
Abstract
A multicentre, randomized clinical trial was undertaken to test the hypothesis that acupuncture is more efficacious than sham control procedure in the prevention of episodic tension-type headache. Fifty subjects were randomized to receive a course of treatment with either brief acupuncture or a sham procedure. Subjects were followed up for 3 months. Changes in headache were assessed by daily diary, the primary outcome measure being the number of days with headache. No significant differences were found between the changes in the two groups for any measure at any time point. Results also show that patient blinding was successful. In conclusion, this study does not provide evidence that this form of acupuncture is effective in the prevention of episodic tension-type headache.
Introduction
Episodic tension-type headache (ETTH) is essentially defined as a bilateral headache of pressing or tightening quality without a known medical cause, which does not occur more than 15 days out of every month (more frequent headaches of similar type are called chronic tension-type headache) (1). Additional features are that it is of mild to moderate severity and may inhibit activities but does not prevent them. A large telephone survey of a western population found the annual incidence of ETTH to be 38% (2). It is more common in women than in men (sex ratio 1.2:1), it peaks in the age range 30–39 years, and has a higher incidence with increasing levels of education. A total of 8% of subjects with ETTH report lost workdays due to their headache, averaging at about 9 days per year, and 44% believed that their work effectiveness was reduced on about 5 days per year because of headache. Other surveys indicate problems of similar scale in other western populations (3, 4).
No individual therapy has been shown to be universally effective for ETTH. Some authors have explored the role of psychological factors such as personality, mood and behavioural disorder, but the findings are not consistent enough to inform clinical practice (5).
Patients who suffer from stress-related problems such as ETTH frequently seek help from acupuncture. Headaches and emotional problems were found to be responsible for 15% of consultations with acupuncturists (6). Previous randomized controlled trials of the effectiveness of acupuncture for ETTH have produced contradictory results (7–9). Two recent systematic reviews conclude that the evidence is inconclusive and recommend well-planned studies to assess the effectiveness of acupuncture for ETTH (10, 11). We therefore undertook a multicentre, randomized clinical trial to determine whether a particular form of acupuncture is more effective than sham procedure for the prevention of ETTH.
Methods
After a pilot study to develop and validate a new sham procedure (12), a multicentre study with two parallel arms was co-ordinated by the Department of Complementary Medicine at the University of Exeter. Acupuncturists were recruited from the accredited members of the British Medical Acupuncture Society.
Participants
Adults of either sex were recruited either during consultation, from disease registers, from notices in premises of participating practices or via local media. Subjects were included if they were diagnosed with ETTH according to the accepted definition (1), gave fully informed signed consent and agreed to use only one named analgesic, when required, for the duration of the trial. Subjects were excluded if their headache occurred less than once a week, if they took regular prophylactic medication for headache, if they had previously undergone acupuncture for any condition, if they had a history of severe bleeding diathesis or if they were pregnant. The study was approved by the Local Research Ethics Committee for each centre.
On the initial visit, subjects provided baseline demographic information and completed a purpose-designed headache history questionnaire and the 12-item form of the General Health Questionnaire (GHQ) (13). They then maintained a daily headache diary (see below) for the 3-week run-in period before the intervention.
Randomization
Centralized random allocation by telephone was performed immediately before the first treatment. Randomization lists (block-size of four) were stratified for each centre, prepared from computer-generated random numbers by staff unconnected with the study, and held at a Hospital Pharmacy.
Interventions
Brief acupuncture treatment was given to Group A using one 30 × 0.30 mm needle (AcuMedic), at four obligatory points (GB20 in the suboccipital region or a nearby tender spot and LI4 in the hand, bilaterally) and up to four optional points in head, neck or shoulders, which had to be chosen by the practitioner according to tenderness and the patient's symptoms. Points were treated in succession with a single needle. After insertion, the needle was manipulated for 15 s or until deQi was felt if that was sooner. The needle was then removed and the next point treated. This method is similar to that used in previous studies (9, 14, 15), but without needle retention. It is taught to many doctors learning acupuncture in the UK. The location of optional points used and the strength and duration of stimulation could be modified in subsequent sessions according to the patient's response.
Subjects in Group B received sham treatment by tapping a blunted cocktail-stick in a guide tube against bony prominences in four standard areas (two selected from the occipital protuberances, spines of scapula, vertex of skull and spinous process of 6th cervical vertebra, and two areas at the middle of 2nd metacarpal bone of each hand) and one area chosen individually for that patient. Areas that were avoided in Group B were the site of the pain, tender areas and known acupuncture points. Gentle pressure was applied at each point while rotating the cocktail stick for 15 s, before moving to the next point in sequence. The pilot study had shown that acupuncture-naive patients could not identify this procedure as a sham when performed by a single practitioner. Subsequently, if the subject had not responded, acupuncturists were free to add further sham points to mimic real management.
A course of genuine or sham treatment was given weekly for 6 weeks, with two follow-up treatments after 1 and 2 months.
Blinding and standardized interaction
The nursing assistant interviewed the subjects in a separate room and remained unaware of their group allocation. Subjects were asked to show headache diaries to the nurse but not to the acupuncturist. The consultation with the physician acupuncturist was standardized in terms of examination, treatment, and permitted discussion. Thus, the acupuncturist examined all patients similarly for tenderness of neck and shoulders, and after either procedure made an ambiguous statement such as ‘The needles are all out and there is no bleeding’. Discussion with the acupuncturist about acupuncture was not permitted, and discussion about headache was limited to a simple statement of the beneficial or adverse response to the previous treatment.
The success of subject blinding was tested with the question: ‘When you volunteered for the trial, you were informed that you had an equal chance of receiving acupuncture or another similar form of treatment. Do you believe you were in the group that received acupuncture?’. Possible responses were Yes, No or Don't know. This question was posed after the second and sixth treatments. Subjects immediately placed the paper on which they had written the answer in an envelope preaddressed to the co-ordinating centre, in order to maintain blinding of the nurse.
The investigators did not have access to the randomization code until all data had been entered.
Outcome measures
Subjects were asked to complete a daily headache diary in which they recorded the number, duration and severity of any headaches, and the number of analgesics consumed. Severity was measured by asking subjects to rate their headache on a visual analogue scale (VAS) of 100 mm length marked ‘none’ and ‘worst imaginable’ at the two ends. The diary continued for the 3-week run-in period, the 5-week treatment period, 3 weeks early follow up immediately after treatment, and for a further 3-week period starting 3 months after the end of the initial course of treatment. The primary outcome measure was defined before the analysis as the number of days with headache in each week, as recommended in the literature (16). The GHQ was completed at baseline and immediately after the sixth treatment. Two items from the Short-Form 36 quality of life questionnaire were used at baseline and after the sixth treatment to assess the headache's impact on social activities and work during the previous 4 weeks. Global assessment of change was recorded at the end of treatment and at 3 months follow up, by selecting one option from a list (headaches got worse/stayed the same/got slightly better/got much better/disappeared).
Sample size
The sample size was calculated on the basis of pilot data on headache intensity. Mean intensity before treatment on the VAS was 40,
Analysis
The data were analysed in four periods of 3 weeks (run-in, last 3 weeks of treatment, early follow up, late follow up). The primary analysis consisted of comparing the changes in number of days with headache from run-in to early follow-up periods in the two groups (16). The analysis was by intention to treat, with missing data substituted by carrying forward the last recorded value (i.e. last available 3 week mean, or last available weekly score for graph of weekly headache scores). The majority of the data were not normally distributed, therefore analyses were performed using non-parametric tests, i.e. Mann–Whitney U-test for independent samples, the Wilcoxon signed rank test for paired samples. Fisher's exact test was used for dichotomous data. The null hypothesis was rejected when P < 0.05.
Results
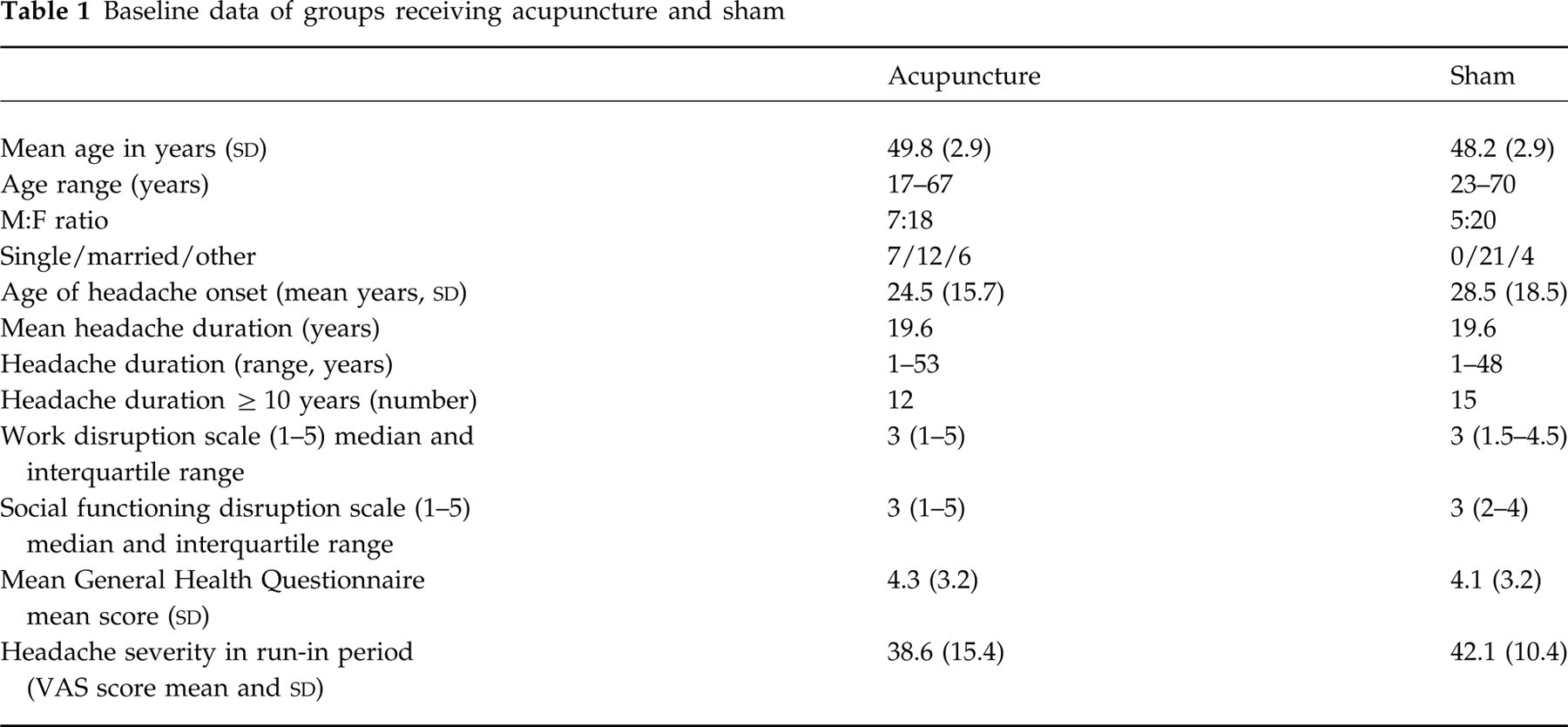
Five centres participated in the trial, involving four primary care practitioners and the first author, a University researcher. A total of 50 subjects was randomized into acupuncture and sham groups, their progress being illustrated in Fig. 1. One subject (sham group) dropped out at the end of the early follow up because of lack of response; one subject (acupuncture group) dropped out at the end of the early follow up as she had started a course of spinal manipulation for her headache. The remaining subjects missed their appointments and did not reply to reminders. No meaningful differences were identified in the prognostic features of the two groups at baseline (Table 1).

Flow chart showing numbers of subjects at each stage of a controlled trial of acupuncture for tension headache.
Baseline data of groups receiving acupuncture and sham
The following adverse events were reported: two cases of severe exacerbation of headache (one acupuncture, one sham group), four cases of bruising and one of post-needling pain (all acupuncture group).
In assessing the credibility of the interventions immediately after the second intervention, six subjects believed they had not had real acupuncture (two in the acupuncture group, four in the sham group) and 16 subjects were uncertain (five acupuncture, nine sham). At the end of treatment, five subjects believed they had not had real acupuncture, 13 were uncertain. These results did not differ significantly between the groups.
The outcomes obtained from the daily diaries are summarized in Table 2. Considering the number of days with headache, there was no significant difference between the groups in the changes from the run-in period to early follow-up period (P = 0.689, Mann–Whitney). For both groups together, the reduction in number of days with headache from the run-in period to all other periods was highly significant (P < 0.001, Wilcoxon); weekly mean scores for the two groups, with 95% confidence intervals (CI), are shown in Fig. 2. There was no significant difference between the groups for numbers responding with a 50% fall in headache days (Table 3).
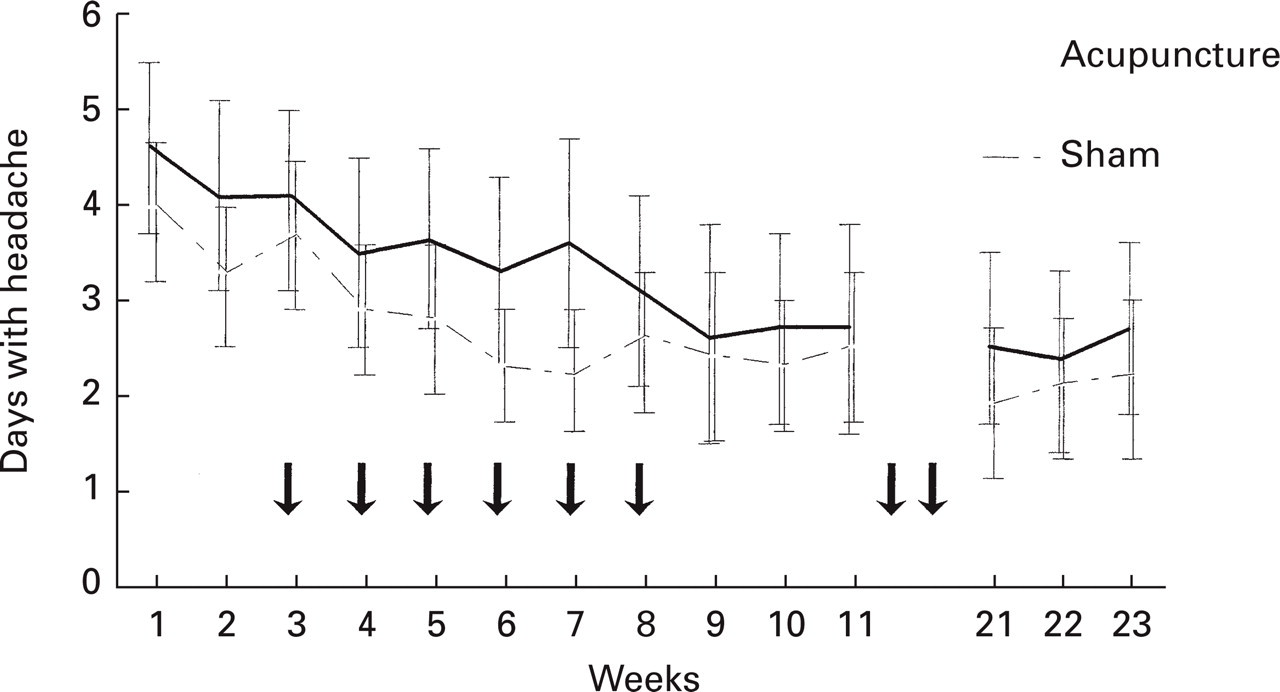
Mean days with headache (and 95% confidence intervals) during each week. Subjects received acupuncture or sham at times indicated by the arrows.
Outcomes of acupuncture and sham treatment for episodic tension headache, in 3-week observation periods
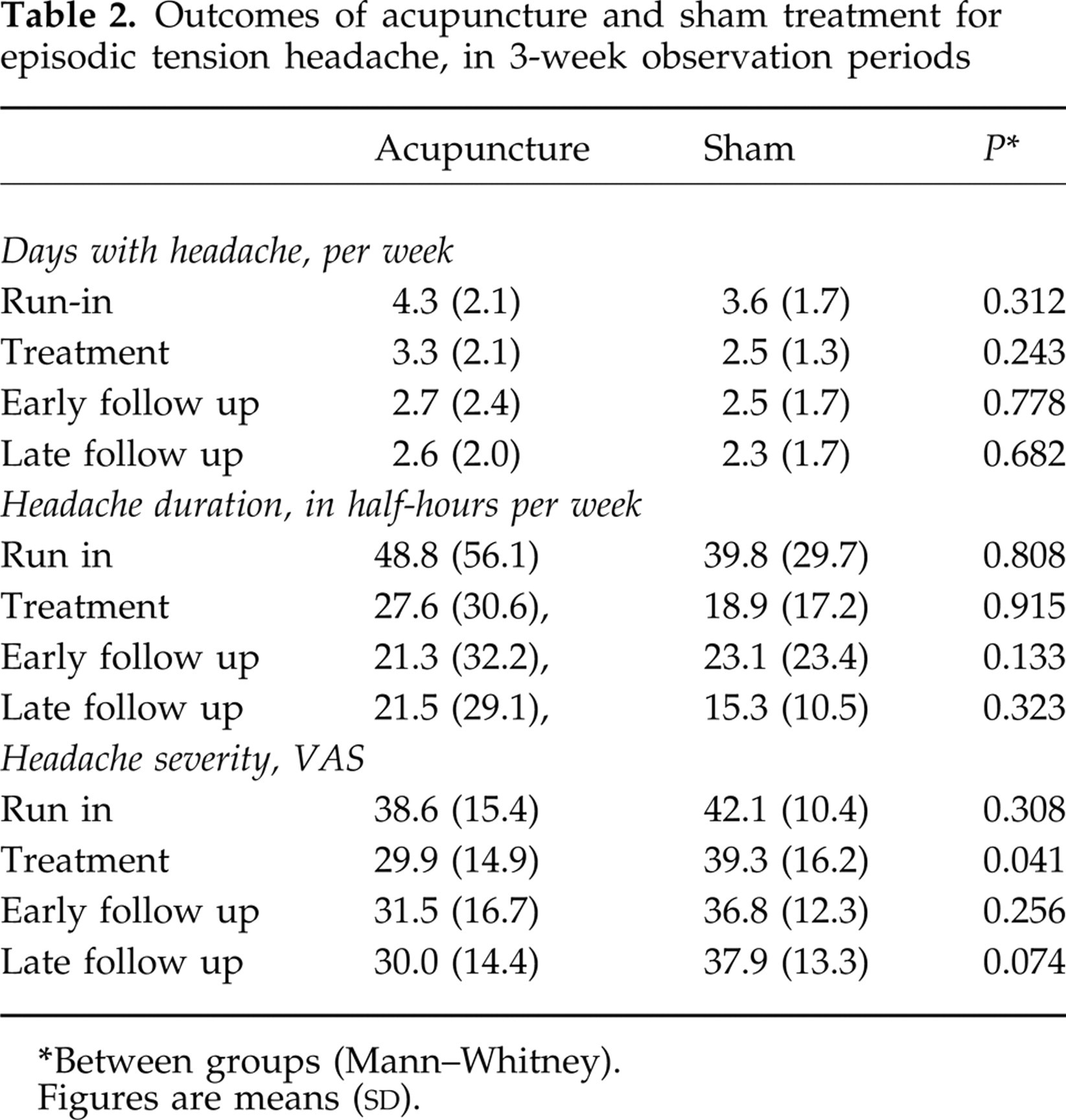
Between groups (Mann–Whitney).
Figures are means (
Number in each group with ≥ 50% reduction in headache days

Between groups (Fisher's exact test).
There were no significant differences between the groups for numbers responding (as determined by a 50% fall in headache duration), for headache severity or for number of tablets used, with one exception: the acupuncture group scored significantly lower severity of headache during the treatment period only. However, this difference was not confirmed when the changes between run-in and treatment period were compared (P = 0.322, Mann–Whitney). Scores for impact of headache on work and social functioning, together with the GHQ scores, improved from baseline to end of treatment but again there were no differences between the groups. The numbers of subjects who indicated that they had improved (slightly or much better) on the global assessment scale after treatment was not significantly different between groups (18/21 and 20/23 at end of treatment; 12/14 and 13/16 at late follow up, for acupuncture and sham groups, respectively). Thirteen subjects rated themselves as much better at the late follow up (acupuncture group five, sham group eight), and one participant in each group reported that their headache had disappeared.
Discussion
The results of this multicentre study of brief acupuncture for episodic tension headache show no difference between genuine and sham treatment for any of the outcome variables. Subjects in both groups experienced a significant reduction of symptoms during the course of the study, amounting to more than one headache day a week. Thirty percent of subjects reported themselves as much better or totally relieved of headache.
It is not possible to state whether this represents a response to the interventions or other factors. Several subjects who met the inclusion criteria for ETTH, including < 15 days with headaches per month, recorded more than two headaches per week during the run-in period. Their symptoms seem to have been worse than usual at the time of enrolment, in which case the changes shown would be due to regression to the mean. Alternatively, this may represent either the tendency to answer questions in a way that secures inclusion in a study, or the tendency of observation alone to produce measurable effects (Hawthorne effect). It is also possible that this improvement represents a genuine response which was similar after both forms of intervention. Acupuncture may produce effects by stimulation of A delta fibres in skin and muscle resulting in release of neurotransmitters (17), and stimulation by cocktail stick over bony prominences could produce a similar effect.
Limitations of the study
Recruitment of subjects was difficult; many patients who were approached met the exclusion criteria, for example having a mixed picture of headache, and in many cases patients had already been given acupuncture for headache or another condition. Some potential subjects did not wish to commit themselves to keeping the diary. As a result, the estimated sample size was not achieved. However, it appears unlikely that the result would have been different with larger numbers, judging both from the CIs of Fig. 2 and from the lack of positive trends in any of the outcome measures.
A multicentre study presents limitations that are not seen in single-centre studies. For instance, it did not prove feasible to check the application of the protocol in all centres. However, the results were consistent across centres and appear homogeneous.
Relationship to other studies
Two studies of acupuncture for tension headache (7, 9), involving a total of 39 subjects, were included in a recent meta-analysis (10). Combining the scores for numbers of subjects responding in treatment or sham control groups gave a responder rate ratio of 1.49 (95% CI 0.96–2.30), where unity indicates no net effect. The present study is similar enough to be added to the calculation. This increases the total number of subjects to 89 and reduces the responder rate ratio to 1.36 (CI 0.93–2.00). The two earlier studies used different acupuncture techniques from the present study, involving up to 10 needles placed in traditional points (not chosen for tenderness) for at least 15 min. It is problematic to draw conclusions from small numbers, but it remains possible that the brief form of needling used in the present study is less effective for ETTH than prolonged needling techniques.
Implications
Although brief needling is a technique used in traditional Chinese acupuncture, it has been applied in the west without being associated with traditional theories (18). Clinically, it appears particularly useful for treating myofascial trigger points (19), and it was used in this study on the grounds that tension headaches are symptoms of myofascial trigger point activity. Brief needling was used for mixed headache in an earlier study (20) in which it proved superior to medication. The present negative result is consistent with several implications. First, the form of treatment used here was inadequate to produce sustained inactivation of trigger points. Second, factors other than myofascial trigger points may be important in producing ETTH in this group of subjects (21). Third, acupuncture only has non-specific effects for ETTH, including the expectations of patients and doctors or the relaxing effect of lying down for 15 min.
In conclusion, brief acupuncture was not found to be superior to a credible sham intervention in the prevention of episodic tension-type headache.
Footnotes
Acknowledgements
Funding for the study was provided by the United Kingdom's NHS Executive South-west R & D. The authors gratefully acknowledge the indispensable help of the following nursing staff: Trudi Faulkner, Pauline Godfrey, Lorna Lutley, Karen O'Neill, Anne Rowland and Freda Williams.