
Abstract
Background
Zavegepant is the first small molecule calcitonin gene-related peptide receptor antagonist for intranasal administration for the acute treatment of migraine. The objective of this study was to evaluate the safety and tolerability of zavegepant in the acute treatment of migraine under repeated, as-needed dosing for up to one year.
Methods
This phase 2/3, one-year open-label safety study of zavegepant 10 mg nasal spray for the acute treatment of migraine enrolled adults aged ≥18 years with a history of two to eight moderate to severe monthly migraine attacks. Participants used one dose of zavegepant as needed to self-treat migraine attacks of any severity, up to eight times per month, for 52 weeks.
Results
Participants were enrolled between 29 June and 4 December 2020. Of the 608 participants entering long-term treatment, 603 were treated with study drug. Participants administered a mean (SD) of 3.1 (1.55) zavegepant doses per month. There were no deaths. Of the seven serious adverse events reported, none was considered related to treatment. Altogether, 6.8% (41/603) of treated participants had an adverse event leading to study drug discontinuation. The most frequent adverse event leading to discontinuation was dysgeusia (1.5% [9/603]). The most common treatment-emergent adverse events (≥5% of participants) were dysgeusia (39.1% [236/603]); nasal discomfort (10.3% [62/603]); COVID-19 (7.5% [45/603]); nausea (6.1% [37/603]); nasal congestion and throat irritation (5.5% [33/603] each); and back pain (5.3% [32/603]). Aminotransferases >3x the upper limit of normal occurred in 2.6% [16/603] of participants; none had concurrent elevations in bilirubin >2x upper limit of normal.
Conclusions
One year of zavegepant 10 mg nasal spray up to eight times per month was safe and well tolerated.
Introduction
Guidelines recommend nonoral therapies for the acute treatment of migraine when attacks are associated with severe nausea or vomiting, characterized by rapidly escalating headache pain, or when orally administered medications take too long to relieve symptoms, are not consistently effective, or cause tolerability issues (1–3). Although parenteral drugs can be useful, many patients with migraine would rather use a nasal spray (4,5). In practice, this limits the pharmacotherapeutic options with regulatory approval for migraine to sumatriptan, zolmitriptan, and dihydroergotamine mesylate. However, triptans are ineffective in up to one-third of attacks (6), and cardiovascular contraindications restrict their use in approximately 3.5 million people with migraine in the United States (US) population (7,8). Dihydroergotamine nasal spray is less effective than sumatriptan nasal spray at early time points (9,10), it has cardiovascular contraindications similar to the triptans, and should not be administered with potent cytochrome P450 3A4 inhibitors (11). While all of these intranasal treatments have a place in the acute treatment of migraine, additional options other than triptans and dihydroergotamine have the potential to address these unmet needs. Zavegepant is the first intranasally administered small molecule calcitonin gene-related peptide (CGRP) receptor antagonist for the acute treatment of migraine, expanding the therapeutic options for those patients not well served by existing nonoral agents.
Zavegepant nasal spray (Zavzpret, Pfizer Inc., USA) was approved in 2023 for the acute treatment of migraine in the US and remains under development for other regions of the world. Prior research has shown that zavegepant nasal spray is rapidly absorbed (median time to maximum plasma concentration (Tmax) for the approved 10 mg dose of approximately 30 minutes (12)) with a low potential for drug-drug interactions (13,14). Single doses of 10 or 20 mg zavegepant were effective for the acute treatment of migraine, with favorable safety, in a randomized, dose-ranging, placebo-controlled, phase 2/3 trial (15). A double-blind, randomized, placebo-controlled, multicenter phase 3 trial confirmed the efficacy of zavegepant 10 mg in the acute treatment of migraine (16), as well as favorable tolerability and safety. However, neither single-attack study provided information about the long-term safety and tolerability of zavegepant. The objective of the present study was to evaluate the safety and tolerability of zavegepant in the acute treatment of migraine under repeated, as-needed dosing for up to one year.
Methods
Ethics
This study was prospectively registered at clinicaltrials.gov (NCT04408794). It was conducted in accordance with the principles of the Guidelines for Good Clinical Practice, the Declaration of Helsinki and all applicable local regulations. The protocol was approved by independent ethics committees and/or institutional review boards at each study center. Before any study-related procedures were undertaken, participants provided written informed consent.
Study conduct
This phase 2/3, multicenter, open-label study of the safety and tolerability of long-term use of zavegepant 10 mg nasal spray was conducted at 63 sites in the US and included three phases: a screening visit/28-day observation phase, a 52-week long-term treatment phase, and a follow-up safety visit 14 ± 2 days after the end of treatment. After informed consent was obtained at the screening visit, investigators or qualified designees entered participants into the study, obtained a participant number assignment via an interactive web response system, and gave participants an electronic diary (Clario, USA). Participants were able use a provisioned device, the Electronic Clinical Outcome Assessment handheld device (Clario, USA), or their own smartphone device by downloading an application to report the evening reports. Participants also had access to a back-up method of reporting the electronic evening reports on a password-protected website.
Since this was a single arm, open-label study, all eligible participants were assigned to the same treatment of zavegepant 10 mg intranasally, as needed, for the acute treatment of a migraine attack of any intensity. At the conclusion of the 28-day observation phase, eligibility was confirmed at the baseline visit, and participants were given a box containing four liquid spray devices (Unidose [UDS] system, Aptar Pharma, USA), each of which was designed to deliver a single 10 mg dose of zavegepant nasal spray. Participants may have been given more than one box of four devices at a study visit to provide a sufficient number of devices between visits. Participants were instructed to self-administer one spray as needed from the liquid spray device for up to 52 weeks; they were instructed not to administer more than one spray per calendar day. Participants were permitted to administer study drug a maximum of eight times per month (every 28 days). Participants were also instructed on the use of an electronic diary to capture information about the following: migraine attack occurrence and pain intensity; use of standard-of-care medication during the observation phase; use of study drug and nostril of administration during the long-term treatment phase; preference of medication; and satisfaction with medication. Participants were instructed to record migraine attack occurrences every day. They were also instructed to record any concomitant medication use, including migraine standard-of-care medications, in a concomitant medication log. Before participants were discharged from the study site, investigators or qualified designees ensured that they understood how to use the electronic diary and the liquid spray device.
During the long-term treatment phase, participants visited the study site every two weeks (±2 days) during the first month and then every four weeks (±7 days) until Week 52. At the end of Week 52, participants returned to the study site for the final review of the electronic diary and assessments of medication compliance and tolerability and safety. Participants who completed the 52-week long-term treatment phase or discontinued early from the long-term treatment phase completed a follow-up visit within 14 ± 2 days after their last site visit. Those who did not treat a migraine attack by Week 8 of the long-term treatment phase were discontinued from the study. The total study duration was approximately 58 weeks.
Because this study was conducted during the COVID-19 pandemic, provisions were made to minimize potential hazards to study participants arising from in-person study visits. Alternatives to in-person study visits included conducting remote study visits via phone/telemedicine video, focusing on safety assessments during remote visits, performing safety lab tests via local laboratories or through professional in-home phlebotomy vendors, and shipping of study medication directly to study participants. Although every effort was made to conduct study visits within the specified windows, in-person visits could be performed outside specified windows to minimize risks to participants and to comply with governmental and institutional guidance and local COVID-19 safety requirements.
Participants
The study population included men and women aged 18 years and older who had migraine with or without aura according to the criteria of the International Classification of Headache Disorders, 3rd Edition (17); a one-year history of attacks lasting four to 72 hours if untreated, with the age of onset prior to 50 years of age; at least two and not more than eight migraine attacks of moderate or severe pain intensity per month, as well as fewer than 15 days per month with migraine or nonmigraine headache within the last three months. Participants had to be able to distinguish migraine attacks from attacks of tension-type headache and cluster headache, and those taking preventive migraine medication were permitted to remain on therapy if they had been on a stable dose for at least three months before the screening visit, and the dose was not expected to change during the course of the study. Participants with contraindications to triptans could be included if they met all other criteria for inclusion. Concomitant use of another gepant was prohibited during the study; CGRP monoclonal antibodies were permitted. Participants were permitted to use other previously prescribed medications for the acute treatment of migraine as needed, specifically aspirin, ibuprofen, acetaminophen up to 1 g/day (maximum two consecutive days), naproxen or other nonsteroidal anti-inflammatory drugs, antiemetics, or baclofen. Triptans, lasmiditan, and ergotamine medications were prohibited from ≥2 days prior to the baseline visit and subsequently throughout the study. Women of childbearing potential and nonsterile men could participate if they were using two acceptable methods of contraception to avoid pregnancy throughout the study, and the women had a negative serum or urine pregnancy test (minimum sensitivity 25 IU/L or equivalent units of human chorionic gonadotropin) at baseline and were not breastfeeding.
Participants were excluded if they had a history of migraine with brainstem aura or hemiplegic migraine or a history of human immunodeficiency virus disease. They were also excluded if they had a history or diagnosis of Gilbert's Syndrome or active hepatic or biliary disease; aspartate aminotransferase (AST), alanine aminotransferase (ALT), or serum bilirubin (total, direct, or indirect) greater than 1x the upper limit of normal (ULN) at the pre-baseline visit; diseases or conditions causing malabsorption (e.g. severe septum deviation, nasal deformity or blockage, inflammation, perforation, mucosal erosion or ulceration, polyposis, nasal trauma); or alcohol or drug abuse within the past 12 months. Participants with the following current conditions were also excluded: uncontrolled, unstable, or recently diagnosed cardiovascular disease; uncontrolled hypertension; uncontrolled diabetes; bodymass index ≥33 kg/m2; unstable medical conditions; diagnosis of major depressive disorder, pain syndromes, psychiatric conditions, or significant neurological disorders; current diagnosis of schizophrenia, major depressive disorder requiring treatment with atypical antipsychotics, bipolar disorder, or borderline personality disorder; and medically significant positive drug screen for drugs of abuse.
Complete inclusion and exclusion criteria are available in the study protocol (https://classic.clinicaltrials.gov/ProvidedDocs/94/NCT04408794/Prot_000.pdf).
Assessments
Safety assessments included: adverse events (AEs) (nonserious and serious AEs); vital signs (seated arterial systolic and diastolic blood pressure, radial artery pulse rate, respiratory rate, and body temperature) and physical measurements (height, weight); electrocardiograms; physical examinations; clinical laboratory test evaluations (hematology, serum chemistry/electrolyte, liver function tests (LFTs), lipid panel, estimated glomerular filtration rate, urinalysis, urine drug screen, follicle stimulating hormone); pregnancy tests (serum or urine); and the Sheehan Suicidality Tracking Scale (18). For clinical laboratory evaluations, participants were instructed to fast for a minimum of eight hours prior to blood draws at baseline, Week 4, Week 24, and Week 52. If a participant was not fasting at a given visit, the blood draw was still performed.
Exploratory efficacy assessments were the number and severity of migraine days per month, migraine-specific quality of life, preference of medication, satisfaction with medication, migraine-related disability, and total improvement relative to the investigator's past experience with other patients with the same diagnosis. The results of these exploratory assessments are not presented in this manuscript.
Statistical analysis
Populations evaluated and used for analysis of the data included the following analysis sets: enrolled (participants who signed informed consent and were assigned a participant identification number), long-term treatment (enrolled participants who entered the long-term treatment phase), and safety (enrolled participants who took study drug).
The primary safety and tolerability endpoints were the frequency (i.e. number and percentage of participants) of AEs occurring in ≥5% of treated participants by severity, serious AEs, AEs leading to study drug discontinuation, and laboratory test abnormalities by toxicity grade. Investigators determined the severity (e.g. mild, moderate, severe) of AEs and the relationship of AEs to study drug; their terms were coded and grouped by system organ class (SOC) and preferred term (PT) using the Medical Dictionary for Regulatory Activities (MedDRA). The highest severity on treatment was reported for each AE PT. Laboratory test results were graded according to numeric laboratory test criteria using US units (19,20). The worst (highest) toxicity grade on treatment was reported for each test.
Due to the history of potential drug-induced liver injury with early generation gepant agents (21,22), there was a focus on evaluating transaminase elevations and hepatic-related AEs. Exploratory safety endpoints included the frequency of AEs of special interest on treatment, and the frequency of LFT elevations (AST, ALT, alkaline phosphatase, and total bilirubin) based on fold changes above ULN and the frequency of elevations of AST or ALT greater than 3x ULN concurrent with total bilirubin greater than 2x ULN (where concurrent was defined as the same collection date). The AEs of special interest — potential drug abuse AEs, medication-overuse headache AEs, hepatic-related AEs, local irritation AEs, cardiovascular AEs, and suicidality AEs (completed, attempted, ideation) — were prespecified in the statistical analysis plan and identified primarily from standardized MedDRA queries and relevant PTs. The standardized MedDRA queries were aligned with the version of MedDRA used for analyses. The PTs for AEs categorized as associated with potential abuse included ‘drug abuse, dependence, and withdrawal’ standardized MedDRA query; relevant PTs in the depressant, stimulant, and psychotomimetic categories of the General disorders and administration site conditions SOC, Nervous system disorders SOC, and Psychiatric disorders SOC, as recommended in Section V.B of the FDA Guidance for Industry Assessment of Abuse Potential of Drugs (23); and dizziness, but only if concurrent with any euphoria-related AE.
With a sample size of approximately 600 treated participants and no events observed, the upper bound of a 1-sided 95% confidence interval for zero observations is 0.005. As a result, this sample size was large enough to rule out AEs that occur at rates greater than five cases per 1000 participants.
Statistical analyses were performed using SAS, version 9.4 (SAS Institute, USA).
Results
Participants
Participants were enrolled between 29 June 2020 and 4 December 2020, and the database was locked on 16 February 2022. Of the 974 participants who were enrolled, 608 entered the long-term treatment phase, 603 were treated with zavegepant 10 mg nasal spray, and 341 (56.6%) completed the study (Table 1). Of the 603 treated participants, 111 (18%) participated in a previous single-attack trial of one dose of zavegepant nasal spray or placebo (NCT04571060). In the previous trial, 86 (14%) participants received zavegepant, and 25 (4%) received placebo. The most common reason for not entering the long-term treatment phase was failure to meet inclusion/exclusion criteria, which affected 7.4% (72/974) of participants who did not enter the observation phase and 29.4% (286/974) of those who entered the observation phase. One participant (0.1%) did not enter the long-term treatment phase due to COVID-19. The most common reasons for discontinuation from the study were lack of efficacy (10.1% [61/603]) and withdrawal by participant (9.5% [57/603]).
Participant disposition – enrolled analysis set.

STS, Suicidality Tracking Scale
Did not enter observation phase/withdrawal by participant.
Adverse event, no migraine attack treated by week 8 visit (two participants), noncompliance, and withdrawal by participant.
Percentages are based on the long-term treatment analysis set (N = 608).
Percentages are based on the safety analysis set (N = 603), starting from the “completed study” row.
45 participants discontinued due to an AE. Forty-one of those participants had treatment-emergent AEs as shown in Table 4.
<2 doses per month over three consecutive months.
The treated population had a mean (SD) age of 42.1 (12.46) years and was 85.7% (517/603) female and 83.3% (502/603) White (Table 2). The mean (SD) number of moderate or severe attacks per month prior to study entry was 5.0 (1.89), and 18.1% (109/603) of treated participants were using preventive migraine medication. In total, 39 treated participants (6.5%) used a CGRP monoclonal antibody, including erenumab (n = 22), galcanezumab (n = 11), and fremanezumab (n = 7). Overall, 39.8% (240/603) of participants had previously discontinued ≥1 triptan due to inadequate efficacy and/or poor tolerability; 33.3% (201/603) were currently using a triptan prior to entering the study. A total of 23.5% (142/603) of participants had cardiovascular risk factors, including, most commonly, a family history of coronary artery disease (10.8% [65/603]), treated hypertension (6.6% [40/603]), and treatment with a statin (4.8% [29/603]). Four (0.7%) of the 603 treated participants had cardiovascular contraindications to triptans (Table 2). Participants used a mean (SD) of 3.1 (1.55) zavegepant doses per month; in total, 18,857 sprays were administered across all participants (Table 3).
Demographics and baseline characteristics – safety analysis set.
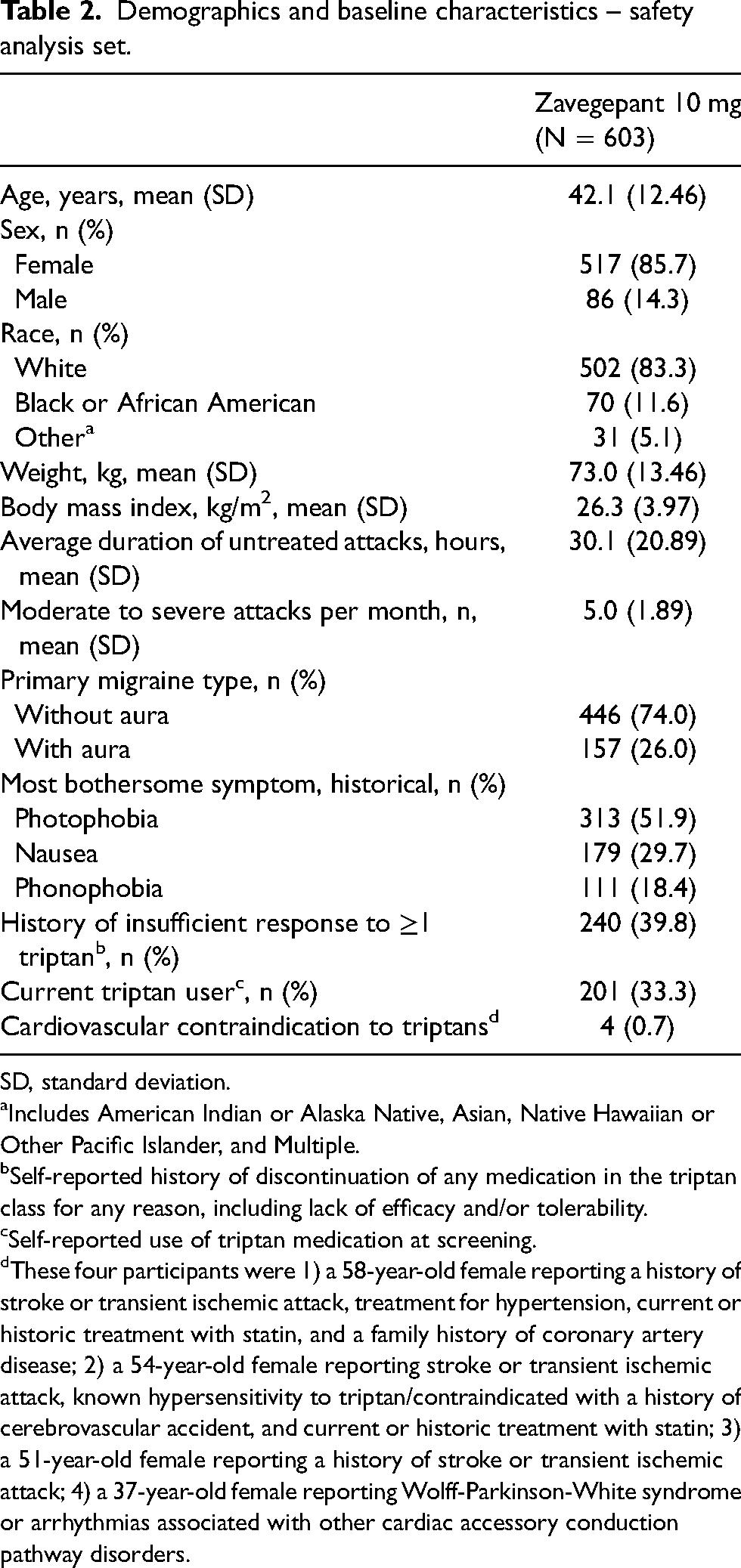
SD, standard deviation.
Includes American Indian or Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, and Multiple.
Self-reported history of discontinuation of any medication in the triptan class for any reason, including lack of efficacy and/or tolerability.
Self-reported use of triptan medication at screening.
These four participants were 1) a 58-year-old female reporting a history of stroke or transient ischemic attack, treatment for hypertension, current or historic treatment with statin, and a family history of coronary artery disease; 2) a 54-year-old female reporting stroke or transient ischemic attack, known hypersensitivity to triptan/contraindicated with a history of cerebrovascular accident, and current or historic treatment with statin; 3) a 51-year-old female reporting a history of stroke or transient ischemic attack; 4) a 37-year-old female reporting Wolff-Parkinson-White syndrome or arrhythmias associated with other cardiac accessory conduction pathway disorders.
Zavegepant exposure during one year of open-label zavegepant 10 mg nasal spray for the acute treatment of migraine – safety analysis set.

SD, standard deviation.
Defined as four-week intervals (28 days).
Safety
During one year of open-label treatment with zavegepant, 76.1% (459/603) of participants experienced treatment-emergent AEs (TEAEs). The most common TEAEs (≥5% of participants) were dysgeusia (39.1% [236/603]); nasal discomfort (10.3% [62/603]); COVID-19 (7.5% [45/603]); nausea (6.1% [37/603]); nasal congestion and throat irritation (5.5% [33/603] each); and back pain (5.3% [32/603]), as shown in Table 4. In total, 6.8% (41/603) of treated participants had an AE leading to study drug discontinuation; the most common AEs leading to discontinuation were dysgeusia (1.5% [9/603]); nasal discomfort (0.8% [5/603]); ALT increased, AST increased, and throat irritation (each 0.7% [4/603]); and dizziness, migraine, nausea, and rhinorrhea (each 0.5% [3/603]). Of the 603 participants evaluated for safety, 22 (3.6%) had a severe AE, and seven (1.2%) reported a serious AE on treatment. None of the serious AEs were considered related to treatment by the investigators, and none were reported in more than one participant. The serious AEs were appendicitis, back pain, bile duct stenosis, concussion, fall, herpes zoster meningoencephalitis, multiple sclerosis, pleurisy, and pneumonia. Aminotransferases >3x ULN occurred in 2.6% (15/579) of participants with on-treatment LFT data, none of whom had concurrent elevations in bilirubin >2x ULN.
Treatment-Emergent adverse events during one year of open-label zavegepant 10 mg nasal spray – safety analysis set. Values are n (%).

AE, adverse event.
Treatment-emergent AEs, a subset of on-treatment AEs, were those that developed, worsened, or became serious on treatment relative to pretreatment.
Over the course of the study, participants who averaged <6 sprays/month and those who averaged ≥6 sprays/month experienced similar rates of AEs (76.1% [434/570] vs 78.8% [26/33]), AEs leading to study drug discontinuation (6.8% [39/570] vs 6.1% [2/33]), treatment-related AEs (57.0% [325/570] vs 51.5% [17/33]), and local irritation AEs (49.8% [284/570] vs 45.5% [15/33]). The incidence of AEs was also comparable in participants who used ≥80 sprays (76.2% [16/21]) and those who used ≥20 to <40 sprays (81.1% [154/190]), ≥40 to <60 sprays (84.8% [117/138]), or ≥60 to <80 sprays (81.8% [36/44]). Although rates in participants who used <20 sprays were lower (65.2% [137/210]), findings in this subgroup include those who discontinued the trial very early. Treatment-related AEs were comparable across cumulative exposure (42.9% [9/21] for ≥80 sprays vs 52.9% [111/210] for <20 sprays), as were rates of treatment-related AEs (56.6% [73/129] vs 58.9% [182/309]) and local irritation AEs (46.5% [60/129] vs 53.4% [165/309]) in participants with <12 weeks on treatment and those with ≥48 weeks on treatment.
Overall, 7.3% (44/603) of participants had at least one AE on treatment categorized as associated with potential drug abuse (Table 5). The most frequent of these AEs (≥1% of participants) were fatigue (2.5% [15/603]) and insomnia (2.7% [16/603]), both of which were mild in the majority of cases. No other AE was reported by more than three (0.5%) participants.
Most common (reported in ≥1% of participants) adverse events categorized as associated with potential drug abuse – safety analysis set.

AE, adverse event.
Hepatic-related AEs were reported in 23 (3.8%) participants. Those reported in more than one participant were ALT increased (15 participants), AST increased (11 participants), blood alkaline phosphatase increased (five participants), and gamma-glutamyl transferase increased, hepatic enzyme increased, and LFT increased (two participants each). Hepatic-related AEs led to discontinuation of study drug in 5 (0.8%) participants.
Local irritation AEs were reported in 299 (49.6%) participants. The most frequently reported AEs were dysgeusia (39.1% [236/603]), nasal discomfort (10.3% [62/603]), and throat irritation (5.5% [33/603]). The majority of local irritation AEs were mild or moderate in intensity. Fourteen (2.3%) participants discontinued use of zavegepant due to local irritation AEs, with the most frequent (>1 participant) being dysgeusia (nine [1.5%] participants), nasal discomfort (five [0.8%]), throat irritation (four [0.7%] participants), and rhinorrhea (three [0.5%] participants).
No participants experienced AEs in the AEs of special interest categories of medication-overuse headache, cardiovascular, or suicidality.
The most frequently observed on-treatment laboratory abnormalities were related to lipid elevations, specifically, low-density lipoprotein-cholesterol (44.3% [206/465]), cholesterol (36.6% [170/465], and triglycerides (29.6% [138/466]). LFT elevations greater than the ULN were reported for ALT (28.2% [163/579]), AST (17.1% [99/579]), ALT or AST (31.4% [182/579]), alkaline phosphatase (14.3% [83/579]) and total bilirubin (4.7% [27/579]). Elevations >3x ULN were reported for ALT (1.6% [9/579]), AST (1.7% [10/579]), and ALT or AST (2.6% [15/579]). No participants had concurrent on-treatment elevations of ALT or AST >3x ULN and total bilirubin >2x ULN.
Discussion
This phase 2/3 study was conducted to evaluate the safety of repeated doses of zavegepant 10 mg nasal spray in the acute treatment of migraine. Results showed that zavegepant 10 mg nasal spray, administered as needed for up to eight doses per month and for up to 52 weeks in adults with migraine, was well tolerated with a favorable safety profile across a variety of safety endpoints, including AE assessments, clinical laboratory testing (including LFTs), vital signs, and electrocardiograms. No deaths were reported, serious AEs were reported in fewer than 2% of participants, and AEs leading to discontinuation were uncommon. Other than the local irritation AEs associated with nasal administration, the AE profile was generally reflective of concurrent medical conditions and illnesses, including seasonal illnesses, that are often observed in patients with migraine, particularly over the course of a year. The results from subgroups by duration and frequency of dosing suggested no association between AEs and dosing frequency or zavegepant exposure, and the majority of AEs, including hepatic-related AEs, were mild or moderate in intensity. No zavegepant-treated participants, including four who had a cardiovascular contraindication to triptans, had cardiovascular AEs. There were no AEs associated with medication-overuse headache or suicidality.
Dysgeusia was experienced by 39% [236/603] of participants. As this predictable side effect of nasal spray formulations (24) was mild in 75% [178/236] of cases and led few participants (1.5% [9/603]) to discontinue the study, the finding — together with the low overall rate of discontinuation — provides additional evidence that up to one year of zavegepant nasal spray was safe and well tolerated.
While lipid elevations were the most frequently observed on-treatment laboratory abnormalities, the incidence of lipid elevations was consistent with the those reported at baseline. We note that interpretation of the lipid results is complicated by pretreatment lipid elevations (i.e. >Grade 0), relatively infrequent sampling, intermittent and variable dosing frequency, and inconsistencies in the fasting status within and across participants.
These results support the use of zavegepant as a safe and tolerable alternative to oral and parenteral agents for the acute treatment of migraine. The demonstrated efficacy profile of zavegepant nasal spray in previous studies provided initial proof for the clinical utility of this unique nonoral therapy. In particular, with previous data indicating an onset of efficacy as early as 15 minutes postdose (16), the nasal spray formulation may help to optimize drug administration during attacks where a faster onset of relief is needed. Additionally, intranasal administration may mitigate the impact of nausea or vomiting on oral dosing and obviate potential effects of gastroparesis on zavegepant absorption.
This study has several limitations and strengths. Besides the known limitations of an open-label, uncontrolled study for distinguishing treatment-associated outcomes from background effects, others include limited representation of men, limited diversity in race and ethnicity, and the exclusion of triptans, lasmiditan, and ergotamine medications and participants with some medical conditions; these factors limit the generalizability of results. Because the study design was not optimized for detecting rare events, cardiovascular safety remains a focus of postmarketing safety surveillance. Strengths of the present study include the large sample size and the high number of treated attacks over the course of a year. In addition, participants had concurrent medical conditions that were largely reflective of the potential treatment population and used a broad array of concomitant medications.
Zavegepant 10 mg nasal spray has previously demonstrated efficacy and safety in the acute treatment of migraine in single-attack trials (15,16). This long-term safety study expands the safety profile of zavegepant by providing evidence of safety and tolerability from a relevant, large population for up to 52 weeks.
Conclusions
During one year of open-label treatment, zavegepant 10 mg nasal spray demonstrated favorable safety and tolerability in the acute treatment of migraine.
Zavegepant nasal spray is the first CGRP receptor antagonist for intranasal administration. Prior to this study, the safety and tolerability of zavegepant 10 mg nasal spray for the acute treatment of migraine had only been demonstrated in single-attack studies, and its long-term safety was unknown. This one-year open-label safety study demonstrated favorable safety and tolerability for zavegepant 10 mg nasal spray for the acute treatment of migraine.
Footnotes
Acknowledgements
The authors thank the study participants and site staff.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KM serves as a consultant, advisory board member, or has received honoraria from Amgen, Teva, Theranica, Vorso, Biohaven, electroCore, and Eli Lilly.
RC was an employee of Biohaven Pharmaceuticals, owns stock in Biohaven Ltd, was an employee of Pfizer, has received research payments from Pfizer, and provides services to Collima LLC which has had consulting agreements with Pfizer, Actio Biosciences, Inc., Aptose Biosciences Inc., Manistee Therapeutics, and Vida Ventures Management Co., LLC.
LM and TF are employed by Pfizer Inc. JM was employed by Biohaven Pharmaceuticals at the time the study was conducted. JM and LM own stock in Biohaven Pharmaceuticals. LM owns stock in Pfizer Inc.
RBL serves on the editorial board of Neurology and as senior advisor to Headache but is not paid for his roles on these journals. He has received research support from the NIH. He also receives support from the National Headache Foundation. He receives research grants from Allergan/AbbVie, Amgen, Dr. Reddy's Laboratories, and Novartis. He has reviewed for the NIA and NINDS and serves as consultant, advisory board member, or has received honoraria from Allergan/AbbVie, Amgen, Biohaven, Dr. Reddy's Laboratories, electroCore, Eli Lilly, GlaxoSmithKline, Merck, Novartis, Teva, and Vedanta. He receives royalties from Wolff's Headache (8th Edition, Oxford University Press, 2009) and Informa. He holds stock options in Biohaven Pharmaceuticals and Manistee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Biohaven Pharmaceuticals, Inc., which was acquired by Pfizer in October 2022. Medical writing services were provided by Christopher Caiazza at Polymedia Corporation and funded by Pfizer.