
Abstract
Chronic migraine (CM) has been associated with idiopathic intracranial hypertension without papilloedema (IIHWOP), a significant percentage of these cases occurring in obese patients with intractable headache. A prospective study from February 2005 to June 2006 was made of 62 CM patients who fulfilled International Headache Society diagnostic criteria and had cerebral magnetic resonance venography (MRV) and lumbar puncture (LP) done. Two patients were excluded, six (10%) with elevated cerebrospinal fluid (CSF) open pressure (OP), five with body mass index (BMI) > 25. None of the patients had papilloedema or abnormal MRV. BMI and CSF OP were significantly correlated (r = 0.476, P < 0.001, Pearson's correlation test). Obesity (defined as BMI > 30) was a predictor of increase in intracranial pressure (defined as OP > 200 mmH2O) (f = 17.26, 95% confidence interval 6.0, 8.6; P < 0.001). From our study we strongly recommend that not only intractable CM patients with high BMI, but also first diagnosed patients with BMI > 30 should be systematically evaluated by a LP to rule out IIHWOP.
Introduction
Chronic migraine (CM) is characterized by a headache (tension-type and/or migraine) that persists for ≥ 15 days per month for at least 3 months, being on ≥ 8 days per month a headache that fulfils criteria for pain and associated symptoms of migraine without aura, not attributed to another causative disorder (1, 2). It is a prevalent and debilitating disorder affecting 2–3% of the generation population (3).
Idiopathic intracranial hypertension (IIH), also known as benign intracranial hypertension, is a syndrome characterized by headache and elevated cerebrospinal fluid (CSF) pressure, with normal neurological examination or any the following abnormalities: (i) papilloedema; (ii) enlarged blind spot; (iii) visual field defect; or (iv) sixth nerve palsy, and normal laboratory and radiological examinations. Noises in the head, pulsatile tinnitus, transitory visual obscurations and diplopia can also occur (4, 5).
Chronic daily headache (CDH) has been associated with IIH. Since 1972, when Lipton and Michelson (6) reported the first case of idiopathic intracranial hypertension without papilloedema (IIHWOP), several authors have reported patients with headache and IIHWOP. The percentage of IIHWOP in refractory chronic/transformed migraine patients ranges from 5 to 14% (7, 8). Other authors have reported similar cases (9–11), and all patients studied were refractory patients seen at tertiary headache centres (6–12). It is unknown whether IIH is also common in a consecutive patient population. We aimed to analyse the prevalence of IIH in a consecutive and treatment-naive CM population.
Methods
Sixty-two patients (10 men and 52 women, ages 15–69 years, mean age 37.9 years) were diagnosed with CM according to International Headache Society criteria 2004 (1) and Appendix 2006 (2), and were consecutively enrolled from January 2005 to June 2006 from all patients attending at the Brain Research Institute—Hospital Israelita Albert Einstein, São Paulo, Brazil. All these patients had a history of episodic migraine, but had subsequently developed frequent migraine. The patients were referred from a basic health programme, in a community near the hospital, representative of the general population where regular visits are performed monthly by health agents, who were trained by the research team. Patients were not exposed to previous migraine prevention treatments. All 62 patients suffered from daily headaches at the time of the study. Clinical history was obtained by the authors. Interviews and neurological examinations were performed by two neurologists (D.S.S.V. and M.R.M.), supervised by the senior author (M.F.P.P.). Body mass index (BMI; weight in kilograms divided by the square of height in meters) was recorded in all patients. Informed consent was obtained from all subjects; the study was approved by the local ethics committee. All patients underwent both magnetic resonance imaging (MRI) and MR venography (MRV) of the brain on a 1.5-T whole-body imaging system. Two patients were excluded: a woman who had chronic meningitis by cysticercosis, and another woman with IIH with papilloedema, both of whom had migrainous features. All patients had a lumbar puncture (LP), which was performed with the patient positioned in the lateral decubitus position on a level surface. A standard 22-G spinal needle was used. The opening pressure (OP) was recorded by using a manometer positioned at a 90° angle to the spinal canal with the patient's knees and hip in the extended position and neck straightened. CSF pressure was recorded until the patient was relaxed and the pressure values had stabilized. All LPs were performed by the same investigator (D.S.S.V.). Increase in CSF was considered when the OP was > 200 mmH2O.
Statistical analysis was performed in order to assess the relationship of BMI and obesity with the increase in intracranial pressure measured by the CSF OP at LP. BMI and OP values were plotted using Pearson's correlation test. We also tested the hypothesis that obesity predicted increase in intracranial pressure using a linear model of regression, with confidence interval (CI) of 95%, considering in all tests statistically significant values < 5%.
Results
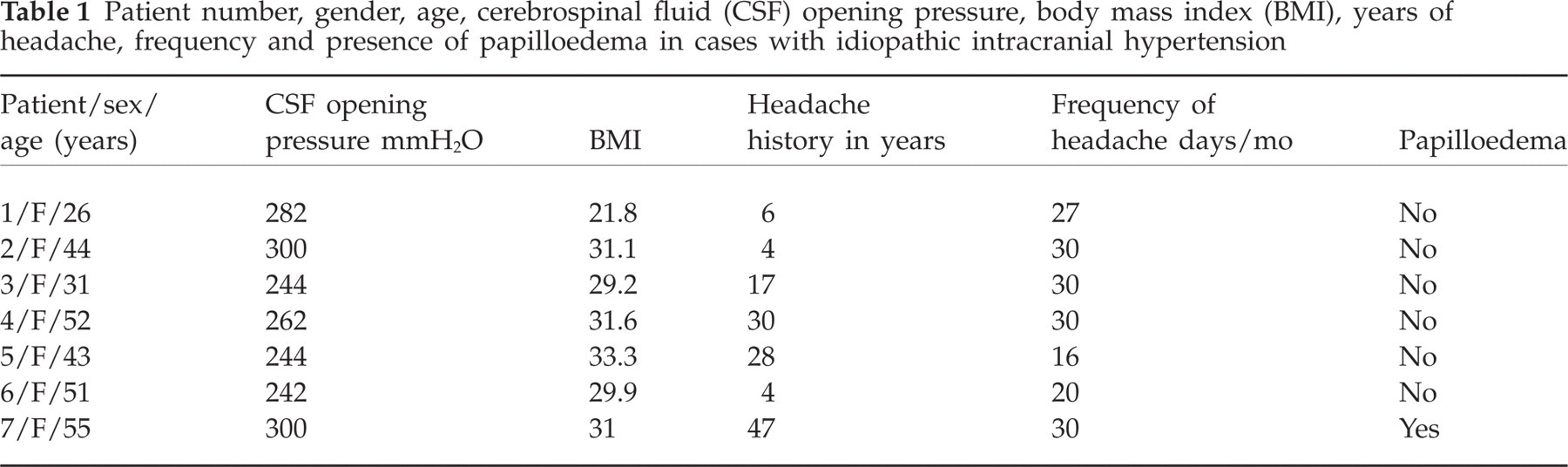
Seven patients out of 61 (11.47%) with CM had IIH. Excluding one patient with IIH with papilloedema, six patients out of 60 (10%) had IIHWOP. No patient had papilloedema, visual field defects or diplopia, or any history or clinical and laboratory signs of endocrine, metabolic, inflammatory or haematological disturbances. One patient had normal BMI, two patients BMI > 29 (overweight) and three patients BMI > 30 (obese). Ages ranged from 26 to 52 years. All patients had normal MRI and MRV. The clinical characteristics of patients studied at presentation are summarized in Tables 1 and 2.
Patient number, gender, age, cerebrospinal fluid (CSF) opening pressure, body mass index (BMI), years of headache, frequency and presence of papilloedema in cases with idiopathic intracranial hypertension
Clinical features, treatment responses in patients diagnosed with idiopathic intracranial hypertension
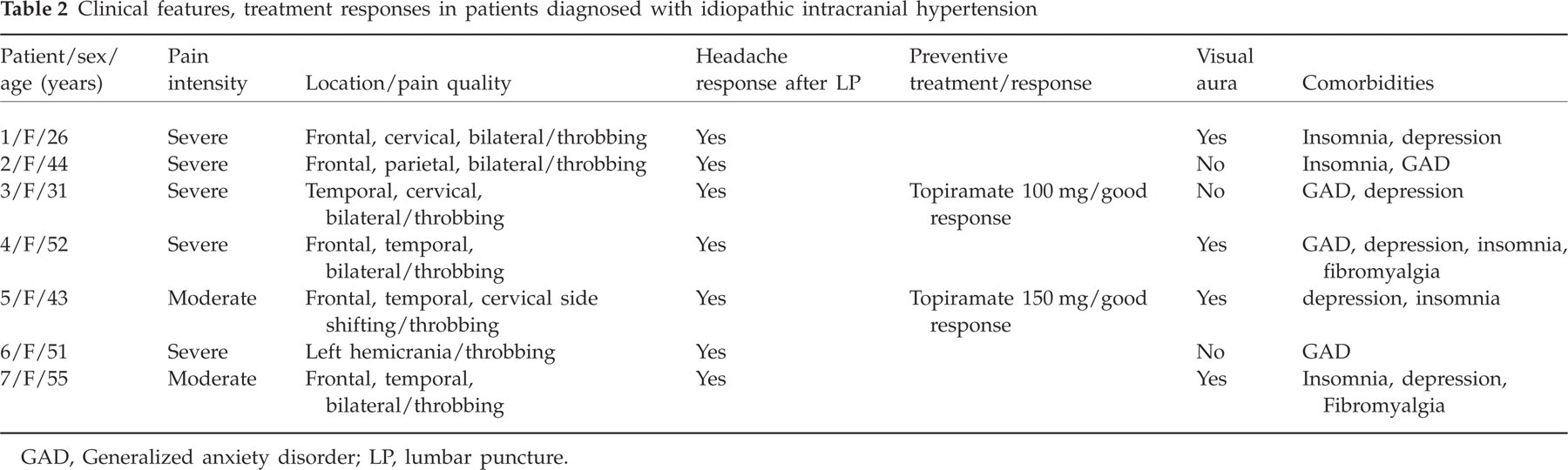
GAD, Generalized anxiety disorder; LP, lumbar puncture.
Follow-up and treatment rationale
Patient follow-up ranged from 6 to 18 months. All patients had significant relief immediately after the LP, sustained at least until 1 week after; they had not received preventive medication at this point. Three patients (no. 3, 5 and 6) had their headache frequency increased after 1 month; they were re-examined and had again elevated OP in the same range. Two patients were put on topiramate with good results, one patient was lost to follow-up. Two patients had sustained and significant improvement of headache, with no need for pharmacological prevention. We put patients on topiramate, patient 3 increased until 100 mg, headaches deceased > 75%, stayed on 100 mg with good control; patient 5 reached good control with 150 mg a day. The rationale for topiramate in these patients was the need for weight loss, good headache control and mood stabilization.
Overweight or obesity were found in 33 (55%) of 60 patients. BMI and CSF OP were significantly correlated (r = 0.476, P < 0.001, Pearson's correlation test). Obesity (defined as BMI > 30) was a predictor of increase in intracranial pressure (defined as OP > 200 mmH2O) (f = 17.26, 95% CI 6.0, 8.6, P < 0.001). The graph (Fig. 1) shows the correlation between BMI and OP.
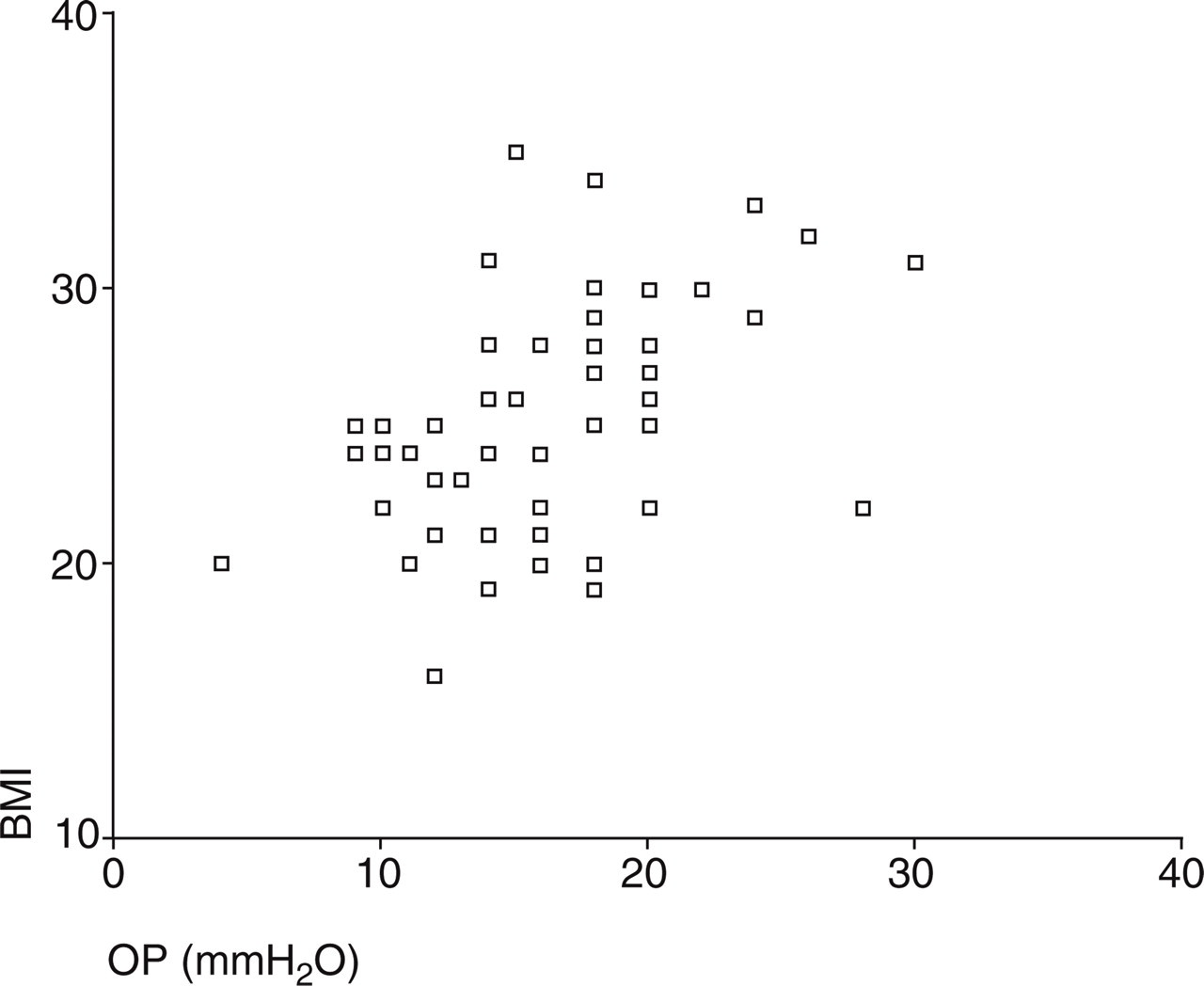
Correlation of body mass index (BMI) with cerebrospinal fluid opening pressure (OP) in chronic migraine.
Discussion
Our study shows a high prevalence of IIH in a consecutive and treatment-naive CM population, and the results are similar to previous findings in refractory CDH populations.
IIH is most common in women and obese individuals. Female : male ratios range from 4:1 to 15:1. Obesity in IIH patients is found in 71–94%. The pathophysiological relation between obesity and IIH remains unclear, and hypotheses such as increased cerebral venous pressure resulting in raised intra-abdominal pressure and endocrine dysfunctions have been suggested (4).
Recent studies have reported that obesity is not comorbid with migraine, but is related to the severity and frequency of headache attacks experienced by migraineurs as well as of associated symptoms (13). Obesity has also been found to be a risk factor for transformed migraine, associated with frequency and severity, but not for chronic tension-type headache (14).
In our case series, it was found that overweight and obesity were frequent in patients with chronic/transformed migraine, where 28 (46.6%) patients had BMI > 25 without IIH. In our series, only one patient with IIHWOP had a BMI < 25.
Some authors have reported CSF pressures > 200 mmH2O in healthy obese subjects (15), not necessarily with a diagnosis of IIH. Corbett and Mehta reported 25% of 41 normal obese subjects had CSF pressure values between 200 and 250 mmH2O (16). Hannerz et al. have described 15 of 19 obese patients with CSF pressures > 200 mmH2O in women with signs of inflammation in serum (17). However, Bono et al. have reported CSF pressures no higher than 200 mmH2O in 18 obese and 33 overweight patients with normal MRVs who underwent lumbar puncture, showing that overweight/obesity per se do not induce OP > 200 mmH2O (18).
Quattrone et al. have reported that 10 of 11 patients with CDH and signs of cerebral venous thrombosis (CVT) on MRV had BMI > 25, of whom five had intracranial hypertension with OP > 200 mmH2O (8). Mathew et al. have reported 12 of 85 CDH patients with migrainous features who were refractory to conventional therapy as having IIHWOP, seven of whom were obese (7).
Healthy obese subjects may have CSF pressure above the upper limit of the normal range (200 mmH2O) (15–17), but Bono et al. have recently shown that excess body weight has a slight effect on CSF pressure in subjects with normal MRV (18); the same group reported bilateral transverse sinus stenosis (BTSS) to be a strong factor related to IIHWOP in patients with daily headaches with migraine features (19), although another study (20) found disturbances of flow in one or both transverse sinus in 45 out of 111 patients with normal opening CSF pressure. BTSS or disturbances of venous flow were not found in our study.
Quattrone et al. found all patients with chronic migraine, IIHWOP and signals of CVT were obese or overweight (8). In studies (16, 17) showing elevated CSF pressure values in healthy obese individuals, no subject underwent MRV; the possibility of increased CFS pressure caused by CVT/BTSS cannot be excluded. Whiteley et al., studying 242 consecutive out-patients who underwent a LP for a neurological diagnosis, found a median opening pressure of 170 mmH2O (range 90–280 mmH2O) with a 95% reference interval for the distribution from 100 mmH2O (2.5 percentile) to 250 mmH2O CSF (97.5 percentile). There was a significant correlation between CSF opening pressure and BMI, but not relevant to clinical practice (21, 22).
If we follow more strict criteria for IIHWOP, taking into account only patients with OP > 250 mmH2O, we would have to disregard three patients, but three other patients would still be diagnosed as IIHWOP and one with IIH with papilloedema, in total four of 61 consecutive patients (6.5%)—a significant percentage. Nevertheless, we are confident with the diagnosis of IIHWOP in those two patients with OP 244 mmH2O, and in the one with 242 mmH2O, because of the headache response after LP and clinical outcomes.
IIH was found in a significant percentage in our case series of consecutive CM patients. We strongly recommend that not only intractable CM patients with high BMI, but also first diagnosed patients with BMI > 30 should be systematically evaluated by a LP to rule out IIHWOP.
The section ‘Comment’ of 7.1 of the IHS Classification only mentions ‘IIH most commonly occurs in young obese women. Although the majority of patients with IIH have papilledema, IIH without papilledema is observed. Other symptoms or signs of IIH include intracranial noises, tinnitus, transient visual obscurations and diplopia’ (1). We suggest additional guidelines for the screening of IIHWOP among chronic migraine patients should be included in the ‘comment’ text, inserting that not only intractable patients, but also first diagnosed patients with BMI > 30, should be screened.
Other mechanisms than CVT or BTSS may be causing elevated pressure in IIHWOP in CM patients; further studies are necessary to clarify this issue.