
Abstract
In 1992 a nasal spray formulation of butorphanol, an opioid medication intended for pain relief, was marketed in the USA on an unscheduled basis. Only a few years later, amid widespread reports of abuse and dependence, primarily in migraine patients, its manufacturer voluntarily requested the Food and Drug Administration to reschedule the drug as a Schedule IV narcotic. The events surrounding this episode are reviewed, and four problem areas that might have contributed are identified: (i) inadequate review of previous experience with other formulations of butorphanol; (ii) failure to consider the impact of disease state and drug formulation on the risk of adverse events; (iii) the limited scope of clinical trials prior to approval; and (iv) aggressive marketing efforts. The implications of these lessons for future drug development and post-marketing surveillance in the migraine field are considered.
Introduction
In 1992 a nasal spray formulation of butorphanol, an opioid medication intended for pain relief, was marketed in the USA. Butorphanol was not a new drug. An injectable version had been available for some time and was used in hospital settings, principally for the treatment of postoperative and labour pain. The nasal spray formulation of the drug was intended as a fast-acting, convenient method of treating acute pain that would provide relief comparable to that of the injectable drug without the inconvenience of an injection. It had been evaluated in clinical trials involving acute pain states such as postoperative pain, dental pain and migraine headache, and had a rapid onset of action with pain relief lasting from 3 to 5 h (1).
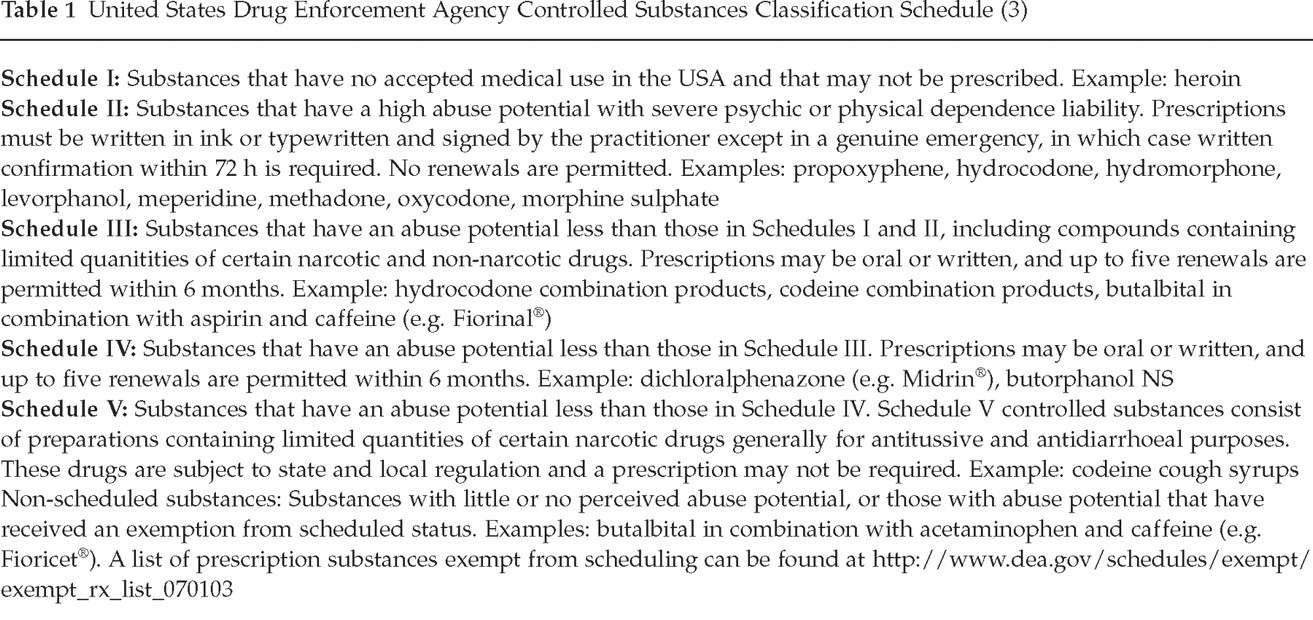
In 1991 meetings of the United States Food and Drug Administration (FDA) Drug Abuse Advisory Committee (DAAC), the manufacturer of butorphanol nasal spray opposed suggestions that the drug be scheduled, a move that would have required greater controls on prescriptions (2). As summarized in Table 1, the Drug Enforcement Agency (DEA) Schedule of Controlled Substances classifies drugs in one of five categories, ranging from Schedule I (no medical use; not prescribed) to Schedule V (limited quantities of drugs with some abuse potential). The act establishing the scheduling process provides that ‘proceedings to add, delete, or change the schedule of a drug or other substance may be initiated by the Drug Enforcement Administration (DEA), the Department of Health and Human Services (HHS), or by petition from any interested party, including the manufacturer of a drug, a medical society or association, a pharmacy association, a public interest group concerned with drug abuse, a state or local government agency, or an individual citizen. When a petition is received by the DEA, the agency begins its own investigation of the drug’ (3). Information subsequently obtained under the Freedom of Information Act about the DAAC meetings suggests that the company was concerned that a scheduled status for butorphanol nasal spray would have the effect of decreasing prescriptions for the drug. In these hearings, the company presented evidence suggesting that butorphanol was less likely than other pain medicines to produce abuse or addiction (2). The DAAC voted not to recommend scheduling of the drug, and in late 1991 the manufacturer received approval to market butorphanol nasal spray for treatment of acute pain in a non-scheduled manner.
United States Drug Enforcement Agency Controlled Substances Classification Schedule (3)
In early marketing and promotional efforts, the manufacturer advocated use of the drug for treatment of acute pain, especially that of migraine headache (2). Ultimately, around 60% of prescriptions for the drug were for the purpose of treating migraine, despite the fact that it did not have a specific indication for that disorder. Soon, however, previous reports of dependence, addiction and even deaths associated with butorphanol were unearthed (4–6), and new ones began to appear in medical journals and the popular press (7, 8). In the few years after introduction of butorphanol nasal spray, the number of adverse drug reactions reported to the FDA related to butorphanol rose from 60 to 400 per year, with dependence/addiction accounting for 24% of such reports, up from 6.5% before introduction of the nasal spray formulation (2). Nearly all of the reports of problems with the drug involved patients using it to treat migraine.
By 1998, numerous lawsuits had been filed against the manufacturer, claiming that it knew or should have known that butorphanol can be habit-forming and that it had inappropriately promoted the drug as non-addictive. The American Trial Lawyers Association was reported to have a working group devoted to this litigation, among 61 other such working groups devoted to such things as asbestos, lead paint and airplane accidents (9). One class action lawsuit was settled in 1999 out of court (although the court refused certification of the class) and others remain in litigation (10). An internet search using the drug's brand name ‘Stadol®’ returns a plethora of stories such as the following:
‘My wife was given stadol for her migraines in 1993. By 1996 she and both of my daughters were addicted. One daughter is currently in prison as a result of bad checks and fraud to obtain this poison. My younger daughter and my wife were arrested for trying to fraudulently obtain stadol. My wife was a good mother and had never been in trouble with the law until she found this stuff. All of the Drs told her it was not addictive and she was able to get it over the phone at will. I have never been one to sue people but this drug was totally misrepresented to us’ (11).
‘… I too got addicted to stadol in 1995. As you say, it was marketed as a completely safe drug for migraines. I am a registered nurse and my husband is an internal/ER doc. I got samples from sales reps, my neurologist, internal med doc and also my husband wrote when I could not get it. He subsequently got in trouble with the state medical board when it became a controlled drug in October 1997. So then I simply started forging prescriptions myself. Never in my career have I ever thought of stealing, forging or taking any drug from patients or family. But I would do anything to get my stadol. I am now under investigation by the DEA and will more than likely be arrested. My career is ruined, my husband's career is severely damaged … I feel most sorry for my family for what I have put them through, but also for myself and the fact that the drug was so misrepresented. My husband and I went to a seminar which he was required by the board to go to given by a Dr that works with addiction, but also for Bristol-Myers, of course he could not come right out and say anything bad, but did pull my husband aside and said he thought all along stadol NS should be a controlled drug from the start. So now I am facing arrest and like your wife have never been in trouble ever in my life …’ (12).
‘I'm wanting to talk with anyone who has had a bad experience with Stadol Nasal Spray. I'm in terrible trouble with this drug and I want to talk with someone who can relate’ (13).
In 1995, only 3 years after its introduction to the market, amid widespread reports of abuse and addiction problems related to butorphanol nasal spray, primarily in headache patients, the manufacturer of butorphanol nasal spray took the unusual step of voluntarily requesting that the FDA reclassify butorphanol nasal spray as a controlled substance. On 31 October 1997, the FDA declared butorphanol a Schedule IV narcotic (14). Table 2 summarizes the timing and sequence of events surrounding the scheduling of butorphanol nasal spray.
Some events leading up to and following the approval and rescheduling of butorphanol nasal spray

DAAC, Drug Abuse Advisory Committee of the United States Food and Drug Administration; NS, nasal spray.
What went wrong?
A review of the pharmacological effects of butorphanol provides a useful background for understanding the clinical trials and post-marketing problems experienced with the drug. Butorphanol is an opioid analgesic. The term ‘opioid’ refers to a group of drugs that bind to opioid receptors; many, but not all, of these drugs have morphine-like properties. The principal medical use of these drugs is to relieve pain, although they can be effective in suppressing cough and controlling diarrhoea as well. Most opioids unavoidably produce some depression of central nervous system function (sedation, confusion, slowed reaction times), and most can be habit-forming or addictive (15). The term ‘narcotic’ is often used to refer to this class of medications, but is in fact a general term that applies to any drug that depresses the central nervous system enough to produce decreased responsiveness to external stimuli.
Although butorphanol is a member of the opioid class of medications because it has morphine-like effects at the same mu opioid receptor stimulated by morphine, its pharmacology is complex, and it is subclassified as a ‘partial agonist and mixed agonist/antagonist’ opioid. Activation of mu receptors (agonist activity) generally produces euphoria, pain relief, and sedation. However, some of butorphanol's effects at the mu receptor counteract those that would be produced by morphine (antagonist activity). In fact, if butorphanol is given to a person who is dependent upon morphine or another pure mu agonist, it can produce withdrawal symptoms. In addition, butorphanol has effects at the kappa opioid receptor, which can produce unpleasant emotional sensations and dysphoria (15). The fact that butorphanol was not a pure mu agonist, and that it sometimes produced dysphoria, led many to believe that it would be less addictive than other opioid drugs (16).
Four problem areas
What lessons can be drawn from the clinical trials and post-marketing experience with butorphanol nasal spray? Available evidence suggests four areas that, in hindsight, deserved more scrutiny than they received: (i) previous experience with butorphanol and similar drugs; (ii) the impact of disease state and drug formulation on the risk of adverse events, especially dependence and addiction; (iii) the limited scope of clinical trials of butorphanol nasal spray in migraine; and (iv) initial marketing efforts that emphasized low addiction potential of the drug.
Review of previous data
Based on evidence suggesting a low abuse potential for butorphanol, its manufacturer persuaded the FDA that the new formulation should not be classified as a controlled substance. However, the question of whether butorphanol might prove addictive had been considered previously, in 1978, when injectable butorphanol was first presented for approval. At that time, an FDA Drug Abuse Advisory Committee recommended that the drug should be classified as a scheduled narcotic because of its abuse potential. This recommendation was not adopted (16), and apparently was not reconsidered by either the manufacturer or the FDA prior to the 1991 FDA decision about butorphanol nasal spray.
Much of the evidence presented to the FDA and physicians suggesting that butorphanol had a low potential for causing abuse or addiction was generated by or involved a single physician who served as a consultant to the drug's manufacturer and was a member of the FDA Drug Abuse Advisory Committee (17–19). His work was cited by other sources in their statements that butorphanol has low abuse liability. This physician recused himself from committee considerations of butorphanol (2), but the dual professional association raises concerns of possible bias or conflict of interest, and the extent of reliance on a single expert's work is troubling.
In addition to these earlier concerns about the abusability of butorphanol, information existed at the time of butorphanol nasal spray approval about other opioid medications that had initially been thought to have low addiction liability but had in fact turned out to have high abuse potential. These included pentazocine (Talwin®), like butorphanol an agonist/antagonist drug that had been hailed as less addictive than other opioids, and had been a non-scheduled drug for 12 years until its addictive potential was recognized (20).
Title 21 of the United States Code Controlled Substances Act outlines a number of factors to be considered in determining whether a drug should be classified as a controlled substance (21). These include the actual or relative potential for abuse, scientific evidence of its pharmacological effect, the state of current scientific knowledge regarding the drug, its history and current pattern of abuse, the scope, duration and significance of abuse, what risk there is to public health and its psychic or physiological dependence liability, as well as whether the substance is a precursor of another controlled substance. Sidney Wolfe of the Public Citizen's Health Research Group has observed that ‘these factors rely heavily on a large number of consumers being harmed before a drug is controlled’ and ‘in effect makes the American public subjects in a large uncontrolled experiment in which the participants have not been fully informed of the risk of dependence with the drug’ (22).
The effects of delivery system and disease state
It has been suggested that a false sense of safety was created because injectable butorphanol had not been widely abused. Use of the injectable drug was limited to medical settings, meaning it was given in controlled circumstances under direct medical supervision. This probably limited the extent of diversion and misuse, since availability of a drug affects its abuse potential (23, 24). For this reason, early reports of medical professionals misusing the injectable formulation (25, 26) should probably have been viewed as evidence of the potential for abuse if the drug became available in a more easily administered formulation that could be used unsupervised in non-medical settings. Information submitted to the FDA as part of the approval process for butorphanol nasal spray indicated that 2446 subjects had been studied in butorphanol clinical trials, but that only ‘approximately half’ received the nasal spray formulation; the rest had received intravenous medication. It was further observed by the manufacturer that ‘the type and incidence of side-effects with butorphanol by any route were those commonly observed with opioid analgesics’ (27).
The presentation of results from trials using different formulations of the drug may have obscured adverse events due to the nasal spray formulation of the drug rather than the drug itself. Drugs that can be taken by sniffing, snorting or injection are often more highly abusable than drugs which are taken by mouth (28). In the case of butorphanol, the alternative method of delivery (nasal spray rather than intravenous administration) appears to have increased the addictive potential of butorphanol. Such an increase might have been predicted based on understanding of the rapid, reinforcing nature of nasal spray drug administration, combined with unsupervised administration.
Failure to consider impact of the disease state on the risk of dependence or addiction may also have contributed to an inaccurate understanding of potential problems with the drug. There is no indication that consideration was given to the possibility migraine patients might use the drug more frequently or have a higher risk of dependence or addiction than patients with self-limited dental or orthopaedic pain syndromes. Unlike some of the other pain states in which the drug was tested, though, migraine is a chronic illness in which patients can be expected to suffer headaches at regular intervals for years or decades. The tendency of headache patients to overuse abortive medications for headache is widely recognized. Despite this, evidence of the drug's effect in other pain states was accepted as applicable to its effect in migraine. In retrospect, it seems clear that this led to incorrect conclusions about the magnitude of the risk of addiction and dependence.
The limited scope of clinical trials
The clinical trials of butorphanol nasal spray for the treatment of acute migraine were conducted properly, but the population studied was not representative of those actually treated with the drug after its approval. As in most drug trials assessing the efficacy of treatments for migraine, subjects with frequent or refractory headaches were excluded from the butorphanol trials (29). In clinical practice, of course, it is such patients who are most likely to be prescribed a potent new pain reliever for headaches. Similarly, subjects with a prior history of substance abuse were not allowed to participate in the trials; in clinical practice, such patients are not rare. At least some patients in butorphanol nasal spray trials apparently did display difficulties with overuse, suggestive of dependence.
The original package insert for butorphanol nasal spray identified only two trials of the nasal spray formulation in migraine, comprising a total of 107 subjects for whom the drug was used to treat only one headache (27). Although some of the premarketing trials of butorphanol were characterized as ‘long-term’, such language may be misinterpreted. In these studies ‘long-term’ use referred to subjects allowed to use the drug for the treatment of intermittent migraine attacks for up to a year. In fact, the majority of patients who have migraine can expect to have attacks over many decades, and trial length of a year or less is inadequate to establish the true harm-to-benefit ratio of a treatment that is likely to be used for decades or longer.
Such longer-term trials present many design and financial obstacles that may make them impractical, but the limitations of shorter-term data need to be clearly recognized. In such situations, post-marketing surveillance studies assessing drug use in real-world conditions can be important, and the FDA may require them. In hindsight, its failure to anticipate the need for such studies in the case of butorphanol nasal spray was an error.
In summary, clinical trial experience with butorphanol nasal spray in patients with migraine was limited at the time the drug was approved for marketing. It is clear that both the company and regulatory authorities believed that evidence gained with parenteral formulations of the drug for a variety of pain states was directly applicable to its use in other formulations for the specific disorder of migraine. This belief has been proved wrong by subsequent events. Additionally, it is remarkable that a new formulation of a drug which after release was heavily promoted for use in a specific condition (migraine) was studied in only 107 subjects with that disease prior to marketing.
One small study published in 2002 examined the use of butorphanol nasal spray in 83 patients attending a headache clinic. Eighteen (22%) had ‘overused or become inappropriately dependent on’ butorphanol nasal spray. These patients were more likely than others in the study to have additional diagnoses of anxiety or depression, suggesting that there may be a subpopulation of patients with affective disorders who are at higher risk of dependence. This study also provided information on the extent of overuse encountered in some patients, with a report that ‘while most patients in the study used one or two bottles of butorphanol nasal spray per month, 10 patients utilized 15 or more bottles on a monthly basis’. (A bottle is estimated to contain up to 18 sprays, depending upon evaporation and the amount of medication wasted by priming.)
Initial marketing efforts
Butorphanol nasal spray was heavily promoted by the manufacturer. Messages emphasized the low abuse potential of the drug and downplayed the risks of addiction. One physician commented on the ‘unprecedented media blitz’ of publicity about the drug, resulting in ‘hundreds of patients asking me about this “new treatment for migraine”’. (30) Paradoxically, marketing messages suggesting that the drug had a lower likelihood of abuse compared with other opioids may have inadvertently led to its prescription for patients at risk of substance abuse by doctors hoping to lessen that risk, and contributed to the rapid development of dependence problems. One subsequent lawsuit accused the manufacturer of fraud, negligence, civil conspiracy and racketeering for providing false and misleading information to the FDA to win approval for butorphanol nasal spray. This, according to the plaintiff, ‘left consumers and doctors … unaware of its real danger’ (31). Another lawsuit alleged negligent misrepresentation stemming from ‘defendant's failure to warn that its nasal spray product was addictive’. The plaintiff sought to certify a class action and to establish a medical monitoring programme to identify nasal spray users addicted to the drug. The court held that although the plaintiff was a proper class representative, the case would not be certified as a class action because individual issues of addiction and the fact that the suit sought primarily monetary damages overwhelmed common issues in the case (32).
The manufacturer of butorphanol nasal spray now promotes the drug as ‘rescue’ therapy for migraine attacks that have failed to respond to other abortive agents (33). In addition, the labelling for butorphanol has been amended. It includes information from one controlled clinical trial of patients receiving butorphanol nasal spray for non-malignant chronic pain for 6 months, in which 2.9% of the patients were reported to be overusing the drug (suggestive of tolerance and perhaps addiction), while none of those receiving placebo developed such a pattern of overuse. In addition, withdrawal symptoms were reported in 2.6% of patients receiving butorphanol nasal spray and none of those receiving placebo. The label also indicates that ‘butorphanol is one of a class of drugs known to be abused and should be handled accordingly’ (34). Whether this label change along with changes in the company's promotion strategy for the drug will have the desired effects remains to be seen.
Lessons for the future
The lessons learned from the butorphanol nasal spray episode have important implications for future evaluation of headache drugs. First, it is important to avoid a false sense of security about a drug based on its safety record in treating pain conditions other than migraine. Butorphanol nasal spray worked well for acute, self-limited pain problems such as dental or postoperative pain, but no one foresaw the problems it would cause when used for acute episodes of a chronic pain condition like migraine. Additionally, early reports of problems with a medication, especially when received from experts who treat many migraine patients, should be investigated vigorously and viewed as an important, early signal of potential problems that were not identified in clinical trials.
Second, information about the safety and tolerability of other formulations of a new drug, or drugs that have similar side-effects, should be carefully considered in determining approval of a new formulation. The dependence and addiction problems that surfaced when butorphanol nasal spray became widely available for self-administration might have been anticipated if the record of other drugs with psychoactive properties used in migraine had been reviewed (such as the butalbital compounds.) Additionally, the ease with which butorphanol nasal spray could be administered compared with previous injectable versions probably contributed to the rapid development of addiction. Thus, the effect of route of administration should be very carefully considered.
Third, clinical trials of abortive migraine treatments should extend long enough not only to establish efficacy and tolerability in a single attack, but also to identify any long-term effects of repeated use. The clinical trial population should be similar to the population of patients who can reasonably be expected to use the drug. In the case of migraine, that means reconsidering the usual practice of excluding severely disabled subjects from clinical trials of abortive medications, or requiring post-marketing surveillance in this group. Such patients are the ones most likely to use any new drug approved for migraine, and to use it often. Finally, promotional efforts for new drugs should not suggest or imply that a new drug may be ‘less likely’ than others in its class to cause a particular adverse event, unless there is evidence from extensive post-marketing use that this is true. Such suggestions can have the unintended effect of encouraging the prescription of the new drug to patients at high risk for such adverse events, paradoxically increasing the chance that the problem will occur.
Applying previous experience
A number of examples from the headache field suggest that the lessons of the butorphanol nasal spray episode have not been fully absorbed. For instance, oral transmucosal fentanyl citrate (OTFC), a mu-agonist opioid, has recently been advocated as rescue treatment for migraine attacks that do not respond to first-line therapy such as the triptans (35–37). However, a black box warning in the prescribing information for this drug states that the product is ‘indicated only for the management of breakthrough cancer pain in patients with malignancies who are already receiving and who are tolerant to opioid therapy for their underlying persistent cancer pain … it is contraindicated in the management of acute or postoperative pain … and must not be used in opioid nontolerant patients …’ (38). Despite this, a continuing medical education monograph sponsored by a grant from the manufacturer of OTFC recently extolled the benefits of this ‘raspberry-flavored lozenge attached to a handle’ as something that ‘may offer hope for sufferers of acute migraine who cannot use or do not respond to the triptans’ (39). Articles discussing the use of OTFC for rescue treatment of migraine have begun to appear in ‘throwaway’ medical journals sent to physicians (40). Based on experience with butorphanol nasal spray, it is not difficult to anticipate that widespread out-patient use of OTFC for migraine could prove disastrous. Despite the undoubtedly good intentions of advocates of this form of treatment, and an undisputed clinical need for effective migraine rescue therapy, the potential for misuse, diversion, unintentional overdose and addiction posed by OTFC seems unacceptably high. Furthermore, the occurrence of such problems can be predicted with reasonable certainty on the basis of past similar experience with butorphanol nasal spray. A false sense of security about the use of OTFC in migraine based on its safety in treating breakthrough cancer pain should be avoided, and the consequences of providing a formulation of fentanyl that can be easily administered without direct medical supervision should be carefully considered. Use of the drug for rescue treatment of migraine should be delayed until long-term, formal clinical trials in adequate numbers of migraine patients have occurred that clearly establish its harm-to-benefit ratio when used over a long period of time. Furthermore, patients in these trials should represent the spectrum of migraine sufferers who are likely to be prescribed the drug in actual clinical practice.
Other recent events reinforce the prudence of such an approach. Over the last decade, the use of scheduled, maintenance doses of opioids for the treatment of intractable headache and other non-malignant pain problems has become common, based almost entirely on models of opioid treatment for cancer pain (41). Unfortunately, when subjected to careful evaluation, such use has proved to be of benefit for only a minority of patients with headache (42, 43); meanwhile, mounting evidence implicates regular opioid administration as a factor in the development of worsening pain and neurological toxicity (44, 45). In this case, as with butorphanol nasal spray, a false sense of security about the efficacy and safety of a treatment strategy in headache, based on its favourable risk-to-benefit ratio in other pain conditions, may have contributed to a delay in rigorous evaluation of the evidence for its use in headache. Similar concerns have been raised about tramadol, an analgesic drug whose abuse potential is generally felt to be low, at least when used in other pain conditions (46).
On a positive note, the manufacturers of the seven commercially available triptan medications have been reasonably careful to avoid suggestions that one drug in the class might have a safety advantage over others in the class, at least with respect to cardiovascular events. They appear to recognize that such comparisons, in addition to being scientifically untenable (47), might have the unintended effect of encouraging prescription of their triptan to patients at high risk for coronary events. In the case of butorphanol nasal spray, emphasis on its lower dependence liability compared with other opioids almost certainly contributed to its use in patients for whom physicians otherwise might not have prescribed an opioid.
Conclusions
In discussing the issue of post-marketing drug surveillance, an editorialist in the New England Journal of Medicine has commented that ‘Some adverse events are truly unexpected, whereas others, though previously unrecognized, cannot be described as wholly unexpected … we need to take a more aggressive approach to the postmarketing surveillance of new drugs, particularly if there is some a priori reason to suspect that they may have adverse effects … when the index of suspicion is sufficiently high, postmarketing surveillance should be made a condition of drug approval …’ (48). In addition to the efforts of regulatory bodies such as the FDA to ensure improved drug safety, physicians involved in the day-to-day care of headache patients, and those who participate in the design and execution of clinical trials, should increase their vigilance for unintended effects of drugs that are predictable on the basis of previous experience. The history of drug development in general, and in the migraine field in particular, suggests that situations similar to those reviewed in this review will inevitably occur in the future. By collecting, analysing, publicizing and applying the lessons of previous experiences, we can decrease the chance that we will repeat the mistakes of the past.