
Abstract
Background
One of the most underestimated types of chronic headaches is headaches as a result of cerebro-spinal fluid dysregulation disorders. Idiopathic intracranial hypertension (IIH) presents with headache and visual symptoms and usually is associated with papilledema. We identified patients with IIH in a chronic headache population presenting to a hospital-based headache clinic, and studied its associations with clinical, sonographic and magnetic resonance imaging (MRI) findings.
Methods
Of 168 patients, 141 chronic headache patients were identified and completed the study procedures (semi-structured medical interview, fundus examination, MRI brain with magnetic resonance venography (MRV) and trans-orbital sonography (TOS)). Patients with abnormal findings underwent lumbar puncture for opening pressure.
Results
The prevalence of IIH was 27%. IIH patients were of higher age, had gnawing/throbbing headache in the vertex in most cases, and had higher body mass index. Fundus examination had a sensitivity of 79% and a specificity of 98% for the detection of IIH cases. Approximately 23% of IIH patients had no papilledema. The most sensitive MR sign was found to be transverse sinus stenosis. TOS showed optic nerve sheath dilation in 35.7% of IIH without papilledema cases.
Conclusions
The prevalence of IIH is high in the chronic headache population and should be suspected in the headache clinic setting, particularly because there is significant overlap with migraine symptomatology. MRI/MR venography and TOS can be useful adjunct tests to identify IIH patients.
Keywords
Introduction
Headache disorders are a leading cause of disability worldwide, with migraine being the second cause of years lived with disability (1). The International Headache Society (IHS) defines chronic headaches as headaches affecting an individual for ≥15 days in one month (2). Cerebro-spinal fluid (CSF) dysregulation headaches, which include any headache as a result of abnormalities of CSF pressure and volume, represent one of the most underestimated causes of chronic headache (3). Headaches attributed to low CSF pressure include post-dural puncture headache, CSF fistula headache and spontaneous intracranial hypotension (4). On the other hand, idiopathic intracranial hypertension (IIH) is characterized by the elevation of intracranial pressure of more than 250 mmH2O with the absence of a mass lesion or hydrocephalus on brain imaging (5). The most common symptoms of IIH are headache and visual affection (6). Most cases of IIH are associated with papilledema, although those with no papilledema could pass undiagnosed as chronic migraine or tension-type headache unless the exclusion of increased CSF pressure is performed by lumbar puncture (LP) (7). Given this overlap, a high index of suspicion and the use of clinical criteria and adjunct tests is necessary to avoid misdiagnosis. In the present study, we aimed to identify patients with IIH in a hospital-based chronic headache population and to assess the association between IIH and clinical, sonographic and magnetic resonance imaging (MRI) brain and magnetic resonance venography (MRV) findings.
Methods
This study was an investigation of consecutive patients attending the headache clinic at Ain Shams University Hospitals (a tertiary hospital serving eastern Greater Cairo) between November 2022 and April 2023. Using the PASS 15 program (www.ncss.com/software/pass/) for sample size calculation and setting the confidence level at 95% and margin of error at 5%, it was estimated that a sample size of at least 140 patients was needed to detect an expected prevalence of CSF dysregulation-related headache disorders of 10% among this headache population.
Patients of both genders were included if they presented with chronic headaches (headache affecting an individual for ≥15 days in one month (2) for at least three months) and were aged >18 years. We excluded patients with secondary headaches attributed to trauma, substance abuse or withdrawal, infection, a disorder of the cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, other facial or cervical structure, major psychiatric illness, or vascular disorder, and those with contraindications to MRI exposure such as pacemakers.
All patients gave informed consent, and the study was approved by the ethical committee of the Neurology and Psychiatry department, Faculty of Medicine, Ain Shams University (FWA 000017585).
For all patients, history was taken using a semi-structured medical interview (taking in consideration duration of headache, prior headache history, use of medication, tinnitus, vertigo/dizziness, neck pain, double vision and other visual symptoms). Transitory visual obscurations and pulsatile tinnitus were particularly sought out as characteristic symptoms of IIH. We classified headaches according to the International Classification of Headache Disorders, 3rd edn (ICHD-3). Neurologic examination including fundus examination was also done. Fundus examination was performed by neurologists well-trained on direct ophthalmoscopy, and moreover, patients were referred to ophthalmology department at Ain Shams University Hospitals for confirmation and grading of papilledema through slit lamp examination. No fundus photos were taken. All patients had an MRI brain with MRV without contrast with or without thin cut fat suppressed orbital sequences using a 1.5 T MR scanner (Achieva and Ingenia; Philips Medical Systems, Eindhoven, The Netherlands), looking for signs suggestive of IIH, namely: empty sella turcica, transverse sinus stenosis, posterior globe flattening, optic nerve head protrusion and optic nerve sheath distention or tortuosity (Figure 1). For an empty sella sign, it was assessed in the sagittal plane. For flattening of the posterior aspect of the globe and distention of perioptic subarachnoid space with a tortuous optic nerve, those were considered positive if present unilaterally or bilaterally. All radiological findings were evaluated by expert neuroradiologists at Ain Shams University Hospitals radiology department who were blinded to the diagnosis and not directly involved in our study. LP (in an outstretched relaxed left lateral decubitus position with both legs and neck extended) was used to confirm intracranial hypertension in all the suspected cases of IIH either clinically or those having positive findings suggestive of IIH on MRI/MRV and those having papilledema on fundus examination. Additionally, Trans-orbital sonography (TOS) for measurement of optic nerve sheath diameter (ONSD) was performed for patients scheduled for LP to confirm IIH. TOS was performed when subjects were supine and with the upper part of the body and head elevated to 20–30° with their eyes in a mid-position to suppress eye movements. A linear array probe was placed on the temporal part of the closed upper eyelid using a thick layer of ultrasound gel. The anterior part of the optic nerve was depicted in an axial plane showing the papilla and the optic nerve in its longitudinal course. ONSD was assessed 3 mm behind the papilla by measuring the distance between the external borders of the hyper-echogenic area surrounding the optic nerve. A cutoff value of 6 mm or above was considered dilated (8)

Examples of magnetic resonance imaging (a, c, d, e, f) and magnetic resonance venography (b) signs suggestive of idiopathic intracranial hypertension.
Statistical analysis was done on Statistical Package for Social Science (SPSS, version 25; IBM Corp., Armonk, NY, USA). The comparison between groups regarding qualitative data was performed using the chi-squared test. The comparison between independent groups with quantitative data and parametric distribution was performed by using an independent t-test and one-way analysis of variance.
Results
During the study period, 168 patients with headache who attended the headache clinic at Ain Shams University Hospitals were identified fulfilling the inclusion and exclusion criteria. Of those, 141 chronic headache patients were available for the required investigations and follow-up and completed the study.
Clinical characteristics
The mean ± SD age of the patients was 33.6 ± 10.1 years, with predominately females (77%), and with 22% of patients having a positive family history of migraine. We calculated the body mass index (BMI) at the time of enrollment to be 24.9 ± 2.5 for the whole group.
Regarding the site of headache, most of the patients (41%) had unilateral temporal pain, 18% patients had vertex pain, 15% patients had occipital pain, 15% patients had bi-temporal pain, 7% patients had bi-frontal pain and 2% patients had hemi-cranial pain. Regarding the character of headache, most of the patients (52%) reported gnawing/throbbing pain, 31% of patients had dull aching pain, 13% of patients had electric-like pain and 3% of patients had pressure/tight-band pain.
MRI findings
MRI was performed for all patients and showed findings suggestive of idiopathic intracranial hypertension such as an empty sella turcica sign in 22 patients (15%), transverse sinus stenosis signs in 52 patients (37%), a posterior globe flattening sign in 11 patients (8%), optic nerve head protrusion signs in 16 patients (11.%), and optic nerve sheath distention or tortuosity in 25 patients (18%).
Confirmation of diagnosis
The final diagnosis of type of chronic headache is shown in Table 1. We first sorted all patients according to clinical data, then all of them were subjected to fundus examination and MRI brain with MRV. Of the 141 patients, 59 cases were suspected as cases of IIH and underwent LP for opening pressure measurement.
Final diagnosis of patients with chronic headache in the study sample.

Abbreviations: IIH: idiopathic intracranial hypertension; MRI: magnetic resonance imaging; MRV: magnetic resonance venography.
According to the Revised Friedman criteria of IIH, 39 cases were finally confirmed as IIH, whereas according to the Korsbaek criteria of IIH, 51 cases were confirmed as IIH (9,11) (Figure 2).

Recruitment and study procedures. Abbreviations: IIH: idiopathic intracranial hypertension; MRI: magnetic resonance imaging; MRV: magnetic resonance venography.
As per Table 2 according to the Revised Friedman criteria, of the 39 cases of IIH, 30 cases were definite IIH cases, whereas only nine were probable IIH, and 13 cases who were considered as IIH cases by the Korsbaek criteria were ruled out by the Revised Friedman criteria because they did not have sufficient MRI signs suggestive of IIH (i.e. not having three MRI signs out of four signs), although they had increased intracranial tension as measured by opening pressure assessment (Figure 2).
Comparison between using Revised Friedman criteria and Korsbaek criteria for detection of IIH cases.

Abbreviation: IIH: idiopathic intracranial hypertension.
Comparison of confirmed IIH patients to non-IIH patients
Clinical features
Table 3 shows there was a statistically significant difference between IIH, and other types of headaches regarding the site of headache, being more unilateral temporal in the non-IIH group vs. being in the vertex in the IIH group (p = 0.055).
Comparison of clinical characteristics between confirmed IIH and Non-IIH chronic headache patients according to Revised Freidman criteria regarding studied parameters.

Abbreviations: IIH: idiopathic intracranial hypertension; IQR: interquartile range.
There was a highly statistically significant difference between IIH and other types of headaches with respect to BMI, with a higher BMI in the IIH group, and the character of headache being gnawing/throbbing in 94.9% of IIH patients (p < 0.001 and p < 0.001 respectively). There was no significant difference between IIH and other types of headaches related to age, sex and duration of headache in years.
MRI and MRV
Table 4 compares the MR signs in confirmed IIH patients to non-IIH patients. We also determined the specificity and the sensitivity of each MRI sign in detecting true IIH (Figure 3 and Table 4). The results show that, for the detection of IIH cases, the empty sella turcica sign has a sensitivity of 46%, specificity of 96% and accuracy of 82%; the transverse sinus stenosis sign has a sensitivity of 87%, specificity of 82% and accuracy of 84%; the posterior globe flattening sign has a sensitivity of 23%, specificity of 98% and accuracy of 77%; the optic nerve head protrusion sign has a sensitivity of 31%, specificity of 96% and accuracy of 78%; and the optic nerve sheath distention/tortuosity sign has a sensitivity of 43%, specificity of 92% and accuracy of 79%.

Receiver operating characteristic curve for the diagnostic accuracy of magenetic resonance signs in the detection of idiopathic intracranial hypertension cases.
Diagnostic accuracy of MRI and MRV in the detection of IIH cases.

Abbreviations: IIH: idiopathic intracranial hypertension; TP: true positive; TN: true negative; FP: false positive; FN: false negative; PPV: positive predictive value; NPV: negative predictive value.
Papilledema
The results shown in Table 5 indicate that, in patients with chronic headache with normal fundus examination, there is a possibility that almost one-fifth of cases have IIH as the final diagnosis (i.e. IIH without papilledema; IIHWOP).
Relation between fundus examination results and the type of headache confirmed by lumbar puncture with diagnostic accuracy of fundus examination in the detection of IIH cases.
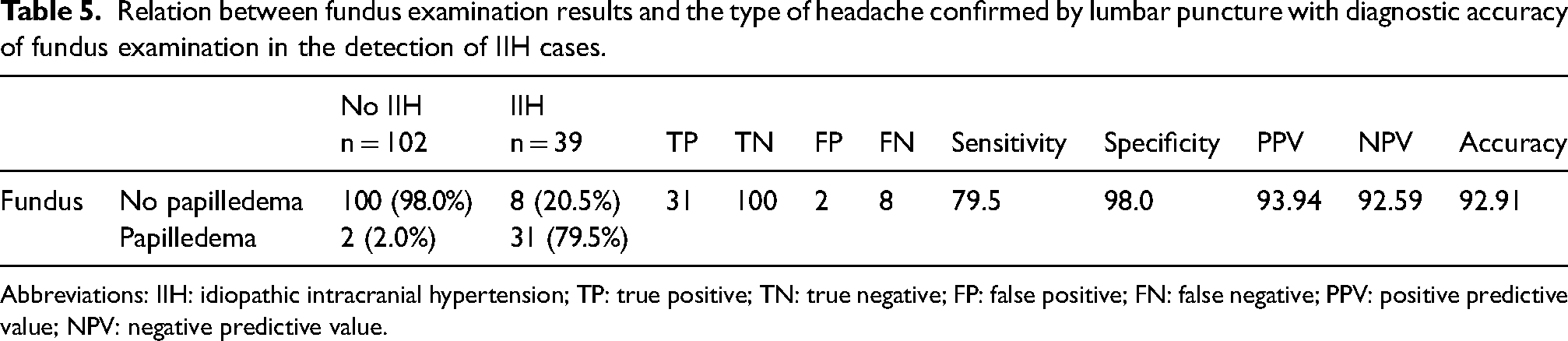
Abbreviations: IIH: idiopathic intracranial hypertension; TP: true positive; TN: true negative; FP: false positive; FN: false negative; PPV: positive predictive value; NPV: negative predictive value.
Figure 4 and Table 5 show that fundus examination has a sensitivity of 79.5%, specificity of 98% and accuracy of 92% for the detection of IIH cases.

Receiver operating characteristic curve for the diagnostic accuracy of fundus examination in the detection of idiopathic intracranial hypertension cases.
Opening pressure
The results showed that, for patients with IIH assessed by LP, their opening pressure ranged from 27 to 77 cmH2O (mean ± SD = 35.96 ± 11.41) whereas those who were ruled out had an opening pressure ranging from 6 to 23 mmH2O (mean ± SD = 18.9 ± 5.59).
ONSD
There was a highly significant association between TOS ONSD and opening pressure on LP (opening pressure = 40.82 ± 13.34 vs. 30.04 ± 3.16 for dilated vs. non-dilated ONSD respectively; p < 0.001). Also, BMI was higher in patients who had dilated ONSD on TOS (26.96 ± 2.43 compared to those with normal ONSD (25.96 ± 1.85); p < 0.001).
Comparison of TOS to MRI/MRV showed that there was a significant association between TOS ONSD and optic nerve head protrusion sign on MRI p = 0.004).
Table 6 shows the relationship of fundus exam findings to TOS ONSD. Importantly, 35.7% of IIHWOP cases had dilated optic nerve sheath diameter through assessment by TOS.
Fundus examination findings for dilated and non-dilated ONSD (mm) on trans-orbital sonography.

Abbreviations: IIH: idiopathic intracranial hypertension; ONSD: optic nerve sheath diameter.
Discussion
In the present study, we report for the first time the detection of IIH cases among a chronic headache population presenting to a hospital-based clinic and show that it is rather high (27%). The study also shows that fundus examination, despite its high specificity, misses a significant proportion of IIH patients (20% of confirmed IIH patients were non-papilledemic IIHWOP). MRI combined with MRV was useful in identifying IIH patients with a very high specificity for most signs, although only the transverse sinus stenosis sign had a sufficiently high sensitivity to be clinically reliable. We also showed that assessment of ONSD using TOS can support the diagnosis by identifying some of the IIHWOP cases.
The high prevalence of IIH found in the present study may be because of improved case ascertainment, prospective recruitment of patients and the fact that we studied a population of chronic headache patients presenting to a specialized headache clinic in a tertiary university hospital. Many of these patients are incorrectly diagnosed as having chronic migraine, especially because the overlap of clinical symptoms between IIH and migraine is considerable (12). In the general population, there are many reports of the prevalence of IIH being 10.9/100,000. In a retrospective case review conducted in Sheffield, UK, it was reported that it may be as high as 76/100,000 (10,13). To the best of our knowledge, there are no published data on the prevalence of IIH in the clinic setting among the chronic headache population enabling a comparison with our results.
The present study used two sets of criteria for the detection of IIH cases. Using the Revised Friedman criteria, we found IIH cases to be around 27% of patients in the sample, whereas, using the Korsbaek criteria, we detected higher cases, reaching 36% of cases. The discrepancy is mainly for those patients with no papilledema on fundus examination as we revert to MRI brain with MRV signs suggestive of IIH. Furthermore, in our study, we found that some patients who have only two MRI brain signs suggestive of IIH also have a high opening pressure of >25 cmH2O but <30 cmH2O. Thus, if we applied the Revised Friedman criteria, those patients would be diagnosed as other types of headaches rather than IIH. Those patients probably lie in a borderzone area between migraine and IIH, which is the subject of many recent studies.
The key role of imaging in the diagnosis of IIH is to exclude secondary causes of raised intracranial pressure and papilledema. However, various MRI signs became recognized as neuroimaging markers of IIH, although the estimates of their occurrence, sensitivity, specificity and relevance differ widely in the published literature with a paucity of studies (14). Korsbæk et al. (10) found, in a diagnostic study on a large cohort of patients with clinically suspected, new-onset IIH, that moderate suprasellar herniation, distension of the perioptic subarachnoid space, flattening of the posterior aspect of the globe and bilateral transverse sinus stenoses were highly associated with IIH and elevated opening pressure (10). Bidot et al. (14) found that severe bilateral transverse sinus stenosis is present on MRV in almost 100% of people with IIH in contrast to Prabhat et al. (15), who detected transverse sinus stenosis on MR venography in only (62.5%) of the patients. Farb et al. (16) found that bilateral sino-venous stenosis was seen in 27 of 29 patients with IIH and only four of 59 control patients had a sensitivity and specificity of 93%. Also, Korsbæk et al. (10) found transverse sinus stenosis to have a significant relation with IIH (60.2 vs. 18.9%), with the different incidences related to different sampling size, sampling method and different techniques of imaging and assessment. Overall, our findings agree with those studies reporting that transverse sinus stenosis could be a highly accurate sign for being used in early detection and exclusion of IIH. The empty sella turcica sign of MRI had a sensitivity of 40.4% in our sample and a specificity of 99%, such as in the study by Patterson et al. (17), who found that the cross-sectional area of the Sella was 38% greater in people with IIH than those without with only slight reduction in the size of the pituitary gland. Prabhat et al. (15) found that empty sella was present in (68.8%) of patients, whereas Jones et al. (18) found that it was only in (33.1%) of patients, with the results in the previous and current studies suggesting empty sella turcica sign to be more of a specific sign that could be used as a good positive sign for IIH, although it would not be helpful in early detection, nor for the exclusion of IIH.
Prabhat et al. (15) found that optic nerve tortuosity was the most sensitive sign on neuroimaging (82.5%) followed by posterior scleral flattening (80%), and the least sensitive sign was transverse sinus stenosis. This is not in agreement with our findings. Prabhat et al. (15) also found the partial empty sella sign had a sensitivity of 68.75% and a specificity of 76.67%. Again, the divergent results are probably a result of the different case ascertainment and imaging methods. This emphasizes the importance of consensus criteria that use a composite of several MRI signs to make the diagnosis.
In the present study, IIHWOP was not uncommon even though several earlier studies considered it to be less prevalent. We performed lumbar punctures for all suspected cases of IIH, whether clinically or on MRI/MRV, and this probably led to a more accurate capture rate of true IIHWOP. In a study of 45 patients, Favoni et al. (19) found a low prevalence (2.5%) of IIHWOP in refractory chronic headache patients, with 39 patients being diagnosed as chronic migraine patients, and the rest as chronic tension-type headache with concomitant episodic migraine. Similarly, Digre et al. (20) found that only 5.7% of patients diagnosed with IIH do not have papilledema. On the other hand, Mathew et al. (21) reported that 15% of patients with chronic headaches (n = 85) had increased intracranial pressure (>250 mm CSF) and no papilledema. Vieira et al. (22) also found that 21.5% of patients diagnosed with chronic migraine actually had idiopathic intracranial hypertension, with 11.5% having IIH with papilledema, and 10% had IIH without papilledema. It is in general still unknown how papilledema can be absent despite elevated intracranial pressure. It may be hypothesized that intracranial pressure waves, which are variable over time, rather than absolute pressure may be responsible for the dilation and may be different in the subset of patients with IIHWOP.
TOS is a rather simple bedside test that can be integrated easily into clinical practice. We did not find it to be very sensitive (around 46% of confirmed IIH patients had a non-dilated ONSD on TOS in our sample), but it was useful in correctly identifying at least one-third of IIHWOP cases. Several studies have reported on the use of TOS in IIH such as that by Dağdelen & Ekici (23), who found that the mean ONSD was significantly thicker in the IIH patients (6.4 mm) compared to the control group (4.9 mm) with a cut-off value of ONSD in patients with IIH measured as 5.7 mm. However, there is no consensus on the optimum cut-off values to be used and this may contribute to the low sensitivity. In the present study, the TOS findings correlated well with some of the MRI signs of IIH related to the optic nerve and globe, and this was also seen in a few other studies such as those by Patterson et al. (17) and Roemer et al. (24) and, as such, this suggests that TOS may be useful in raising the suspicion of IIH when MRI is not available .
This study has limitations related to the nature of the sample population studied. Patients with chronic headache who present to specialized headache clinics in tertiary centers are likely to be treatment-resistant patients with a long disease duration. Therefore, it might not be representative of the entire chronic headache patient population. A study on a larger sample in a different setting can confirm the findings in the wider headache population. Additionally, we did not perform LP on all the patient population that we recruited, but only on patients suspected to have IIH, which potentially means that a patient might still have had raised intracranial pressure but was missed because they did not have clinical, sonographic or MRI signs. Finally, we did not repeat the study procedures longitudinally over time and therefore cannot make any conclusions regarding the evolution or change of the signs we studied over time.
Conclusions
The prevalence of IIH in this hospital-based chronic headache population is high and should be suspected in cases of chronic headache, particularly because there is significant overlap with migraine symptomatology. MRI/MRV and TOS can be useful adjunct tests to identify IIH patients.
The prevalence of IIH is high (27%) in the chronic headache population. IIH should be suspected in the headache clinic setting in resistant chronic headache, particularly because there is significant overlap with migraine symptomatology. Approximately one-quarter of IIH patients might not have papilledema. MRI/MRV and TOS can be useful adjunct tests to identify IIH patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical statement
The study was approved by the ethical committee of the Neurology and Psychiatry department, Faculty of Medicine, Ain Shams University (FWA 000017585). All patients provided their informed consent.