
Abstract
Background
Many risk factors have been associated with migraine progression, including insufficient and ineffective utilization of migraine medications; however, they have been inadequately explored. This has resulted in suboptimal usage of medications without effective altering of prescribing recommendations for patients, posing a risk for migraine chronification.
Methods
Our aim is to conduct a comprehensive review of the available evidence regarding the underuse of migraine medications, both acute and preventive. The term “underuse” includes, but is not limited to: (1) ineffective use of appropriate and inappropriate medication; (2) underutilization; (3) inappropriate timing of usage; and (4) patient dissatisfaction with medication.
Results
The underuse of both acute and preventive medications has been shown to contribute to the progression of migraine. In terms of acute medication, chronification occurs as a result of insufficient drug use, including failure of the prescriber to select the appropriate type based on pain intensity and disability, patients taking medication too late (more than 60 minutes after the onset or after central sensitization has occurred as evidenced by allodynia), and discontinuation because of lack of effect or intolerable side effects. The underlying cause of inadequate effectiveness of acute medication lies in its inability to halt the propagation of peripheral activation to central sensitization in a timely manner. For oral and injectable preventive migraine medications, insufficient efficacy and intolerable side effects have led to poor adherence and discontinuation with subsequent progression of migraine. The underlying pathophysiology here is rooted in the repetitive stimulation of afferent sensory pain fibers, followed by ascending brainstem pain pathways plus dysfunction of the endogenous descending brainstem pain inhibitory pathway. Although anti-calcitonin gene-related peptide (CGRP) medications partially address pain caused by the above factors, including decreased efficacy and tolerability from conventional therapy, some patients do not respond well to this treatment. Research suggests that initiating preventive anti-CGRP treatment at an early stage (during low frequency episodic migraine attacks) is more beneficial than commencing it during high frequency episodic attacks or when chronic migraine has begun.
Conclusions
The term “medication underuse” is underrecognized, but it holds significant importance. Optimal usage of acute care and preventive migraine medications could potentially prevent migraine chronification and improve the treatment of migraine attacks.
Introduction
Headache chronification has long led to the increased intensity and duration of headache pain and significant burden in headache disorders, especially migraine. Research has found that chronic headache disorders are associated with substantially greater burden of disease, increased psychiatric and other comorbidity, elevated overall costs and healthcare consumption, when compared with various episodic forms of headache (1,2). This has led to numerous reviews on how to prevent the ongoing progression of these headache disorders (3–5). Currently, multiple risk factors have been identified and can be categorized into modifiable and non-modifiable causes. Non-modifiable risk factors include sociodemographic data such as sex, age and race. By contrast, modifiable causes represent the primary targets for intervention and encompass headache features and frequency, consumption of specific food and drink, obesity, lack of exercise, inadequate sleep patterns, and overuse of acute care medication (6,7). Acute care medication usage has been an area of interest in the progression of headaches, particularly medication overuse headache (MOH) (8–11).
MOH occurs when patients with preexisting headache disorders over-consume acute care medications for ≥3 months for a specified number of days per month depending on the medication, eventually leading to the chronification of headache and decreased responsiveness of acute care medications. This has been a growing subject of interest, especially in developing countries and countries where over-the-counter medications and even prescription medications are easily accessible (12–14). By contrast, a less frequently discussed, but highly significant phenomenon, has been described in the literature: insufficient use of effective medication. Inadequate medication use plays a major role in the development of increased headache frequency, often leading to overuse of medication, which can lead to headache progression (15). In this review, we will be using the term medication underuse headache (MUH) in contrast to the well-known term MOH to highlight how insufficient or inadequate medication may lead to a progressive headache. It is essential to note that MUH is not a newly coined term because this terminology and type of headache does not currently exist but rather represents a conceptual development toward chronic headache that is not well understood. Additionally, given the broad spectrum of headache disorders, our focus will mainly be on migraine, which is the headache disorder most often associated with MOH. The aim of this review is to explore how insufficient or underutilized effective medication, or long-term inadequate response to any medication, may contribute to the progression of migraine, whereas optimal effective medication utilization could potentially prevent progression.
The progression of migraine
Migraine is classified into two distinct categories depending on the clinical course; namely, episodic migraine (EM), defined as having fewer than 15 headache days per month, and chronic migraine (CM), characterized by those having 15 or more headache days per month for more than three months. In addition, CM must have at least eight days with the characteristics of migraine features, or the patient considered it a migraine attack and took a migraine specific acute care medication. In addition, both types of migraine share the same features including: (1) at least five migraine attacks lifetime without aura, or two lifetime associated with aura; (2) headache duration of 4–72 hours if untreated; (3) at least two of the following associated pain symptoms: unilateral, pulsating, moderate or severe intensity, or exacerbated by routine physical activity; and (4) at least one of the following symptoms: nausea and/or vomiting or both photophobia and phonophobia (16). Currently, evidence suggest that the formation of CM could not be achieved without having a pre-existing EM, and that is what is seen clinically (17,18). Hence, the primary treatment strategy is to prevent the progression of migraine, which typically chronifies at a rate of 2.5% per year (18,19).
Clinical studies of medication underuse
The subsequent sections of this paper primarily focus on medications aimed to treat migraine progressions. It is crucial to acknowledge that there are several other types of migraine treatment that should also be considered, including non-pharmacological treatments such as lifestyle changes, behavioral medicine techniques, relaxation exercises, mindfulness, yoga, biofeedback training, vitamins, minerals and neuromodulations (20,21). These holistic approaches can often complement medication-based treatments and may offer significant benefits in preventing migraine progression. However, there is a lack of existing information on their underuse, and thus it will not be mentioned in this review.
Acute care (abortive) treatment of migraine
The primary objective of acute care or abortive medication is the cessation of, or decrease in the intensity or duration of, pain during a migraine attack. Its main goal is to stop the pain and thereby prevent the propagation of peripheral sensitization to central sensitization which may also prevent neurogenic inflammation in the dura. The evaluation of the efficacy of acute care treatment often concentrates on the assessment of achieving pain-free status or significant decrease in pain intensity within two hours or other time points (22,23). In this section, we will be focusing on the underuse of acute care therapy. A summary of clinical studies related to the underuse of acute care treatment can be found in Table 1.
Studies related to underuse of acute care medication
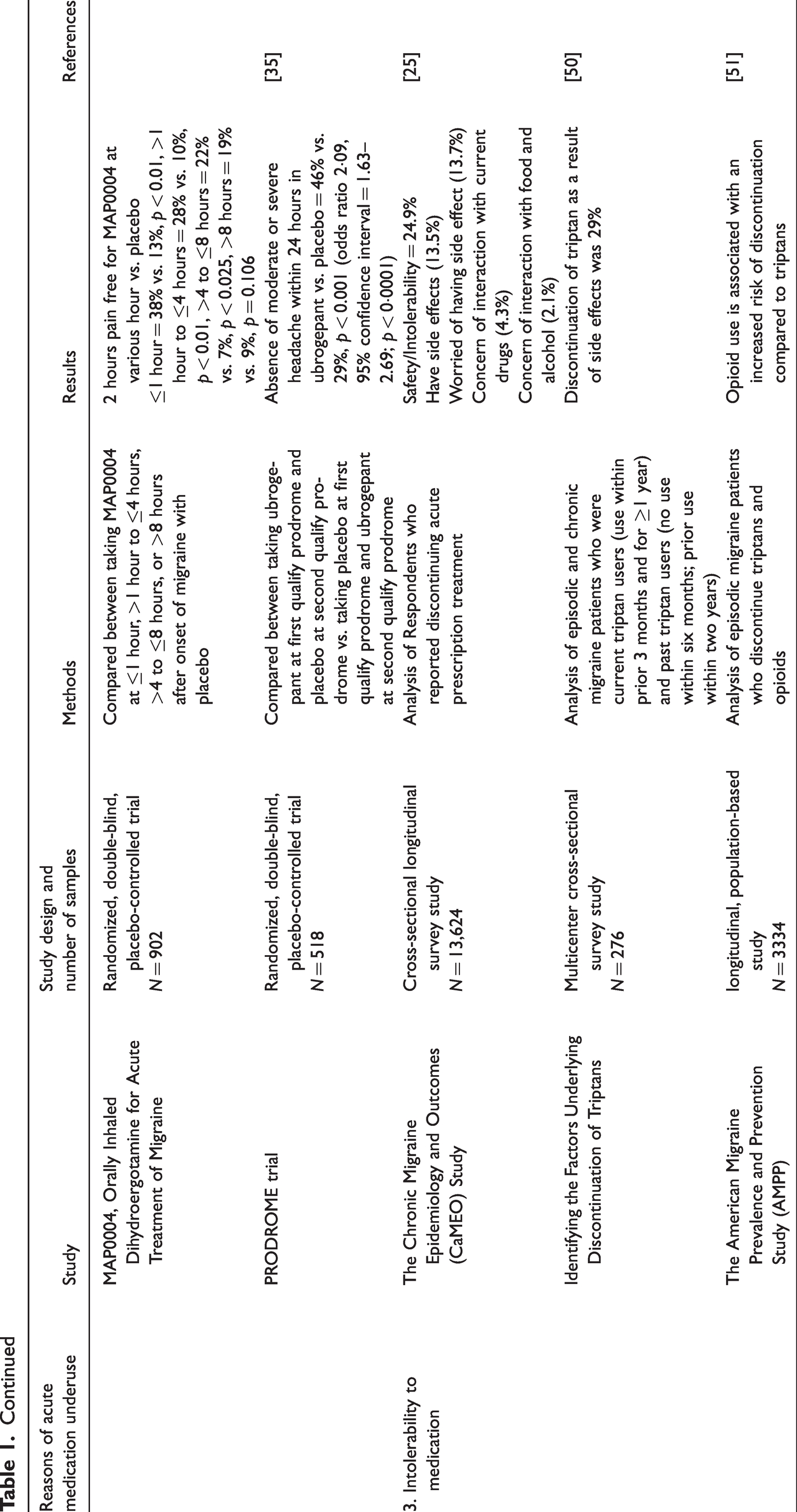
Ineffective acute care treatment of migraine leading to its progression
Studies focusing on ineffective acute care treatment are rare. One such study, the American Migraine Prevalence and Prevention Study (AMPP), found that ineffective abortive treatment was associated with the progression of EM to CM. In this study, treatment efficacy was assessed through the Migraine Treatment Optimization Questionnaire (mTOQ-4) (24). Subsequently, these responses were categorized into four groups: very poor, poor, moderate and maximal treatment response. The results revealed conversion rates to CM in the following year as 6.8, 4.4, 2.7 and 1.9%, respectively. Following adjustment, it was observed that poor treatment efficacy exhibited an odds ratio of 2.17 (95% confidence interval = 1.36–3.44), whereas very poor treatment demonstrated an odds ratio of 3.39 (95% confidence interval = 1.98–5.80) in the development of CM (15). This implies that suboptimal acute care treatment could lead to migraine chronification. Moreover, adequate treatment demonstrated a lower conversion rate compared to the typical progression rate of migraine. Interestingly, triptan usage was more prevalent in the maximal treatment group, whereas simple analgesics were more commonly used in the poor response groups. This finding holds significance in the selection of acute care medication.
In a Japanese Adelphi Migraine Disease Specific Programme, a cross-sectional survey study specifically looking at inefficacy of triptans, revealed that patients with triptan unresponsiveness have more frequent headache days per month (mean 5.7 vs. 4.5; p = 0.023) and migraine headache days per month (4.8 vs. 3.7; p = 0.013) than triptan responsive patients (25). This was a cross-sectional study and could not be a predictor of migraine progression; however, we cannot deny the association between higher frequency days and lack of responsiveness to acute care medication. A cross-sectional analysis of The Chronic Migraine Epidemiology and Outcomes (CaMEO) Study found that a subgroup of patients who did not use acute care medication and patients who discontinued acute care medication have severe migraine-related disability, at 14.4% and 23.2%, respectively (26). Despite being cross-sectional, these results hold significance, highlighting the unmet needs in acute care medication. A subsequent analysis of this study revealed that patients discontinued medication because of poor efficacy and intolerable side effects. Moreover, almost half of the patients experienced moderate to severe disability (27). Hence, poor efficacy of acute care migraine medication may contribute to the ongoing disability of the patient and perpetuate the progression of migraine.
Improper timing of administration of acute care treatment of migraine
The perfect timing of administration of acute care medication has longed been debated regarding whether it be taken at moderate pain intensity or at the very onset of headache (28). Those investigators who advocate taking medication during the attack consider that assessing accurate headache features can help avoid unnecessary medication usage; however, those who favor medication at the very onset of pain consider that it offers higher efficacy. At the very start of the triptan era, most trials administered triptans when the headache was of moderate or severe intensity, as required by the Food and Drug Administration to ensure that it was a migraine attack. Compared with a placebo, they were proven effective measuring pain relief (29–31). Later studies shifted the focus to an earlier approach, giving triptans before one hour, when the pain was milder, yielding findings that suggested that patients had better pain relief at two hours than waiting for moderate to severe pain.
In the TEMPO study conducted by a French group, a comparison between early dosers (<1 hour from headache onset) and late dosers (>1 hour from headache onset) revealed that patients in the early doser group had higher rates of pain relief than those in the late doser group (52.8% vs. 32%, p ≤ 0.01) (32). Another double-blind, placebo-controlled trial of almotriptan also found that treating when the pain is mild and within one hour of pain onset compared to treating when the pain is moderate to severe, showed a greater rate of response (53% vs. 38%, p = 0.03) (33). Numerous studies have shown similar results (34–36). Furthermore, a study that administered ubrogepant during the prodrome phase (prior to the start of headache in patients who could accurately predict the onset of migraine headache most of the time) revealed that within 24 hours, moderate or severe pain did not occur for 46% of participants, compared to 29% in the placebo group (p ≤ 0.01) (37). In that situation, it can be predicted that early administration of acute care medication could be important in suppressing the progression of the sensitization in the trigeminovascular pathway and preventing the progression of the migraine attack to include central sensitization (38).
The development of cutaneous allodynia has been shown to be a predictor of treatment response. The results from the AMPP study have shown that cutaneous allodynia was a significant predictor of inadequate acute treatment for pain-free at two hours, pain relief response at 24 hours and sustained pain-free response at 24 hours (39,40). This could be interpreted as suggesting that allowing a severe headache to develop into cutaneous allodynia could result in inadequate pain relief. Another concerning topic is whether taking medication early, before the headache is well formed, leads to MOH in some patients with frequent headache. Studies have found that some patients tend to overconsume triptans by taking them for mild headache attacks when they may not be needed (41). A study indicates that it would take over 12 days of triptan use per month to cause chronification of migraine (19). The International Classification of Headache Disorders, 3rd edition (ICHD-3) defines MOH as the use of a triptan and other medications like ergots and opioids for 10 days per month for three months (16). Therefore, patients should always be advised of the limits of these medications; however, although the ICHD-3 is the best classification we have today around the world, the limitation of medication amounts for each individual has not been studied and may vary. Additionally, headache recurrence is usually defined as worsening or recurrence of headache within 24 or 48 hours after the resolution of pain at two hours after taking a medication. Even though the product information of each triptan tablet suggests repeating the dose in two hours for lack of improvement, patients should always be cautioned that re-taking the same medication for a recurrent headache might not be effective (42). Studies have found that the prevalence of recurrence in migraine patients is 15–40% in triptans users (43); however, a change to another triptan or to an effective non-steroidal anti-inflammatory drug such as naproxen sodium might be beneficial (44,45). Therefore, this unmet need should be evaluated frequently at the start and a new strategy might be needed in subsequent visits or office contact until the optimal treatment is reached.
In our opinion, if a patient has multiple days of headache per week, but is not sure which one will progress to a migraine attack that could be treated by a triptan or gepant, the patient should wait and see if the headache begins to progress in intensity with unilateral throbbing and associated symptoms. As soon as it does, and the patient believes it will progress to a migraine attack, this is the optimal time to take their medication and try to avoid MOH. However, this dose should be taken within the one-hour period. Additionally, there should be a limitation on the number of acute medications prescribed to an average of two days per week for most acute care medication, other than gepants (46).
Currently, which care plan is best for the for the migraine patient is still a subject of debate. In the disability in the strategies of care (DISC) study, conducted many years ago, 835 migraine patients were stratified into three groups: stratified care, step care within attacks and step care across attacks. Patients in the stratified care group received acute care medication based on their Migraine Disability Assessment (MIDAS) score (MIDAS I and II received aspirin plus metoclopramide; MIDAS III and IV received oral zolmitriptan). In the step care within attacks group, patients received aspirin plus metoclopramide for all attacks; however, if the pain did not subside within two hours, they were given zolmitriptan 2.5 mg. Patients in the step care across attack group received aspirin and metoclopramide for the first three attacks. If the pain did not reduce from severe to mild or no pain in at least two of three attacks, an escalation to zolmitriptan was recommended for the rest of the attacks. The study revealed that patients in the stratified care group showed a greater two-hour headache response compared to those in the step care within attacks and step care across attacks groups (52.7%, 40.6% and 36.4%, respectively, p ≤ 0.001) (47). Note that the stratified group had more side-effects. A further economic analysis on the DISC study showed that, although the mean total cost per attack was the highest in the stratified group (with a mean over six attacks of £28.25 compared to £11.74 and £23.15 in the stepped care across attacks group and within attacks group, respectively), when combined with productivity costs, the stratified group exhibited a lower total cost than the other two groups. However, this difference did not reach statistical significance (48). Another study showed similar results (49). This strategy was incorporated into the American Headache Consensus Statement (50). By contrast, the European Headache Federation guideline recommends the use of stepped treatment approach (treatment ladder). Starting from basic analgesics, then escalating the treatment to the next level after three attacks of migraine. The guideline stated that it is the most effective and cost-effective individualized care (51,52). In our opinion, even though the above method may be less expensive, selecting medication should be tailored according to each individual regarding the intensity of the pain and severity of each attack according to associated symptoms, patient preferences, side effects and contraindications. Caution should be exercised when following rigid steps, whereas adaptation, when necessary, is encouraged. This approach aims to prevent the underuse of acute care medication. Making a patient wait for a revisit for many weeks later to advance failed treatment is not usually the best way to treat patients, even if it is less expensive.
Intolerability to acute care medication for migraine
Other factors leading to the underuse of acute medication are side-effects and intolerability to treatment. Regarding the Chronic Migraine Epidemiology and Outcomes (CAMEO) study, it was found that discontinuation of medication as a result of intolerability occurred in 24.9% (53). This number is as high as lack of efficacy to acute care medication; furthermore, tolerability was shown to be one of the factors causing switching or discontinuation of acute care medication in several studies (54,55). In a systematic review and meta-analysis including 97 randomized control trials, it was found that gepants (small molecule calcitonin gene-related peptide receptor antagonists), lasmiditan (5-HT1F receptor agonist), dihydroergotamine, ergotamine plus caffeine, acetaminophen, antiemetics, butorphanol and tramadol in combination with acetaminophen, all have increased side effects compared to placebo (56). Providing education, selecting medication based on patient preferences and avoiding side-effects would increase the adherence of medication in order to prevent further migraine progression (53).
Traditional oral preventive medications
The goal of preventive medications is primarily to decrease the frequency of migraine attacks; it is not usually used for rapid cessation of pain and should not be confused with acute care treatment. Its main objective is to decrease the hyperexcitability of the pain pathway, resulting in continued improvement in headache frequency and other parameters over time (57). Therefore, the clinical indicators used to interpret patient improvement are decreased migraine and headache days per month, as well as decreased pain intensity and duration (58). Moreover, interictal pain burden has been identified as an indicator of migraine disability, and preventive medication plays a crucial role in alleviating these symptoms (59,60). Also, if the above occurs, there will be a decrease in headache burden, disability and an improvement in overall quality of life (61,62). Here, we will discuss the epidemiology of preventive medication underuse, discontinuation and the reason behind it.
Underuse of preventive medication
Epidemiological studies on the underuse of preventive medication have been well studied. A US study found that, among enrolled patients, 38.8% of the participants were eligible for preventive medications; however, only 12.4% were using them (63). A Portuguese based studied found that, among eligible patients for migraine prevention, only 22% were taking them (64). Note that these studies were conducted in a headache center, where the doctors are more likely to use optimal treatment. A large cohort study (the ObserVational survey of the Epidemiology, tReatment and Care Of MigrainE (Europe) (OVERCOME [EU]), found that 73.9% of the patients who were eligible for the use of preventive medication were not using it (65). The prospective cohort Assessment of Tolerability and Effectiveness in Migraine Patients using Preventive Treatment (ATTAIN) study, found that prior to the introduction of anti-calcitonin gene-related peptide (CGRP) preventive therapy, despite high burden and frequent headache days, 70.1% of patients had been treatment naïve (66). In a study at an emergency department, half of the patient included in the study had more than seven migraine days per month; however, only 5% were already on preventive medication (67). Based on these studies, there is certainly confirmation that doctors are under-prescribing preventive medication, and this will probably lead to migraine chronification. Further exploration of this issue suggests the need for increased education among doctors about the benefits of preventive medication to instill greater confidence in its use.
Discontinuation of preventive medication
Discontinuation has led to underuse of preventive medication, in addition to patient drop-outs and those lost to follow-up. What we have to accept is that older, oral preventive medications are not designed specifically for the preventive treatment of migraine, but rather to treat hypertension, heart disease, epilepsy and depression, amongst other diseases. This should also be discussed with the patient so they have a better understanding of what outcomes to expect. It may well take two to three months to have therapeutic blood levels and good efficacy and patients may have some tolerability issues. A retrospective analysis on the adherence of oral preventive medication showed it to be between 26% and 29% at 6 months and between 17% and 20% at 12 months, respectively. This study focused on 14 different medications which could be classified into three major categories: antidepressants, antihypertensives and anticonvulsants. Among all of the preventive medications included in the study, the percentage of discontinuation was similar among groups (68). Other studies show similar results (69,70). Therefore, drug classes in the usage of migraine prevention might not be significantly superior to one another; however, a Canadian study found that angiotensin receptor blockers and anti-CGRP medications have higher adherence rates (70). This might be because these newer medications have fewer side effects and may be more effective in some patients. We will be discussing anti-CGRP methodologies below.
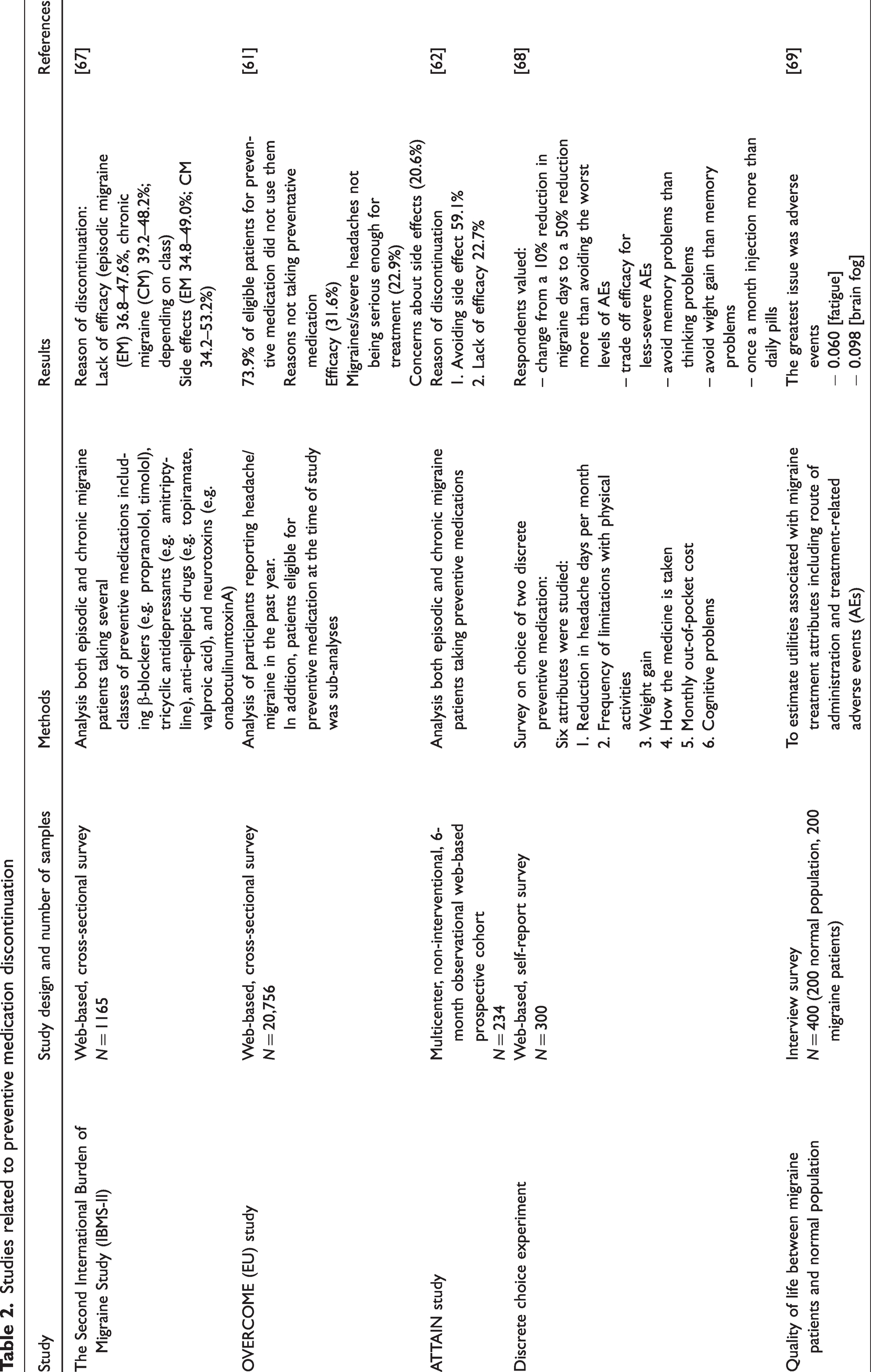
The primary reasons for discontinuing preventive medication have been identified as lack of efficacy and too many side effects. The Second International Burden of Migraine Study (IBMS-II) found that lack of efficacy was the reason for discontinuation in 36.8–47.6% in EM patients and 39.2–48.2% in CM patients, whereas side effects were found to be the issue in 34.8–49.0% of EM patients and in 34.2–53.2% of CM patients, respectively (71). The OVERCOME [EU] study found that 66.8% of the patients were dissatisfied with their current treatment (65). In addition, the ATTAIN study showed that side effects was the most common reason for dissatisfaction, followed by lack of efficacy (66). Table 2 summarize studies related to the discontinuation of preventive medications.
Studies related to preventive medication discontinuation
Exploring patient satisfaction of preventive medication
Patient satisfaction is difficult to define. In this section, we will explore the possible reasons for patients’ satisfaction. The OVERCOME [EU] study found that only 33.2% of those who were using preventive medication were satisfied with it. Although the study did not mention the reason behind the satisfaction or lack of it, it provides a wider picture of the unmet need in migraine prevention (65). In a discrete choice experiment, 300 participants were invited to participate in a survey. Patients had to answer questions about six attributes, each with three levels. Reduction in headache days per month (10, 25 or 50%), frequency of limitations with physical activities (none, one-category improvement or two-category improvement), cognitive problems (no problems, thinking problems or memory problems), weight gain (none, 5% body weight gain or 10% body weight gain), route of administration (daily oral pill, once-monthly injection or twice-monthly injection) and monthly out-of-pocket cost ($5, $60 or $175). The results showed that participants valued efficacy more than decreased adverse events; however, patients were willing to trade off efficacy if there were severe adverse events. Interestingly, patients were more concerned about weight gain than cognitive or memory problems (72). In other words, when considering preventive medication, efficacy might have been their first priority; however, certain side effects were also considered, especially weight gain. Another study revealed that the most problematic issue in oral medication was adverse effects (73).
Pathophysiology of migraine progression as a result of medication underuse
When considering the transformation of migraine, the exact pathophysiology remains unknown; however, established observations suggest two main underlying foundations. The first is the activation of the ascending pathway, wherein prolonged stimulation of the trigeminovascular pathway by inflammatory substances could lead to hypersensitization and a lack of habituation. Later, prolonged inflammation would lead to peripheral sensitization and central sensitization (74). The second involves the deactivation of the brainstem descending endogenous inhibitory pain pathway, resulting in disruption of the brainstem pain modulating system (Figure 1). The combined effect results in alterations in the natural course of the disease (9,75–80). Therefore, medication underuse should affect either or both of these pathways.
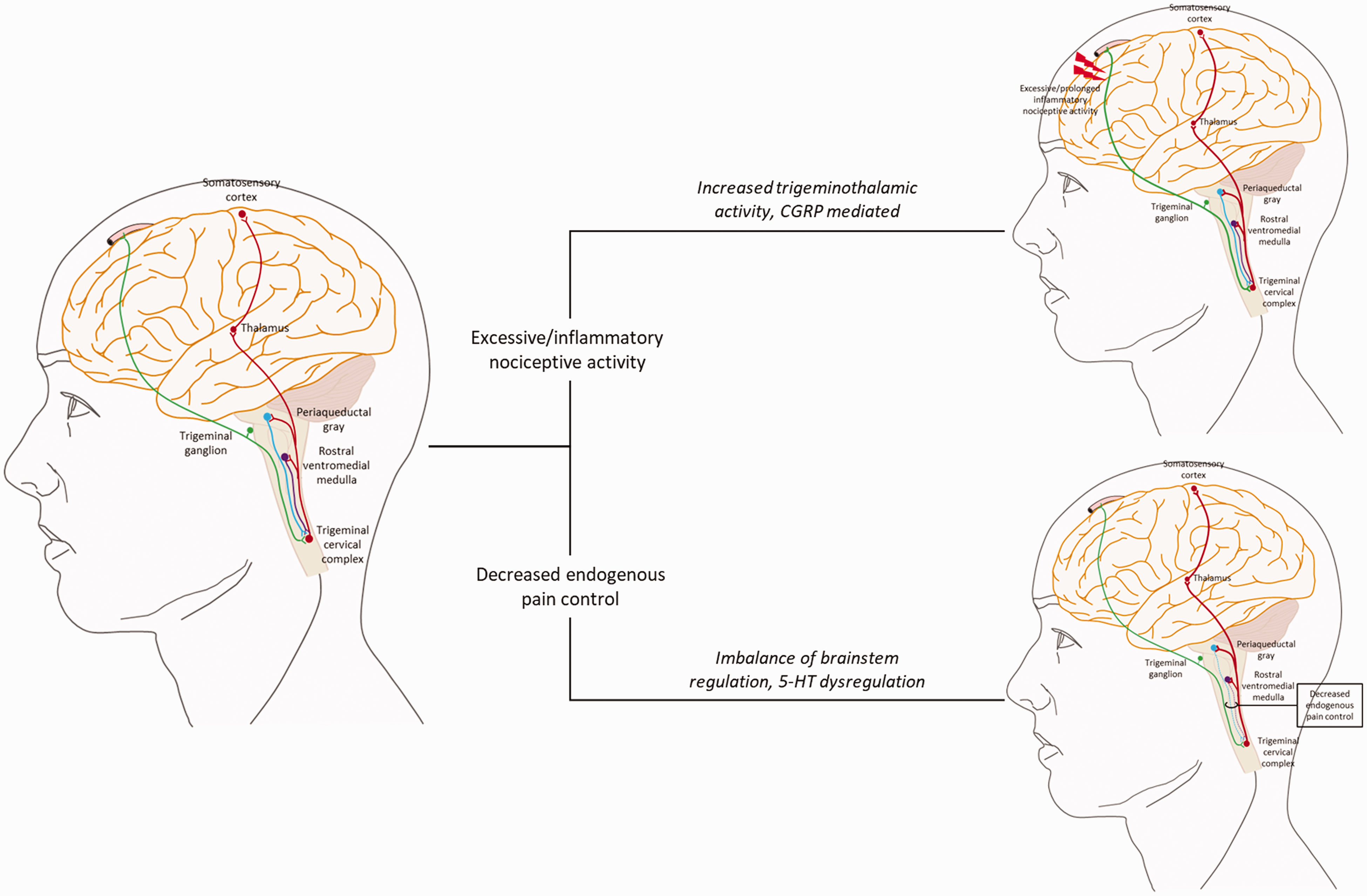
Migraine chronification is caused by two main pathways: 1. Ascending pathway (Prolonged inflammation and disruption of serotonergic brainstem neurons). 2. Descending pathway (Decreased endogenous pain control).
Repetitive and prolonged nociception in the activation of ascending pathway
Currently, we understand that hypothalamic dysfunction may be responsible for the initiation of migraine symptoms, particularly in the premonitory phase (81,82). However, the trigeminovascular system plays a pivotal role in migraine pain (83,84). The initiation of a migraine pain involves the activation of nociceptive inputs in sensory afferent nerves, specifically targeting the peripheral c-fibers and Aδ fibers of the trigeminal nerves located in the cerebral arteries and connecting the meninges with the pons and the trigeminal nucleus caudalis (85). These fibers are known to express various substances such as CGRP, vasoactive intestinal peptide, neuronal nitric oxide synthase and substance P (86). Subsequently, these signals progress through the trigeminal ganglion before projecting into the trigeminal nucleus caudalis as part of the trigeminocervical complex, marking the inception of the system's central nervous system phase. The second-order neurons extend from the trigeminal nucleus and project to the ventroposteromedial nucleus and the medial nucleus of the posterior complex of the thalamus, ultimately connecting with multiple cortical regions (83,85).
The pivotal process within the ascending brain stem pathway is termed chronic sustained neurogenic inflammation (87,88). It is assumed that prolonged inflammation affects multiple receptors and disrupts the trigeminovascular system, leading to peripheral sensitization followed by central sensitization. In vivo studies have demonstrated that inflammation of the dura mater can chronically activate the trigeminovascular pathway (89). This is evident through the overexpression of phospho extracellular signal regulated kinase 1/2, interleukin-1β and CGRP-positive nerve fibers within the trigeminal ganglion (90). In a human study, interictal CGRP levels of EM patients and CM patients were statistically different (33.74 ± 16.10 pg/ml vs. 74.90 ± 28.29 pg/ml; p ≤ 0.001) (91). This evidence supports the idea that a more sustained inflammation is seen in CM and could also lead to chronicity. Additionally, the prolonged and sustained activation of the trigeminovascular pathway during attacks could potentially lead to central sensitization (5). This suggests that the failure to stop the pain during an attack might result in a continuous release of inflammatory markers. Consequently, if this cycle repeats multiple times, it could contribute to the progression and chronicfication of migraine. In addition to CGRP, vasoactive intestinal peptide and other neuroinflammatory markers have displayed similar outcomes (92,93).
Central sensitization emerges as a subsequent development following prolonged inflammation, often triggered by the activation of second and third-order neurons (94). Glutamate receptors (AMPA and NMDA) are assumed to play a significant role in central sensitization (95). Clinically, manifestations may include either hyperalgesia or allodynia. This suggests that allodynia is a marker for central sensitization (96). Moreover, the presence of widespread and progressive allodynia might signal the onset of chronicity (97). Consequently, the treatment strategy involves interrupting or preventing allodynia to deter the progression of central sensitization.
Dysregulation of the endogenous brain stem descending central pain modulating network
The descending central pain modulating network, involving serotonin and norepinephrine, is located in the areas of the periaqueductal grey and the rostral ventromedial medulla (6,98,99). Normally these nuclei act as a gateway to alter pain before its interpretation in the cerebral cortex. On the other hand, dysfunction in these areas cause hyperalgesia and allodynia. In other words, it is a co-facilitator in central sensitization. Basic science has shown that the system’s malfunction is caused by oxidative stress and dysregulation of the serotonergic neurons (100–102). Numerous studies have pointed out that medication overuse is the main contributor to dysregulation of this pathway (9,103–106). On the other hand, as a result of limited data, medication underuse is still uncertain.
Migraine medication to the rescue
As mentioned earlier, the primary goal of acute care medication is to alleviate pain as quickly as possible and certainly within a two-hour window (22,23). This is crucial because pain cessation implies potential diminishment of inflammation and deactivation of the trigeminovascular pathway. It also improves the chance that the attack will not persist or recur. A thorough study using cutaneous allodynia as an outcome showed interesting insights into stopping the activity of the trigeminovascular pathway. The study measured pain at baseline and followed the subject every hour. At one hour, allodynia develops on the ipsilateral side of the head as well as the throbbing headache; at two hours, allodynia spreads to the contralateral side of the head and ipsilateral arm. Finally, at four hours, allodynia becomes more prominent, but without further spread (107). This suggests that, within the first hour, peripheral nociception has been activated. At one hour, the peripheral nociception could mediate activation of the second order neuron within the trigeminal nucleus caudalis (108,109). Later, after two hours, progression to the third order neuron in the thalamus occurs with activation, causing widespread allodynia (Figure 2). This holds immense importance in determining the appropriate timing for pain termination. To support this idea, both animal and human models have been established. In a rat model, a single unit recording was placed on the spinal trigeminal neurons to receive input from dura and facial areas. Sumatriptan was given at the same time with inflammatory soup (IS) (to induce pain in the rat) or two hours after the application of IS. The results show that early administration of sumatriptan could block all aspects of central sensitization; late intervention could block the progression of receptive fields and increase the dural activation threshold. This could be interpreted as: early intervention can be beneficial in blocking the progression of pain. Although late intervention did not show similar results, it is better than not taking anything at all for the pain (38). The results of a human study by the same group found that when administration of sumatriptan occurs in a patient with or without allodynia, the percentage of response was 15% and 93%, respectively. Treating at one hour vs. four hours was equally ineffective in patients with allodynia and equally effective in patients without allodynia. This has provided even further insights suggesting that early administration of acute care medications might be crucial before the development of allodynia (110).
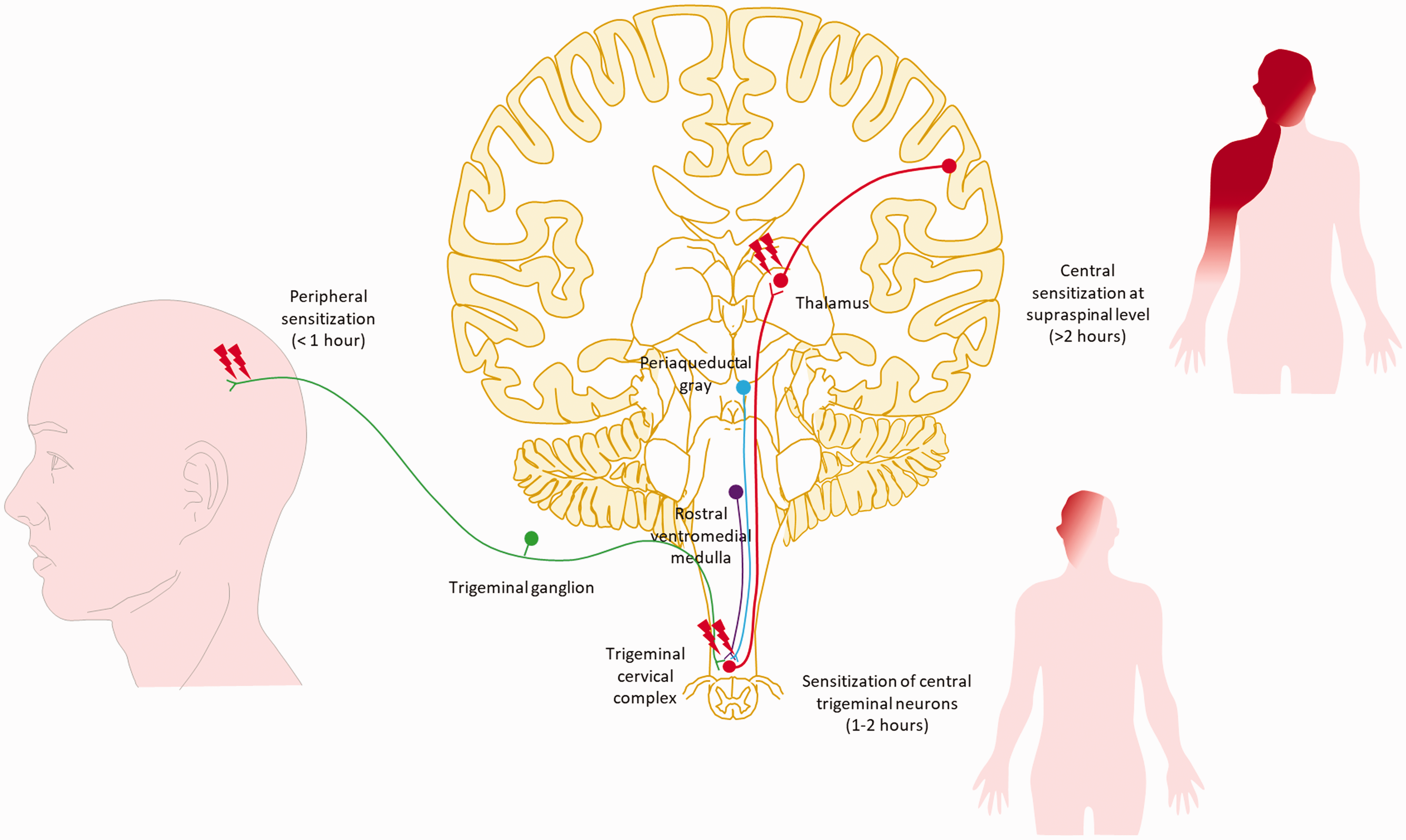
Demonstration of the activation of the trigeminovascular pathway. In the initial hour of the attack, activation primarily occurs within peripheral sites, leading to ipsilateral throbbing pain. By the one-hour mark, the signal extends to the second-order neuron within the trigeminal cervical complex, marking the beginning of the central portion of the system. This results in allodynia on the ipsilateral side of the headache. Beyond two hours, the activation propagates to the third-order neuron in the thalamus and subsequent cortical areas, leading to the propagation of allodynia to the contralateral head and ipsilateral arm.107,110
Activity dependent and activity independent processes in central sensitization
Regarding the above section, we can interpret these findings as though there are two main processes occurring. The first process involves early administration of acute care medication terminating the pain, whereas the second process involves late administration of the medication that cannot resolve the pain. This has been demonstrated in a rat model showing that, once there is induction of the second order neuron, lidocaine can terminate the input from the dura (111). This is a process called activity dependent. On the other hand, once central sensitization is fully established, lidocaine cannot block the ongoing input, which is now activity independent (112,113). The activity dependent process is found to be a result of glutamate and a neuromodulator such as CGRP or substance P inducing multiple intracellular pathways in the dorsal horn (85). For the activity independent process, it develops slowly and is maintained for a certain period of time. The underlying substrates are similar to activity dependent but with more production of cytokines (114). Further studies have found that the activity independent process can lead to migraine progression (85,115).
Pathophysiology summary
In summary, we consider that ascending activity in the trigeminovascular pathways may be the pivotal process contributing to the progression of medication underuse. During acute attacks, administering effective medication early, particularly before the onset of allodynia, is found to be beneficial and can potentially prevent central sensitization. When aiming to prevent the transition to a chronic state, early administration of effective preventive medication, with fewer monthly migraine days, during phases of low inflammatory mediator levels, such as in EM, is more effective than in chronic conditions that have a higher frequency of monthly migraine days.
Anti-CGRP medication and medication underuse
Without a doubt, anti-CGRP treatments demonstrate promising efficacy and tolerability in a significant number of patients in both clinical trials and real-world studies (116–124). Furthermore, comparisons with older oral preventive drugs in real-world studies have revealed favorable results, both in terms of efficacy and tolerability (125,126). This encouraging trend is attributed to the treatments' selectiveness in migraine pathophysiology without producing unfavorable outcomes. However, cost remains a significant issue, especially in the developing world. Consequently, determining the appropriate treatment and its timing, is still a matter of controversy.
To the best of our knowledge, no well-designed study has been established to predict who would respond to anti-CGRP therapy; however, evidence regarding the factors related to treatment responders is accumulating (127). Patients with lower migraine frequency were found to be better responders; in a prospective cohort study, it was found that a lower number of migraine headache days per month was associated with responders at one and six months (p < 0.001) (128). Real-world data on the monoclonal antibody galcanezumab also demonstrate similar results, indicating that the responder group had fewer headache days compared to the non-responder group (24.0 ± 6.4 vs. 26.0 ± 6.2, p ≤ 0.012) (129). When focusing on the comparison between CM and EM, a recent study comparing super responders (SR) and non-responders (NR) found that the percentage of CM in the NR group was higher than in the SR group (92% vs. 52%, p = 0.001) (130). However, in another real-world study using erenumab, it was found that fewer headache days were a good predictor only in the CM group and not in the EM group (131). Although no definitive conclusion has been reached, initiating anti-CGRP treatment when migraine frequency per month is lower may be more beneficial than when it escalates to a higher frequency.
Apart from headache days, the number of prior preventive medications has been shown to be a predictor of poor outcome (132,133); however, it remains unknown whether this ineffectiveness stems from medication resistance or a lack of effectiveness of the older, less migraine specific preventive medications. Notably, many patients had extensive exposure to preventive medications over time before the anti-CGRP era. Besides headache-related factors, non-headache features also contribute significantly. The presence of comorbid depression is linked to a poorer outcome for erenumab (134,135). In addition, a recent study using erenumab and galcanezumab found that persistence of anxiety and depression were associated with lower rate of response at three months and six months (136), whereas a low Headache Impact Test (HIT-6) score was associated with positive results (137).
In conclusion, using effective acute care medication as soon as the migraine attack begins and initiating preventive migraine treatment early, particularly when the headache frequency is low with minimal prior preventive medication use, could offer greater benefits to patients compared to leaving them untreated or poorly treated for extended periods. Furthermore, addressing comorbidities such as depression and anxiety should always be a part of the treatment strategy.
Limitations and future directions
The limitation of this review revolves around the scarcity of research data addressing medication underuse. Despite an exhaustive search across numerous sources, acquiring specific information on the phenomenon of medication underutilization has proven challenging. Although evidence continues to expand on newly approved drugs, there is a lack of guidance on their application or initiation in practice. The difficulty around underuse is the possibility of underlying biological predisposition to higher frequency of attacks in some patients. One might hypothesize that, if we start effective acute care and preventive medication soon enough, this would likely be better for the patient. We strongly consider this to be the case based on the trials cited above and our current clinical knowledge. Therefore, we call for more comprehensive and longitudinal research on the best time of initiation and utilization of these effective anti-CGRP medications and future available targeting therapy such as anti-pituitary adenylate-cyclase-activating polypeptide ligand therapy. Furthermore, educational programs for healthcare providers and patients alike are needed. Exploring innovative treatment strategies, such as telemedicine and digital health tracking interventions, might improve patient physiological data to go along with clinical states as well as outcomes. This could facilitate better patient engagement and improved adherence to medication regimens, resulting in better outcomes such as reduced pain hours per month, less disability, lightened burden of migraine over time and improved quality of life of our patients (138).
Another limitation in this study is its focus on medication alone. Other treatments, such as neuromodulation or behavioral interventions, may also be effective at reducing migraine progression. These modalities would also require further studies on the proper timing of initiation and usage.
Conclusions
In this review, we have highlighted the complicated interplay between medication underuse and the progression of migraine, shedding light on its multifactorial implications. From the inadequate response or timing of acute care therapies to the challenges surrounding underuse and discontinuation of preventive medications, each aspect contributes to the evolving landscape of migraine progression. Understanding the pathophysiological processes involving ascending and descending pain pathways provides a crucial framework by which to comprehend how medication underuse may perpetuate progression and chronicity. Furthermore, insights into the potential benefits of early intervention with both acute care, preventive medication and specifically anti-CGRP treatments would be of importance in the timely and personalized therapeutic strategies. It is crucial to educate both healthcare providers and patients, tailor treatment plans to suit individual needs and emphasize timely interventions.
Clinical implications
Medication underuse, characterized by inadequate, improper or intolerable usage, may lead to migraine progression and chronification. The critical time window for acute care medication intake – within 60 minutes of onset of a migraine attack and/or prior to central sensitization the onset of cutaneous allodynia – is pivotal in preventing the progression of migraine. Educating patients about the efficacy and potential side effects of acute care and preventive medications is imperative. Enhancing awareness could reduce discontinuation rates. Prolonged inflammation and repetitive stimulation of the trigeminovascular ascending pathway might be the key features in migraine progression as a result of medication underuse. While anti-CGRP medications address many aspects of medication underuse, acknowledging non-responders and considering early initiation when headache frequency is lower might significantly improve their efficacy in preventing migraine chronification.
Footnotes
Acknowledgments
We extend our sincere gratitude to Dr Sranya Phaisawang for her invaluable assistance in the construction and language editing of the manuscript submitted for publication. Additionally, we express our appreciation to Dr Charungthai Dejthevaporn and Dr Surat Tanprawate for their ideas regarding this unique and captivating topic.
Author contributions
WR was responsible for study conceptualization, drafting the original manuscript. WR, AS and AR were responsible reviewing and editing.
Declaration of conflicting interests
The authors declare that there are no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
No funding received.