was performed to rule out other potential causes. To confirm the diagnosis, 2 ml of 1% lidocaine was injected into the territory corresponding to the greater or lesser occipital nerve, depending on tenderness. A positive response was defined as complete relief of pain for at least 24 hours. The authors found that ON was present in 1.2% (68 out of 5515) of patients referred with headache. The study failed to report the participation (response) rate among patients.
Pedraza et al. 17 conducted a prospective study over a five-year and three-month period, including patients diagnosed with ON according to ICHD-2 criteria. One neurologist was responsible for patient inclusion. Data collection encompassed demographics, headache characteristics and neurological examinations. Nerve blocks were administered using a 1:1 mixture of 0.5% bupivacaine and 2% mepivacaine, with 2 ml given based on pain patterns and patient preference. The response to the anesthetic block and its duration were evaluated, although the specific duration and magnitude of the response were not detailed. The authors found that ON was present in 0.6% (14 out of 2338) of patients referred with headache. The study did not report the participation (response) rate among patients.
Clinical features of ON in adult patients with headache or facial pain
Fifteen clinic-based studies, comprising a total of 579 patients, provided data on the relative frequency of individual clinical features of ON eligible for meta-analysis12–26 (Table 4). The pooled mean age was 50 years (95% CI = 45–54 years; I² = 86%),12–15,18–21,24,25 and 73% (95% CI = 57–84%; I² = 79%)12–19,21–23,25,26 were females. The pooled mean age of disease onset was 56 years (95% CI = 53–59 years; I² = 0.0%),17,21 with a mean duration between the onset of symptoms and formal diagnosis of 29 months (95% CI = 16–41 months; I² = 0.0%).17,21 Most patients experienced unilateral pain (81%; 95% CI = 55–94%; I² = 85%).12,13,16–19,21,22,26 The clinical presentation was characterized by stabbing pain (59%; 95% CI = 16–92%; I² = 86%)14,16,17,19,21,26 and severe intensity (54%; 95% CI = 20–85%; I² = 69%)14,16,17,26 affecting the greater occipital nerve (98%; 95% CI = 94–100%; I² = 0.0%).18,20,22 Only one study provided data on the lesser occipital nerve 18 and no studies provided data on the third occipital nerve. Because meta-analyses require data from at least two studies, we were unable to include these nerves in our analysis as a result of insufficient data. Lastly, the clinical presentation was also characterized by hypoesthesia was present in 73% of patients (95% CI = 0.13–100%; I² = 96%).21,22
Demographic and clinical characteristics of patients with occipital neuralgia.
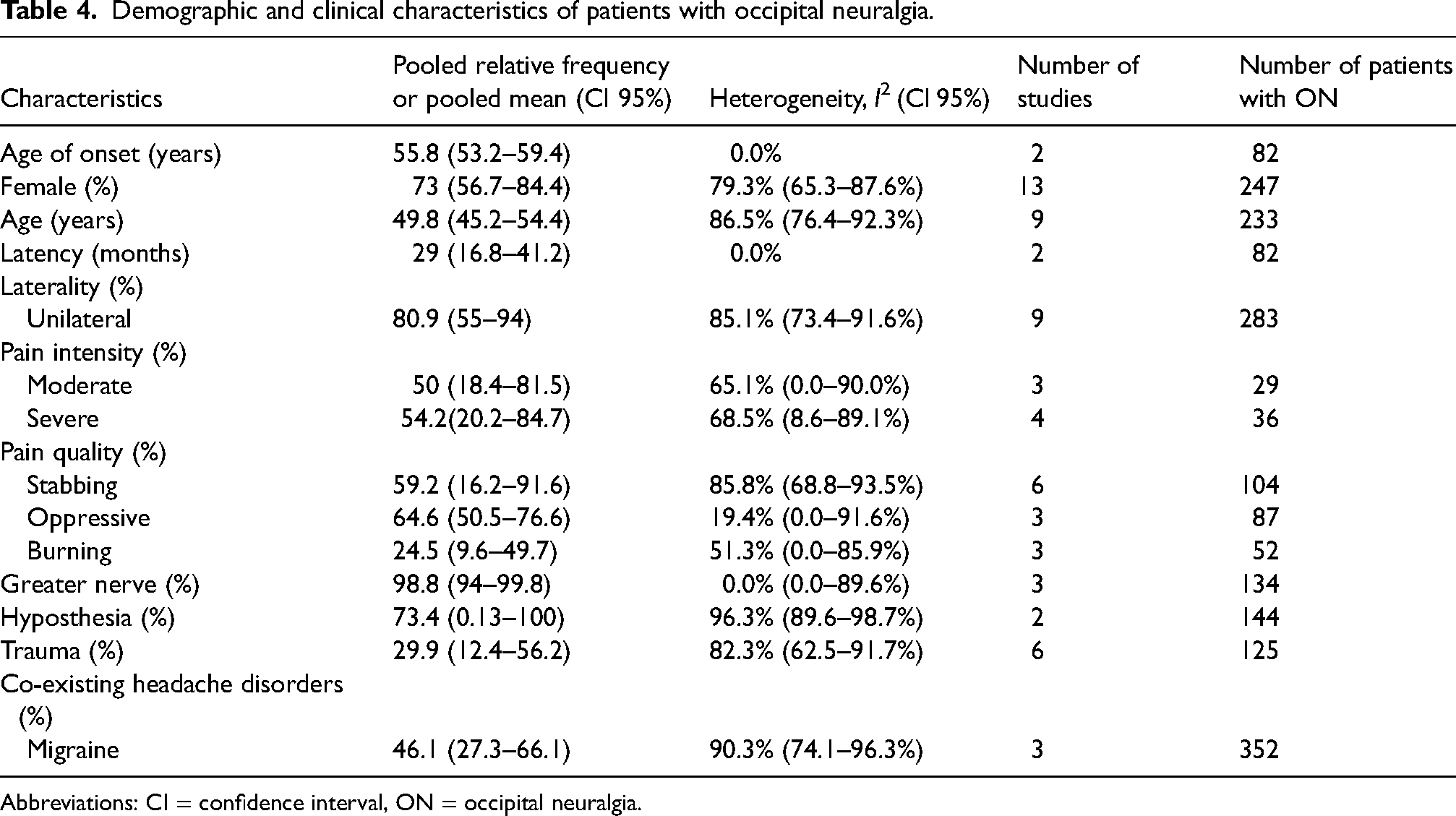
Abbreviations: CI = confidence interval, ON = occipital neuralgia.
Moreover, four clinic-based studies provided data on comorbid headache disorders among patients with ON, including migraine, cluster headache, tension-type headache and primary stabbing headache.20,21 However, only data on comorbid migraine were available in two or more studies.17,21,24 The pooled relative frequency of co-existing migraine was 46% in patients with ON (95% CI = 27–66%; I² = 90%).17,21,24 A history of neck trauma was reported in 30% (95% CI = 12–56%; I² = 82%),14,17–21 which, in some studies, was reported as whiplash injury, although most did not specify the cause of neck trauma. In total, six studies reported on neck trauma, but the reports were scarce.
Meta-regression of clinical features of ON
Meta-regression was performed to investigate explanatory variables for the high heterogeneity observed in the pooled estimates for female sex (I² = 79%), comprising data from 10 or more studies. The analysis examined clinic type (neurosurgical vs. non-surgical) and the use of ICHD-3 criteria as potential sources of variation. However, neither the type of clinic (p = 0.4 for female sex) nor the use of ICHD-3 criteria (p = 0.39 for female sex) explained the observed heterogeneity.
Risk of bias
We assessed the risk of bias in the three clinic-based studies that reported on the relative frequency of ON in adults evaluated for headache or facial pain. All three studies were found to have a moderate risk of bias. They failed to include an appropriate sample size and did not report on recruitment and response rates17,21,24 . The detailed risk of bias assessment is summarized in the supplemental material (Table S5).
Discussion
This systematic review and meta-analysis are the first to reveal substantial variation in the reported relative frequencies of ON in adult patients evaluated for headache or facial pain in clinical settings. The pooled estimate suggests a relative frequency of 2.83% (I² = 99.7%), reflecting considerable heterogeneity that challenges the robustness of conclusions. Although the use of a random-effects meta-analysis with the inverse variance method on logit-transformed data is methodologically sound for addressing heterogeneity, the reliability of these estimates is heavily influenced by the quality, sample size and number of included studies. This considerable heterogeneity constrains the generalizability of our findings.
Our inclusion criteria adhered to the ICHD, the gold standard for diagnosing ON, ensuring specificity and minimizing bias. This approach upheld the reliability of our findings compared to more liberal criteria, which could compromise study integrity.
Clinical features
Adult patients with ON were predominantly female, accounting for 73% of the cases. The mean age of onset was 56 years, with a diagnostic delay of approximately 29 months. Among the clinical features, the pain was mostly severe (54%), of a stabbing quality (59%) and unilateral (81%), almost exclusively affecting the greater occipital nerve (98%). Further research is also imperative to determine the extent of involvement of the lesser occipital and third occipital nerves in patients with ON. Our systematic literature review identified only one clinic-based study that provided specific data on the lesser occipital nerve and no article on the third nerve. 18 This points to a substantial need for studies that might reveal insights important for refining diagnostic approaches for ON.
Hypoesthesia was also frequent, occurring in 73% of patients. Interestingly, almost half of the patients (46%) had co-existing migraine, and 30% reported a prior neck trauma, although the specific nature of the trauma (e.g. whiplash) was often unclear.
The meta-analyses should be interpreted with caution as a result of substantial heterogeneity and large confidence intervals. Meta-regression analysis revealed no significant influence of neurosurgical clinics or the use of ICHD-3 criteria on the observed heterogeneity for unilateral pain and female sex. The source of this variability remains unclear and necessitates further investigation.
Methodological considerations in clinic-based studies reporting on the relative frequency of ON
Our primary outcomes focused on the prevalence and relative frequency of ON. Studies investigating the relative frequency of ON in headache clinics reported a wide range of relative frequency: 24.4, 1.2 and 0.6%. Mathew et al. 24 was a clear outlier with a considerably higher relative frequency. Although we found no overt differences in the studies’ approaches, several methodological factors might contribute to this variability. First, the emphasis on the occipital Tinel's sign during physical examination varied. Mathew et al. 24 systematically evaluated the occipital Tinel's sign for all participants, whereas the other studies did not report doing so. Mathew et al. 24 also included a high proportion of patients with migraine (63%), which might increase the risk of misdiagnosis because scalp tenderness (a common symptom in migraine) can mimic a positive Tinel's sign. 27 Thus, the physical examination finding of scalp tenderness, which is often seen in migraine, might be incorrectly interpreted as a positive Tinel's sign, leading to a potential misdiagnosis of ON. Second, Mathew et al. 24 had a smaller sample (n = 800) compared with Martinéz-Pías et al. 21 (n = 5515) and Pedraza et al. 17 (n = 2338). Smaller samples are more susceptible to bias from sampling variation. 28 Third, the studies used different ICHD editions. Mathew et al. 24 used ICHD-3, Martinéz-Pías et al. 21 used ICHD-2 and 3β, and Pedraza et al. 17 only used ICHD-2. The 2nd edition lacks criteria for laterality, recurrence, duration, pain quality and associated symptoms, and describes any occipital headache not specifically as neuralgia. 6 We would expect that studies using ICHD-2 criteria would report a higher proportion of ON because of its broader criteria. However, this was not the case. It is also worth noting that none of the ICHD editions require a set number of attacks or a specific period over which attacks must occur to qualify for an ON diagnosis, which might also introduce heterogeneity.1,6,7 Fourth, Mathew et al. 24 used 5.5 ml of 0.75% bupivacaine and 0.5 ml of triamcinolone acetonide (20 mg), Martinéz-Pías et al. 21 used 2 ml of 1% lidocaine, and Pedraza et al. 17 used a 1:1 mixture of 0.5% bupivacaine and 2% mepivacaine. Different concentrations might yield different degrees of nerve block. Martinéz-Pías et al. 21 defined a positive response to blocks as complete relief of pain for at least 24 hours, whereas Pedraza et al. 17 employed a simple yes/no system. Mathew et al. 24 did not report their method for assessing response.
In summary, the notable variation in the reported relative frequencies of ON across studies can be attributed to differences in diagnostic criteria, sample sizes, comorbidity rates and methodologies for assessing nerve block response. Future research should aim to standardize these factors to improve the comparability and reliability of findings.
ON versus primary stabbing headache
The most important differential diagnosis for ON is primary stabbing headache (PSH). Both disorders share a stabbing pain quality that lasts from a few seconds to a couple of minutes. 1 However, our meta-analysis highlights distinctions that can aid in precise diagnosis. The location of pain is crucial because almost all cases of ON affect the greater occipital nerve (98%). By contrast, PSH primarily involves the first division of the trigeminal nerve, which innervates the vertex of the head. Additionally, hypoesthesia was present in most ON cases (73%), whereas it has not been described in the clinical presentation of PSH.
ON versus post-traumatic headache
The ICHD-3 classifies ON as both a primary and secondary pain disorder. 1 This dual classification can be confusing, especially because 30% of individuals with ON report a history of neck trauma, potentially overlapping with post-traumatic headache. Although both disorders can theoretically present with unilateral, stabbing occipital pain, their clinical presentations differ considerably. Post-traumatic headache typically manifests as a pressing or throbbing headache lasting from hours to days, 1 whereas ON is characterized by neuralgic pain with a shooting or stabbing quality, occurring in paroxysms lasting seconds to minutes. This overlap, combined with the lack of a clear secondary classification for ON, complicates diagnosis, particularly in cases triggered by trauma.
ON versus other differential diagnoses
In addition to traumatic etiologies, future research should explore a broader range of secondary causes that might underlie ON, such as multiple sclerosis or viral infections. Such efforts could reveal distinct clinical features of ON based on the underlying etiology and hold therapeutic implications. Further research is thus needed to address these gaps in understanding the clinical presentation and pathogenesis of ON.
Other important, although less common, differential diagnoses include Eagle's syndrome and cervicogenic headache, both of which are managed with nerve blocks. 1 Eagle's syndrome is treated through transpharyngeal injection of steroids and lidocaine, whereas cervicogenic headache is diagnosed and treated by blocking a cervical structure or its nerve supply.1,29 This overlap in treatment methods can complicate differentiation based on location and treatment alone. Understanding the cause of pain is essential for diagnosis: ON is most likely caused by inflammation or irritation of the occipital nerve, Eagle's syndrome by an elongated or calcified stylohyoid ligament, and cervicogenic headache by a disorder or lesion within the cervical spine or soft tissues of the neck.
Another rare differential is highlighted in a study by Larsen et al., 30 who found that 29% of patients with short-lasting unilateral neuralgiform headache attacks experienced pain outside the trigeminal distribution, within the C2–3 dermatome. This underscores the potential for misdiagnosis between ON and other rare headache disorders.
Diagnostic GON blocks
According to the current ICHD-3 criteria, the diagnosis of ON is confirmed by a positive response to GON blocks. 1 However, GON blocks are used for various types of headache disorders, 31 necessitating caution when applying ICHD-3 criteria for ON diagnosis. Although GON blocks can provide temporary relief in ON, relying heavily on the response to these blocks carries risks. A positive block does not definitively indicate ON because other headache disorders, such as migraine and cluster headache, can also respond to GON blocks. 31 This is particularly important given the high relative frequency of migraine among patients with ON. Moreover, there is no clear definition of what constitutes a positive response. The dosage, concentration and type of local anesthetic, as well as the required duration of relief, lack consensus.
Future directions
Case reports and case series with fewer than five participants were excluded to maintain methodological rigor and enhance comparability with larger observational studies. The threshold of five participants was chosen to balance minimizing bias and variability at the same time as ensuring adequate data for studying the relatively rare disorder of ON. However, we recognize that, despite this minimum, the statistical power of our meta-analysis may still be limited.
Beyond the limitations posed by the exclusion of smaller studies, our analysis also faced significant heterogeneity in individual clinical characteristics, warranting cautious interpretation. Almost all individual clinical characteristics were associated with considerable heterogeneity and should be interpreted with caution. Meta-regressions investigating this heterogeneity did not identify any single explanatory variable accounting for the observed variability. To address these limitations, future research on the clinical presentation of ON should rigorously follow the ICHD classification and transparently report both negative and positive GON block responses, along with the types of neck trauma experienced by patients.
The overlap between ON and other headache disorders, such as migraine, raises questions about the validity of ON as a distinct diagnosis based on the current literature. There are no clear guidelines on how treatment should be administered, and local anesthetic treatment is effective for other headache disorders as well. The ICHD provides classifications for primary and secondary headache disorders, but the categorization of ON remains ambiguous.
To better accommodate the diagnosis and management of ON, future ICHD editions need to clarify whether secondary etiologies play a role in ON, and, if so, whether a primary and idiopathic type even exists. Under the current classification, two isolated paroxysmal attacks meeting the diagnostic criteria within a multi-year period could, in extreme cases, merit an occipital neuralgia diagnosis, potentially qualifying for diagnosis in one study but being missed in another.
Conclusions
In conclusion, our results should be interpreted with caution as a result of considerable between-study heterogeneity. The relative frequency of ON among adults presenting with headache or facial pain in tertiary care settings exhibit substantial variability, ranging from 0.6 to 24.4%. Predominantly affecting females (73%) with an average onset age of 56 years, ON is characterized by severe (54%), stabbing (59%) and unilateral (81%) pain primarily localized to the greater occipital nerve (98%). Furthermore, almost half of the patients report co-morbid migraine (46%), and approximately one-third have a history of neck trauma (30%). These findings underscore the necessity for standardized diagnostic criteria to address existing heterogeneity and enhance the comparability of future studies. We advocate for adherence to the ICHD criteria in future research and suggest a re-evaluation of the role of GON blocks in the diagnostic process to reduce false positive and negative outcomes. Addressing these gaps is essential for advancing the understanding, diagnosis and management of ON, ultimately improving patient care and outcomes.
Among adult patients evaluated for headache or facial pain in tertiary care settings, the pooled relative frequency of ON ranged from 0.6 to 24.4%, underscoring the need for more accurate estimates. The clinical presentation of ON was predominantly unilateral (81%), almost exclusively affecting the greater occipital nerve (98%), with 73% presenting with hypoesthesia. The intensity of pain was mostly severe (54%) with a stabbing quality (59%). The lack of robust data and between-study heterogeneity limit the conclusions that can be drawn from the present meta-analyses. Further studies are needed to estimate the prevalence and relative frequency rates of ON using standardized methods of data acquisition.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251317595 - Supplemental material for Epidemiology and clinical features of occipital neuralgia: A systematic review and meta-analysis
Supplemental material, sj-docx-1-cep-10.1177_03331024251317595 for Epidemiology and clinical features of occipital neuralgia: A systematic review and meta-analysis by Anna G. Melchior, Sarra Al-Khazali, Rune H. Christensen, Haidar M. Al-Khazali and Håkan Ashina in Cephalalgia
Footnotes
Author contributions
HA conceived and designed (including search strategies) the review. AM did the literature search with SAK. AM wrote all drafts of the manuscript. AM participated in critical revision and writing of the article. All authors have seen and approved the final version of the manuscript submitted for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.