
Abstract
Background
Acupuncture has been used for the treatment of chronic migraine, but high-quality evidence is scarce. We aimed to evaluate acupuncture's efficacy and safety compared to topiramate for chronic migraine.
Methods
This double-dummy randomized controlled trial included participants aged 18–65 years diagnosed with chronic migraine. They were randomly assigned (1:1) to receive acupuncture (three sessions/week) plus topiramate placebo (acupuncture group) or topiramate (50–100 mg/day) plus sham acupuncture (topiramate group) over 12 weeks, with the primary outcome being the mean change in monthly migraine days during weeks 1–12.
Results
Of 123 screened patients, 60 (mean age 45.8, 81.7% female) were randomly assigned to acupuncture or topiramate groups. Acupuncture demonstrated significantly greater reductions in monthly migraine days than topiramate (weeks 1–12: −2.79 [95% CI: −4.65 to −0.94, p = 0.004]; weeks 13–24: −3.25 [95% CI: −5.57 to −0.92, p = 0.007]). No severe adverse events were reported.
Conclusions
Acupuncture may be safe and effective for treating chronic migraine. The efficacy of 12 weeks of acupuncture was sustained for 24 weeks and superior to that of topiramate. Acupuncture can be used as an optional preventive therapy for chronic migraine.
Trial registration
ISRCTN.org Identifier 13563102.
Introduction
Migraine, the second leading cause of global disability, is a prevalent neurological disorder characterized by recurring attacks causing significant pain (1). Chronic migraine, defined as headaches for 15 days per month for three months or more, with eight days per month having a history of migraine, shares features with and can transform from episodic migraine (2,3). The prevalence of chronic migraine in the general population is usually 1–2%, constituting approximately 8% of all migraine cases (4). Chronic migraine is associated with higher disability, increased comorbidity rates, medication overuse, and greater direct and indirect costs compared to episodic migraine (5). Furthermore, 22.7% of migraine patients stopped preventive medication due to inefficacy, while 59.1% discontinued it because of side effects (6).
Patients experiencing daily or near-daily chronic migraine attacks exhibit functional impairment and lower quality of life compared to those with less frequent migraine attacks. Expert opinion suggests that preventive treatment is advisable for individuals with migraine (7). Topiramate, onabotulinumtoxin A, and monoclonal antibodies targeting calcitonin gene-related peptide or its receptor antagonist have documented evidence-based efficacy for chronic migraine (3). Topiramate, endorsed by the American Headache Society, Scottish Intercollegiate Guidelines Network, French Headache Society, and Latin American consensus for chronic migraine treatment (8–10), faces limitations due to suboptimal efficacy and adverse events, leading to low adherence rates (11). Acupuncture is widely employed in China and Western countries for migraine management (12). Evidence indicated that acupuncture has better efficacy than sham acupuncture in treating episodic migraine, with an excellent safety profile (13,14). Yet, some studies found no significant difference in effectiveness between real and sham acupuncture (15,16). Acupuncture exhibits potential benefits for chronic migraine, but inconclusive results stem from limited research evidence. A systematic review suggests that acupuncture may be slightly more effective than preventive medication for people with migraine (17).
To date, only two open-label clinical trials have indicated that acupuncture may be more effective than standard medication for chronic migraine (18,19). However, drawing definitive conclusions from these trials is challenging due to their lack of a double-dummy design. Studies employing a double-dummy design can eliminate the placebo effect and offer more unbiased estimates of efficacy. Therefore, we conducted a double-dummy, single-blind, randomized controlled trial to compare the efficacy and safety of acupuncture and topiramate for chronic migraine.
Methods
Design
This single-center, double-dummy, active-control, randomized controlled trial was conducted in China. The protocol and statistical analysis plan are presented in Online Supplement 1. The design comprised a screening (3–14 days), a 4-week baseline, a 12-week treatment, and a 12-week follow-up period (Figure S1 of Online Supplement 2). This study was approved by the Research Ethical Committee of Beijing Hospital of Traditional Chinese Medicine, Capital Medical University (Reference 2017BL-045-01) and was conducted in accordance with Good Clinical Practice and the Declaration of Helsinki. Written informed consent was obtained from the participants before randomization.
Participants
Eligible participants, aged 18 to 65 years, had a history of migraine for at least one year before screening, with initial onset before 50 years of age. Chronic migraine diagnosis (at least 15 headache days and eight migraine days per month) was confirmed by a neurologistusing the International Classification of Headache Disorders 3 beta version (ICHD-3 beta) (Online Supplement 2, pages 6–8) (20). Participants were excluded if they had a history of cluster headache, other migraine subtypes including hemiplegic (sporadic or familial) migraine, and migraine with brainstem aura (basilar-type migraine), or chronic migraine with continuous pain; used migraine preventive medications and had experience with acupuncture or devices for chronic migraine within three months before screening; had clinically significant diseases; and were pregnant or lactating. Full inclusion and exclusion criteria are described in Online Supplement 2 (pages 3–5).
Patients receiving acute headache medications were included in the trial, as were those with a concurrent diagnosis of medication-overuse headache (MOH), which was confirmed during the screening period using the ICHD-3 beta criteria (Online Supplement 2, pages 7–8) (20). Other preventive medications were disallowed throughout the study.
Randomization and masking
After the baseline assessment, eligible participants were randomized 1:1 to receive acupuncture plus topiramate placebo (acupuncture group) or topiramate plus sham acupuncture (topiramate group) using an interactive web-based response system (Beijing LNKMED Tech Co., Ltd, Beijing, China). Randomization employed a computer-generated code with a constant block size of 4, stratified by MOH. The randomization sequence was generated by an independent statistician without further involvement. The participants, outcome assessors, and statistical analysts were blinded to the groups.
Intervention
Two experienced acupuncturists, each with over 20 years of clinical practice, administered 36 sessions (three sessions per week, every other weekday) of 30-min acupuncture treatments or medication over 12 weeks. Participants were treated individually in a single room to ensure privacy. Standardized instructions and procedures were formulated and adhered to, aiming to maintain consistency in rituals between two groups (Supplement 2, page 10).
Acupuncture prescriptions were based on classic and modern literature (21,22), consensus with clinical experts (23), and experience from our previous study (24). The obligatory acupoints selected were GV20, GV24, bilateral GB13, bilateral GB8, and bilateral GB20. Two adjunct points were used based on the syndrome differentiation of the meridians in the headache region. The potential acupoints included TE5, GB34, LI4, ST44, BL60, SI3, LR3 and GB40. Details of the acupoints are shown in Table S1 and Figure S2 of Online Supplement 2. Single-use needles (Hwato; Suzhou, China) with a length of 25 to 40 mm and a diameter of 0.25 to 0.30 mm, were used in the treatment. Twirling, lifting, and thrusting were performed to produce deqi (a sensation of soreness, numbness, distention, or heaviness that indicates effective needling). The patients also received a topiramate placebo titrated in the same manner as that in the topiramate group. The topiramate placebo (Xi’an Janssen Pharmaceutical, Xi’an, China) was identical to topiramate in appearance, smell, and taste.
In the topiramate group, sham acupuncture was administered on non-effective acupoints, without manual deqi manipulations. These acupoints, selected based on the clinical expertise of acupuncture professionals, extensive Chinese medicine references (21), and insights from previous study (24), encompassed bilateral LI15, PC3, GB35, LR7, and ST37 (Table S2 and Figure S2 of Supplement 2). Acupuncture and sham acupuncture details are outlined in Table S3 of Supplement 2. Topiramate, administered for 12 weeks, underwent a 4-week titration starting at 25 mg/day at bedtime, increasing weekly to either 100 mg/day or the maximum tolerated dose. By week 2, topiramate was evenly distributed twice daily. After the initial four weeks, a stable dose of at least 50 mg/day was maintained, as depicted in Figure S3 of Online Supplement 2.
Participants documented headache-related details using the headache diary (Online Supplement 1, pages 68–74). Recorded information encompassed headache characteristics, headache severity, headache onset, resolution and stop times, pain features, other migraine symptoms, and acute headache medication use. Patients were permitted neurologist-prescribed acute headache medications (Online Supplement 1, page 29). Consistency in the use of the same medication was mandated throughout the baseline and treatment periods, documented throughout the study.
Outcomes
The primary outcome was the mean change from baseline in monthly migraine days (MMDs) during weeks 1–12. A migraine day was defined as a calendar day with a headache lasting at least four consecutive hours, with features meeting the ICHD-3 beta criteria (with or without aura) or probable migraine (Online Supplement 2, pages 6–8), or a day wherein acute migraine-specific medication (triptans or ergot derivatives) was used.
Secondary outcomes encompassed proportions of participants with ≥50%, ≥ 75%, and 100% reduction in MMDs during weeks 1–12. Additional secondary outcomes covered mean changes from baseline in monthly headache days, acute medication use days, and headache hours during the same period, as defined in Online Supplement 2 (page 9). Other secondary outcomes included mean change from baseline in disability (6-item Headache Impact Test [HIT-6] (25) and Migraine Disability Assessment [MIDAS] (26)), quality of life (Migraine-Specific Quality of Life [MSQOL] (13)), and psychological profile (Beck Depression Inventory-II [BDI-II] (27) and State-Trait Anxiety Inventory-Trait [STAI-T] (28)) at week 12. These outcomes were assessed during weeks 13–24 or at week 24 as exploratory measures. The above scales have been translated into Chinese and validated.
Safety outcomes analyzed during the study included adverse events (AEs), abnormal laboratory tests, vital signs, weight, and electrocardiography (ECG). AEs attributed to the study were those persisting from the first treatment to the study’s end. A data monitoring committee oversaw safety data, addressing potential concerns throughout the trial.
Pre-treatment, the participants’ acupuncture expectations were assessed using an Acupuncture Expectancy Scale. Satisfaction was measured using the Patient Global Impression of Change Scale post-treatment. Blinding was assessed using the Bang Blinding Index (29). Acupuncture compliance was defined as receiving ≥29 sessions (≥80% compliance), while topiramate compliance was calculated as the percentage obtained by subtracting the total returned dose from the total dispensed dose, dividing it by the recommended dose, and multiplying by 100% (30). Study procedures and assessments are detailed in Table S4 of Online Supplement 2.
Statistical analyses
Based on a previous study (18), the reduced in MMDs after treatment were 10.5 ± 2.8 days in acupuncture group and 7.8 ± 3.6 days in topiramate group during weeks 1–12. With a sample size of 60 participants (30 per group), randomization was conducted with 80% power to detect group differences at an alpha level of 0.05, allowing for a 10% dropout rate.
Primary, secondary, and exploratory outcomes were analyzed using both intention-to-treat (ITT) and per-protocol (PP) sets. The ITT set included all randomly assigned participants, while the PP set comprised those meeting eligibility criteria, completing treatment and follow-up as planned, with no major protocol deviations. The safety set encompassed participants receiving at least one study treatment.
Withdrawals or patients with missing headache diary days (≥14 days) were prorated to 28 days for efficacy outcome calculation. For those with <14 days of data, efficacy outcomes were treated as missing before multiple imputation. Statistics were derived from 10 imputed data sets, with the mean representing the average mean and the standard error (SE) adjusted based on imputation variance estimates.
Baseline characteristics were summarized descriptively. The primary efficacy outcome was analyzed using a linear regression model adjusted for MOH and baseline MMDs. Least squares mean (LSM) changes from baseline with SE were presented for each treatment group, and treatment differences were expressed as LSM with a 95% confidence interval (95% CI). Continuous secondary and exploratory efficacy outcomes were analyzed akin to the primary outcome. Proportions of responders with ≥50%, ≥ 75%, and 100% reduction in MMDs were assessed using a logistic regression model adjusted for MOH. Mean percentages with SE and odds ratios (OR) with 95% CI were presented for these efficacy outcomes at both 12 and 24 weeks. AEs were summarized with counts and percentages. Changes in laboratory tests, vital signs, weight, and ECG data were described. We conducted a PP analysis as sensitivity analyses.
Blinding effectiveness was evaluated through participant perceptions using the χ² test and Bang Blinding Index, categorizing those who believed they received acupuncture plus placebo, sham acupuncture plus topiramate, or were uncertain about their treatment (29). All tests were two-sided with a significance level of 0.05. No adjustments were made for multiple comparisons. Statistical analyses were conducted using R statistical software (Version 4.0.3, R Core Team, Vienna, Austria).
Results
Participant characteristics
From 7 May 2018 to 7 December 2022, 123 patients were screened. Sixty-three were excluded, primarily due to not meeting inclusion criteria (Figure 1; Table S5 of Online Supplement 2). The remaining 60 patients (mean [SD] age, 45.8 [11.2] years; female [81.7%]) were randomly assigned to receive acupuncture or topiramate. Post-randomization, three patients (5.0%) dropped out (one in acupuncture, two in topiramate). Consequently, the ITT population comprised 60 patients, while 57 completed all periods in the PP population (Figure 1). Baseline characteristics were balanced between groups (Table 1; Table S6 of Online Supplement 2).
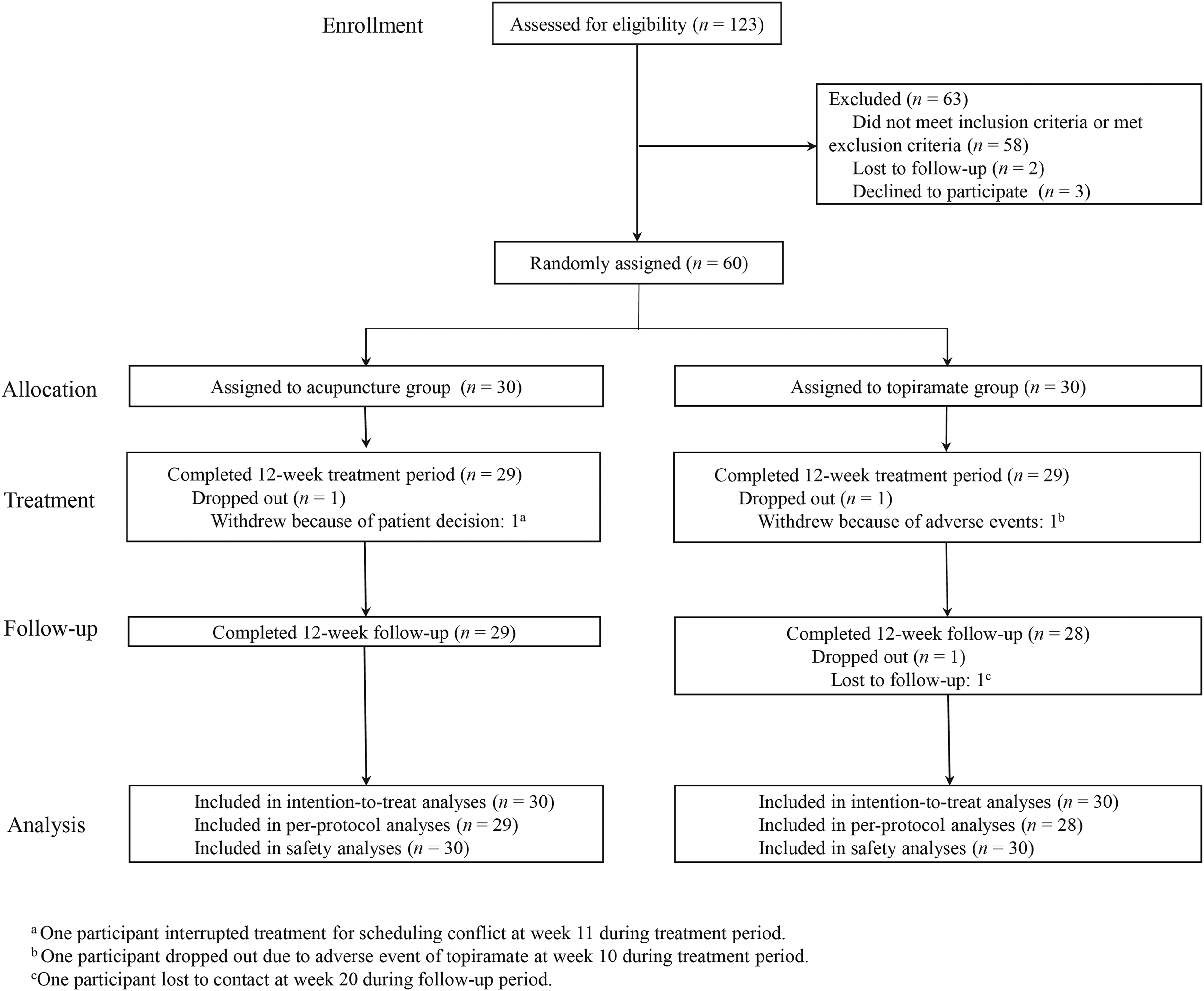
Screening, randomization, intervention, and follow-up of participants in the study.
Demographic and baseline clinical characteristics in the intention-to-treat population.
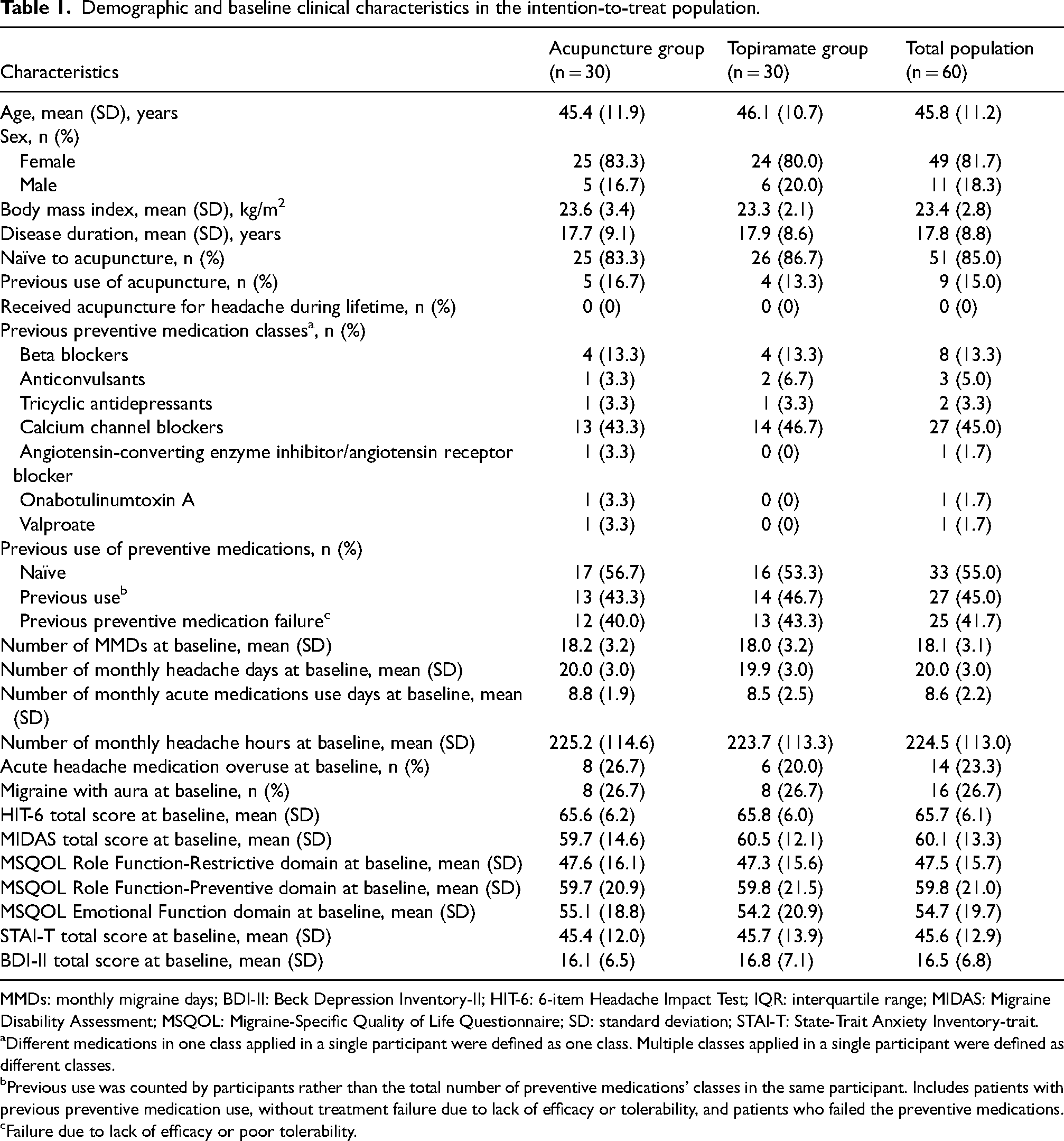
MMDs: monthly migraine days; BDI-II: Beck Depression Inventory-II; HIT-6: 6-item Headache Impact Test; IQR: interquartile range; MIDAS: Migraine Disability Assessment; MSQOL: Migraine-Specific Quality of Life Questionnaire; SD: standard deviation; STAI-T: State-Trait Anxiety Inventory-trait.
Different medications in one class applied in a single participant were defined as one class. Multiple classes applied in a single participant were defined as different classes.
Previous use was counted by participants rather than the total number of preventive medications’ classes in the same participant. Includes patients with previous preventive medication use, without treatment failure due to lack of efficacy or tolerability, and patients who failed the preventive medications.
Failure due to lack of efficacy or poor tolerability.
Efficacy analyses
Table 2 summarizes primary, secondary, and exploratory outcomes. Acupuncture, during weeks 1–12, significantly reduced mean MMDs compared to topiramate in the ITT set (LSM difference: −2.79 [95% CI: −4.65 to −0.94]; p = 0.004; Table 2 and Figure 2). Similar results were observed in the PP set (Table S7 of Online Supplement 2). The significant reduction in MMDs with acupuncture was sustained or further improved during weeks 13–24, showing greater reductions compared to topiramate (LSM difference: −3.25 [95% CI: −5.57 to −0.92]; p = 0.007).
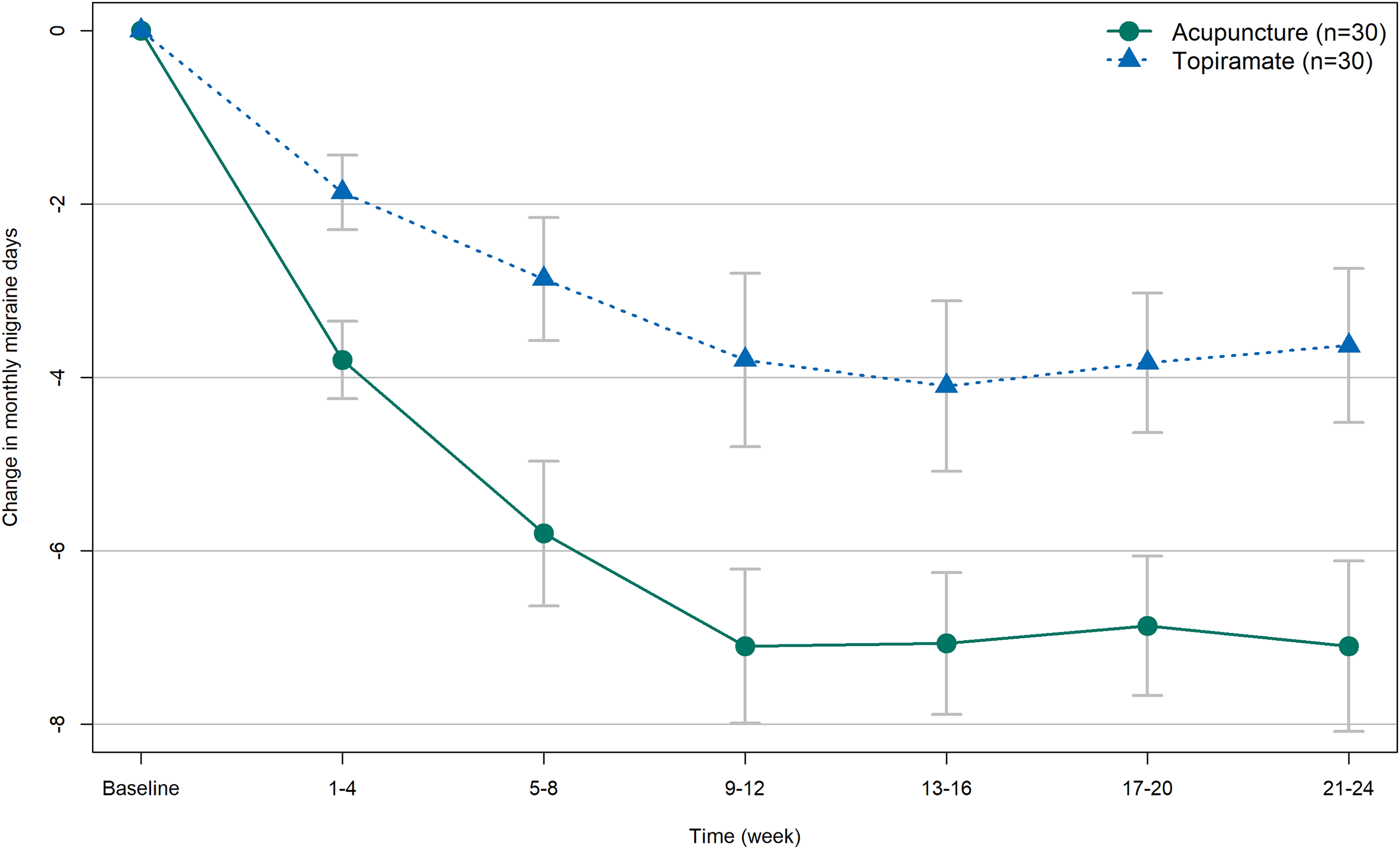
Change from baseline in monthly migraine days.
Primary, secondary and exploratory clinical efficacy outcomes during the treatment and follow-up periods in the intention-to-treat population.
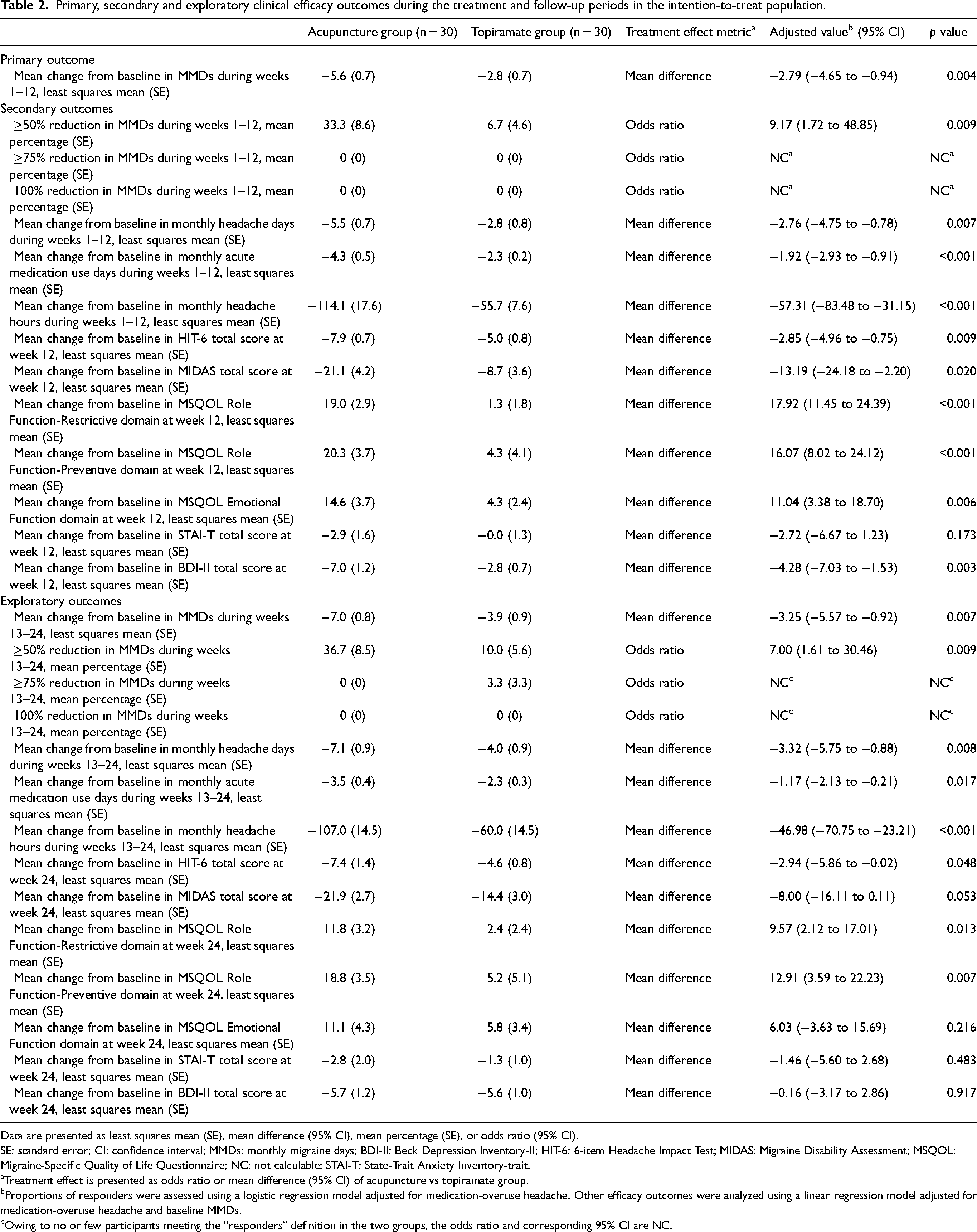
Data are presented as least squares mean (SE), mean difference (95% CI), mean percentage (SE), or odds ratio (95% CI).
SE: standard error; CI: confidence interval; MMDs: monthly migraine days; BDI-II: Beck Depression Inventory-II; HIT-6: 6-item Headache Impact Test; MIDAS: Migraine Disability Assessment; MSQOL: Migraine-Specific Quality of Life Questionnaire; NC: not calculable; STAI-T: State-Trait Anxiety Inventory-trait.
Treatment effect is presented as odds ratio or mean difference (95% Cl) of acupuncture vs topiramate group.
Proportions of responders were assessed using a logistic regression model adjusted for medication-overuse headache. Other efficacy outcomes were analyzed using a linear regression model adjusted for medication-overuse headache and baseline MMDs.
Owing to no or few participants meeting the “responders” definition in the two groups, the odds ratio and corresponding 95% CI are NC.
Acupuncture demonstrated significantly greater ≥50% reduction in MMDs than topiramate during weeks 1–12 (33.3% vs. 6.7%; OR, 9.17 [95% CI: 1.72 to 48.85]; p = 0.009; Table 2) and weeks 13–24 (36.7% vs. 10.0%; OR, 7.00 [95% CI: 1.61 to 30.46]; p = 0.009; Figure S4 of Online Supplement 2).
Acupuncture-treated patients showed greater reductions in monthly headache days, acute medication use days, and headache hours than topiramate-treated patients during both weeks 1–12 and 13–24 (Table 2).
Disability, assessed by HIT-6 scores, significantly improved at weeks 12 and 24, with greater total improvements seen in acupuncture than topiramate (Table 2). Acupuncture also exhibited higher reductions in MIDAS scores at week 12. In terms of quality of life, acupuncture showed greater improvements in all three MSQOL domains compared to topiramate at weeks 12 and 24, except for the MSQOL Emotional Function domain at week 24. While BDI-II scores favored acupuncture at week 12, no significant differences were observed at week 24. There were no significant differences in STAI-T scores between the groups at weeks 12 and 24.
Acupuncture yielded higher participant satisfaction than topiramate at week 12 (Table S8 of Online Supplement 2). Blinding effectiveness was evidenced by no differences in responses between treatment groups, and the Bang Blinding Index indicated successful blinding (Table S9 of Online Supplement 2). No baseline differences were observed in participants’ expectations of acupuncture (Table S10 of Online Supplement 2). Treatment compliance showed higher topiramate compliance in the acupuncture group compared to the topiramate group, with no significant difference in acupuncture compliance between the two groups (Table S11 of Online Supplement 2).
Safety analyses
Acupuncture group reported fewer AEs (10.0%) than the topiramate group (26.7%), with clinically significant differences (p < 0.001; Table 3). In the acupuncture group, two AEs were acupuncture-related (subcutaneous hematoma, numbness), and one was topiramate placebo-related (dyspepsia). No patients dropped out due to AEs related to acupuncture. The topiramate group had seven AEs related to topiramate side effects (paresthesia, dizziness, attention difficulty, fatigue, nausea). One participant reported acupuncture-related AEs (needling pain after treatment). One patient dropped out due to topiramate-related AEs. However, all events were mild, self-limiting, and required no special medical interventions. No serious AEs were reported in either group.
Adverse events related to treatment.a
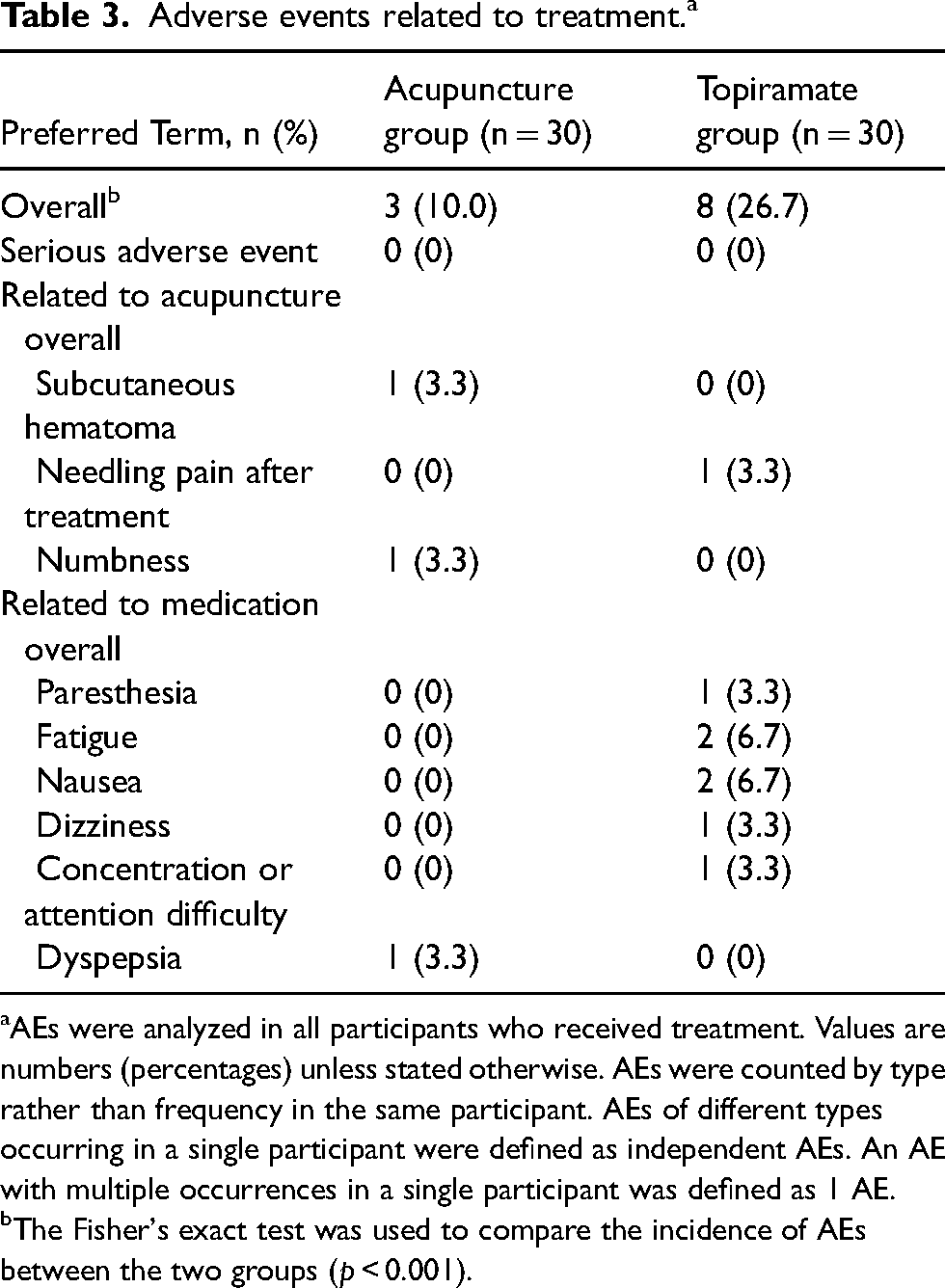
AEs were analyzed in all participants who received treatment. Values are numbers (percentages) unless stated otherwise. AEs were counted by type rather than frequency in the same participant. AEs of different types occurring in a single participant were defined as independent AEs. An AE with multiple occurrences in a single participant was defined as 1 AE.
The Fisher's exact test was used to compare the incidence of AEs between the two groups (p < 0.001).
Mean changes from baseline in laboratory test, vital signs, body weight, and ECG were small and similar between the treatment groups, without clinically relevant findings (Tables S12–S14 of Online Supplement 2).
Discussion
In this single-center, single-blind, double-dummy, active-control, randomized controlled trial, acupuncture showed greater efficacy than topiramate in the mean change from baseline in MMDs during weeks 1–12. A positive response was evident within the first four weeks, persisting for 12 weeks post-treatment, indicating an early and sustained preventive effect. The efficacy was also accompanied by clinically significant improvements in disability and quality of life, as shown by greater enhancement in HIT-6, MIDAS, and MSQOL total scores after acupuncture treatment than that after topiramate treatment. Acupuncture had significantly fewer AEs than topiramate in the 12-week treatment period. Given topiramate's high AE rates, frequent drug discontinuations, and poor tolerance, acupuncture offers a safety advantage in clinical practice.
Comparison with other studies
Topiramate is widely recommended in guidelines for the preventive treatment of chronic migraine (10,13,20), demonstrating proven efficacy. In this study, the change from baseline in MMDs with topiramate (2.8 days) aligns with previous trial results (2.3 to 3.5 days) (31,32). For topiramate, the 50% response rate in this study was lower than that in two other placebo-controlled trials (32,33). The lower response rate of topiramate in this study may attributed to the fact that 43.3% of patients in the topiramate group had a history of failure in preventive medication treatment, while previous studies showed no history of preventive medication failure. In the topiramate group, 26.7% reported AEs, falling within the 15.0–75.0% range reported in the general population (32,34). This broad migraine population, with an average disease duration of around 18 years, included nearly 55.0% who had not previously received preventive medications (Table S15 of Online Supplement 2), highlighting undertreatment and underprescribing issues in migraine care, possibly reflecting the healthcare situation in China (35). Many people with migraine are unwilling to start prophylactic treatment because of poor tolerability of preventive medications (11). For migraine patients, most of whom are female and young to middle-aged, topiramate's cognitive and psychological adverse effects (3) can lead to diminished ability of occupational activities. This trial showed that acupuncture significantly improved patient acceptance compared to topiramate, addressing the need for a well-tolerated migraine treatment with effective clinical outcomes.
Acupuncture, extensively employed for migraine prevention, resulted in a mean change of 5.6 days in MMDs from baseline in our trial. Our trial's result aligns with studies on acupuncture versus placebo for episodic migraine, where the change from baseline in MMDs was 3.5 days in acupuncture groups (13,14). Several head-to-head trials have compared acupuncture with standard medication for episodic migraine (34,36), and one of our randomized controlled trials showed that acupuncture was more effective than flunarizine in decreasing the number of days of migraine attacks (24). While acupuncture is increasingly utilized for preventing episodic migraine, its application for chronic migraine is less common. In our trial, the acupuncture group showed a 2.79-day reduction in MMDs compared to the topiramate group over 12 weeks, aligning with findings from two open-label acupuncture versus medication studies (differences in MMDs: 2.9 days and 2.8 days, respectively) (18,19). The National Institute for Health and Clinical Excellence clinical guidelines propose a minimally important difference (MID) of 0.5 days for monthly migraine/headache days change (37). In our study, the between-group differences exceeded MID, with reductions of 2.79 days during treatment and 3.25 days in the follow-up period, signifying a sustained therapeutic effect and clinically meaningful differences between acupuncture and topiramate.
Strengths and limitations of this study
This trial's double-dummy design, distinguishing it from head-to-head trials without sham controls, minimizes the placebo effect and enhances participant compliance. The 24-week assessment provides insights into acupuncture's long-term efficacy, crucial for successful prophylaxis and reducing migraine recurrence. Additionally, the trial includes multidimensional evaluations of disability, quality of life, and psychological profiles in patients with chronic migraine. Nevertheless, this study has several limitations. This single-center trial's external validity is limited, as it lacks the diverse participant access of multicenter studies. However, single-center trials offer easier quality control and better internal authenticity compared to multicenter trials. Second, the study's sample size is relatively small. However, it was estimated based on a previous study, and our results indicate a statistical power close to 100%. Third, the current patient population in this study consists of approximately 40% of migraine patients with a history of preventive medication failure. This inclusion may potentially restrict the generalizability of our findings. Thus far, there is limited data available to inform evidence-based acupuncture treatment decisions for patients who have experienced unsuccessful prior treatments. Fourth, sham acupuncture may introduce unpredictable physiological effects and patient-acupuncturist interactions, potentially amplifying the non-specific effect compared to a medicine placebo (38). The use of sham acupuncture might have increased efficacy in the topiramate group, minimizing the difference between groups (39), and thus conserving the efficacy of acupuncture in our study. Fifth, due to the nature of acupuncture, blinding acupuncturists is not feasible. However, the study's primary outcome relied on participants’ self-evaluation, mitigating bias introduced by unmasked acupuncturists to some extent. Sixth, real acupuncture was performed at head acupoints, while in the topiramate group, acupuncture was performed at non-effective acupoints on the limbs which were ineffective for treating headache. Nonetheless, sham acupuncture was applied at non-effective points to minimize physiological effects and prevent segmental analgesia in the topiramate group. Finally, topiramate is effective in chronic migraine patients with MOH (32). Due to the low proportion of chronic migraine patients with MOH in this study, it remains unclear if acupuncture is more effective than topiramate for this subgroup. Further research is needed.
Clinical relevance
Chronic migraine, a disabling disorder, substantially impairs patients’ quality of life and daily functioning (3), correlating with heightened resource utilization—more healthcare provider visits, emergency department visits, and diagnostic testing (5). Treatment guidelines from the American Headache Society indicate only a handful of oral migraine preventive medications with robust clinical evidence of efficacy (40). Adherence to preventive medication among patients with chronic migraine is 26–29% at six months (41), which might be due to the number of patients who do not respond well to drug treatment or cannot tolerate the adverse effects of drugs. Some patients, including those with contraindications or aversions to medications, and specific populations like pediatric, pregnant, and older individuals with chronic migraine, may find acupuncture preferable. Moreover, acupuncture, less prone to MOH, offers individualized treatment plans. Our study reached beyond the gold-standard design for efficacy analysis in single-blind, placebo acupuncture-controlled trials by conveying the real-world situation. It currently represents the best approximation of clinical practice under our study setting. However, previous studies found no significant difference in effectiveness between real and sham acupuncture (15,16). Sham acupuncture may generate a notable placebo effect, particularly when subjective indicators as outcomes. To counteract the placebo effect, our study used a double-dummy design for a more realistic assessment of difference of treatment effect between acupuncture and topiramate. The topiramate group's efficacy may result from both topiramate and the placebo effect of sham acupuncture, enhancing the overall therapeutic impact and reducing group differences. To date, the National institute for health and clinical excellence clinical guideline recommended two sessions a week for acupuncture treatment in episodic migraine in Europe (37). Our intensive regimen (three session a week) and personalized acupoint protocols based on Traditional Chinese Medicine patterns highlight the need for cross-cultural studies that evaluate the cost-effectiveness and feasibility of using acupuncture to treat chronic migraine.
Conclusions
This study showed that acupuncture is safer and more effective than topiramate in treating chronic migraine. Acupuncture exhibited robust efficacy, significantly reducing MMDs, improving disability, and enhancing quality of life, with a sustained beneficial effect throughout follow-up. Acupuncture emerges as a valuable alternative for chronic migraine patients, particularly those with medication contraindications, intolerance, preferences against medications, and specific populations like pregnant women and adolescents.
Clinical implications
In this long-term clinical trial, acupuncture is safe and more efficient than topiramate in the treatment of patients with chronic migraine throughout the 24 weeks treatment and follow-up periods.
The efficacy of 12 weeks of acupuncture may be superior to that of preventive medication for chronic migraine in improving migraine-related disability and quality of life.
The sustained improvements in patient-reported outcomes further support the beneficial effects of long-term use of acupuncture as a preventive treatment for migraine.
Supplemental Material
sj-docx-1-cep-10.1177_03331024241261080 - Supplemental material for Acupuncture plus topiramate placebo versus topiramate plus sham acupuncture for the preventive treatment of chronic migraine: A single-blind, double-dummy, randomized controlled trial
Supplemental material, sj-docx-1-cep-10.1177_03331024241261080 for Acupuncture plus topiramate placebo versus topiramate plus sham acupuncture for the preventive treatment of chronic migraine: A single-blind, double-dummy, randomized controlled trial by Lu Liu, Qiuyi Chen, Luopeng Zhao, Tianli Lyu, Limin Nie, Quan Miao, Yuhan Liu, Libin Zheng, Feiyu Fu, Yuxi Luo, Chenxi Zeng, Chengcheng Zhang, Peiyue Peng, Yixin Zhang, and Bin Li in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024241261080 - Supplemental material for Acupuncture plus topiramate placebo versus topiramate plus sham acupuncture for the preventive treatment of chronic migraine: A single-blind, double-dummy, randomized controlled trial
Supplemental material, sj-docx-2-cep-10.1177_03331024241261080 for Acupuncture plus topiramate placebo versus topiramate plus sham acupuncture for the preventive treatment of chronic migraine: A single-blind, double-dummy, randomized controlled trial by Lu Liu, Qiuyi Chen, Luopeng Zhao, Tianli Lyu, Limin Nie, Quan Miao, Yuhan Liu, Libin Zheng, Feiyu Fu, Yuxi Luo, Chenxi Zeng, Chengcheng Zhang, Peiyue Peng, Yixin Zhang, and Bin Li in Cephalalgia
Footnotes
Acknowledgments
We thank Hang Shen (Peking Union Medical College Hospital), and Lin Zeng (Peking University Third Hospital) for statistical analysis guidance. We also thank the research assistants, neurologist, acupuncturists, members of steering committee, executive committee, and data monitoring committee, and all of the patients who participated in this study.
Author contributions
BL conceived and designed the study. BL, LL and QC had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. LL and QC drafted the manuscript. BL, LL, QC, LZ, TL, LN, QM and YL contributed to the acquisition, analysis, and interpretation of data. TL did the statistical analysis. BL and LL obtained funding. BL, LBZ, FF, YXL, CZ, CCZ, PP, and YZ provided administrative, technical, or material support. BL supervised the study and is the guarantor. All authors provided final approval of the manuscript content for submission and had final responsibility for the decision to submit for publication.
Data availability
Anonymized individual clinical data will be made available upon request from the corresponding author (libin@bjzhongyi.com) for research (non-commercial) purposes to individuals affiliated with academic or public health institutions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Municipal Science and Technology Commission, National Natural Science Foundation of China, Beijing Municipal Natural Science Foundation, Outstanding Young Talents Program of Capital Medial University, Beijing Municipal Commission of Education, China Association for Science and Technology, (grant number Z171100001017033, 82074179, 82374575, 7232270, B2207, KM202110025005, 2019-2021ZGZJXH-QNRC001).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.