
Abstract
Purpose
Visual snow syndrome comprises a whole-field static-like visual disturbance, with increased awareness of entopic phenomena, an inability to suppress the ‘just seen’ and photophobia. Visual snow syndrome is often associated with other problems such as headache, tinnitus, and anxiety. The earliest reported case of a patient experiencing symptoms consistent with visual snow syndrome dates only to 1995. This paper seeks to find patterns of experience in the medical literature of the past that are reminiscent of visual snow syndrome, to challenge the view that it is in any sense a novel disorder. Descriptions of subjective visual sensations such as experienced by patients suffering from visual snow syndrome were sought in treatises, textbooks and other literature generated by leading figures in 19th-century ophthalmology, physiology and physics.
Conclusion
While retrospective diagnosis of modern illness categories in historical medical literature is an enterprise fraught with pitfalls, it is nonetheless possible to see patterns of experience in the 19th-century medical literature that are strongly reminiscent of visual snow syndrome.
Keywords
Introduction
Visual snow syndrome (VSS) was first formally defined in a paper published in Brain in 2014 (1). The proposed diagnostic criteria outlined a syndrome consisting of a whole-field static-like visual disturbance, with increased awareness of entopic phenomena (floaters, blue field entopic phenomena, photopsias), an inability to suppress the ‘just seen’ (persistence of afterimages or palinopsia, visual trailing), and photophobia. While the diagnostic criteria distinguished VSS from persistent migraine visual aura, it was noted that VSS was commonly co-morbid with migraine, as well as with tinnitus and anxiety (2). Other authors have noted a possible association with tremor (3). Subsequent studies have confirmed the replicability of the diagnostic criteria in larger populations (4). A crowd sourcing internet-based study suggests that as many as 4% of the population may experience visual snow, of whom half may have features of VSS (5).
The earliest case believed to represent VSS that was identified in the 2014 Brain paper was a patient presented in a collection of cases of possible persistent migraine aura, published in 1995 (6). No earlier case has been identified in the literature. This has led to speculation that VSS might in some sense be a disease of modern life. It is potentially of interest, therefore, in regard to this question, to see if one can find precursors of the syndrome in historical literature, especially to clinicians specialiing in headache disorders, to whom these patients often present, in the belief that their symptoms are migraine-related.
Retrospective diagnosis of modern illness categories in historical medical literature is an enterprise fraught with pitfalls, and one that is largely frowned upon by professional historians. Medical terminology changes meaning over time. New technology changes the interpretation of clinical signs and symptoms. Despite this, however, it is sometimes possible to see patterns of experience in medical literature of the past that are strongly reminiscent of modern disease categories, and I will contend that this is the case here. Specifically, I will show how the condition called ‘muscae volitantes’ was initially understood to encompass a set of subjective visual phenomena that resemble the condition now known as visual snow syndrome, before advances in ophthalmological technology led to it being restricted to its modern meaning, simply denoting the presence of floaters; and how, and why, at the same time, the more extended set of visual experiences largely disappeared from the literature.
The origins of ophthalmology
Ophthalmology as a specialty arose at the intersection of two ancient forms of medical work: that of the oculist, and that of the anatomist. Oculists – practitioners who operated on the eye for conditions such as cataract – were often demonized as quacks or charlatans. Even the most successful of these practitioners, such as Baron de Wenzel, appointed oculist to George III in 1772, regularly found themselves embroiled in controversies, relying more upon the patronage of important clients than their reputation in the wider medical community (7). Nonetheless, it was the increasing success of leading oculists, and the technical innovation driven by their commercial competition, that encouraged patrons to promote the subject. One such patron was the Holy Roman Emperor Joseph II of Austria, who tasked the surgeon Joseph Barth (who had himself been instructed in eye surgery by de Wenzel) with training oculists for the Imperial states. It was Barth’s sometime assistant and illustrator, George Joseph Beer, who established the first private eye clinic in Austria, and published a series of monographs on eye diseases and the practice of eye surgery, culminating in the highly influential Lehre der Augenkrankheiten (2 volumes, 1813, 1817) (8). Beer’s pupils included the pioneer American surgeon George Frick, and the British surgeon, protégé of John Abernethy, William Lawrence. Indeed, the leading figures in the development of ophthalmology as a speciality in England in the early-to-mid-19th century – Lawrence, Richard Middlemore, and Thomas Wharton Jones – were all highly influenced by Beer’s writings (9).
Subjective visual sensations
The central thrust of the new clinical medicine of the early 19th century was the effort to correlate signs and symptoms elicited from patient, with pathological changes seen at post-mortem, or at least post-operatively. In many areas, however, it became quickly apparent that some patients experienced symptoms that could not be ascribed to particular pathological processes or were common to a number of such processes. In the nascent field of ophthalmology, therefore, a distinction was drawn between the objective signs of ocular disease, and the subjective symptoms of which patients complained. Many such symptoms were seen in conditions which were grouped under the broad term amaurosis (Greek for ‘darkening’), by which was meant vision loss or weakness in the absence of an obvious lesion affecting the eye (10).
One of the more common visual sensations was the presence of small dots in the vision. Beer used the term scotomata for these (the meaning of this term evolved over the 19th century towards its modern meaning of a blind spot in the visual field), noting that they initially might move in the vision, before becoming fixed. ‘This,’ he wrote in 1792, ‘is the seeing of gnats (visus muscorum, Myodesopsia).’ Sometimes, ‘the phantoms resemble a network or gauze’, an appearance termed visus reticulatus. Furthermore, the patient ‘often sees light and glances before the eyes (visus lucidus, Photopsia, Marmaryge Hippocratis). Sometimes he has aversion to light (Photophobia) … Not unfrequently, the patient sees all objects clouded, or as if covered with coal dust (visus nebulosus) …’. While these symptoms could be associated with incipient loss of vision, that was by no means inevitable; as Beer noted, ‘The visus muscorum… frequently accompanies hypochondriacal fits…’ (11). Beer’s term visus muscorum quickly disappeared from the literature, to be replaced by the term muscae volitantes (Latin for ‘flying flies’), which became standard usage throughout the 19th century.
Beer’s work came to the attention of the English-speaking medical world through abridgements and translations published by surgeons who had journeyed to Vienna to study with Beer (9). Richard Middlemore’s 1835 account of amaurosis leans heavily on these translations (not least because he did not read German), but also contains an account of amaurosis ‘from mental emotions’, in which a woman of 60, depressed and distressed from death of two of her children complained that: the sight became impaired very gradually and without pain, and that she was much plagued, first with a scotoma [in the sense that Beer used the term, i.e. of a dot or dots in the vision], and afterwards with an infinite number of muscae volitantes which twirled and twisted before her in the most odd and whimsical manner, so that she was often disposed to attempt their removal with her hand (10). In some cases, muscae volitantes exist as a distinct affliction for years, it being difficult or impossible to remove; … When very numerous, they interfere in some measure with vision, and greatly annoy the patient; they may even reach such a degree that the patient compares his vision to looking through a riddle (12). Objects appear confused, distorted, and as if seen through a mist. A candle appears surrounded by a halo, the flame is distorted and imperfectly defined, and the patient usually sees best in a strong light; for instance, he courts the mid-day sunshine, while he sees little or nothing in the imperfect light of twilight or the darkness of the evening… Spectral illusions are generally complained of; in some cases they are bright and luminous, like a shower of falling stars; at other times flashes of light, sparks, and scintillations, or metallic appearances, like globules of mercury.
Physics and physiology
Experimental physiology emerged as a central component of the medical sciences in the early 19th century, as a result of work by scientists such as Francois Magendie, Jan Purkynĕ, and Johannes Müller. Müller’s Elements of Physiology (first published in 1840–1842) (13) was the standard textbook of the subject across Europe throughout the century. The physiology of vision was one of the cardinal interests of many physiologists, combining as it did the hard science of optics with the emerging understanding of ocular and brain physiology.
Müller’s textbook presented a view of the subjective sensations of vision largely derived from the preceding work of Purkynĕ (14). Muller contrasted subjective sensations such as those caused by pressure on the retina, or the vascular figure seen with a luminous character (the effect subsequently known as the ‘Purkynĕ tree’), with sensations derived from: the images of objects existing in the interior of the eye, and throwing a shadow upon the retina. Such are the thread-like convoluted figures in which rows of globules appear to be contained … They are by some writers called muscae volitantes, and are confounded with certain symptoms which accompany the development of amaurosis; but they are quite innocent in their nature, and exist in persons whose powers of vision are most acute. I have been subject to them since childhood. Whether they be owing to particles floating in the aqueous humour, or contained in the vitreous body, is not known (13). Sometimes they are spots of various shape and size, black or lighter coloured; sometimes dark, with a luminous edge. They may be streaks or lines, straight, waved, angular, twisted, or united in various ways. Sometimes they appear as transparent bladders, or luminous chains, which are generally undulating. They may have a metallic appearance, like globules of quicksilver, or may seem transparent, like water or glass. Often there is the likeness of an insect, as a spider, worms, or that of a spider’s web, or portion of net… Frequently there is a single dark spot, moving with the eye and presenting before any object that is looked at; there may be many such, described as resembling the blacks floating in the atmosphere of London. When they are numerous, they interfere with vision, and annoy the patient greatly… (15)
In a new edition of his treatise published in 1854, Lawrence speculated as to the ‘immediate cause’ of the symptoms. Notions of ‘partial pressure on the nervous system, by distension of vessels in the retina or in the choroid, or by inequality in the surface of the latter membrane are plausible,’ he noted, ‘but merely conjectural.’ An explanation ‘derived from minute particles supposed to be floating in the aqueous humour’ seemed to Lawrence to ‘have foundation’, although he admitted to not having seen such particles, and pointed to the fact that muscae did not seem to be visible when a ‘fragment of lens or capsule is in the anterior chamber, or when opaque specks exist in the cornea’ (16). Lawrence also cited the views, published in 1844, of the prominent scientist and expert on optics, Sir David Brewster, who put their origin in the vitreous humour (18).
Brewster, like many of the scientists of his era with an interest in optics, was as happy making observations of his own visual experiences as of objects in a laboratory. His observations on his experience of migraine aura, for example, were cited by Hubert Airy in his classic description of the condition, published in 1870 (19). Brewster’s attention had been drawn to muscae volitantes ‘in consequence of finding in my own eye a good example of the phenomenon’. Finding that ‘yet no account has been given of them that has even the slightest pretension to accuracy’, Brewster described how when looking at the sky, or a luminous object through a small aperture, he could see ‘a luminous ground, covered, more or less, with transparent filaments or tubes, transparent circles, exceedingly minute, and (when they do exist) with Muscae, or black spots like flies’. Brewster included a drawing, made in October 1838, and noted that in several areas there was ‘a sort of transparent web containing a great number of minute spherical specks’ (Figure 1). Brewster’s view was the phenomena were caused by ‘shadows formed on the retina by divergent light passing by and through transparent filaments and particles placed within the eyeball’.
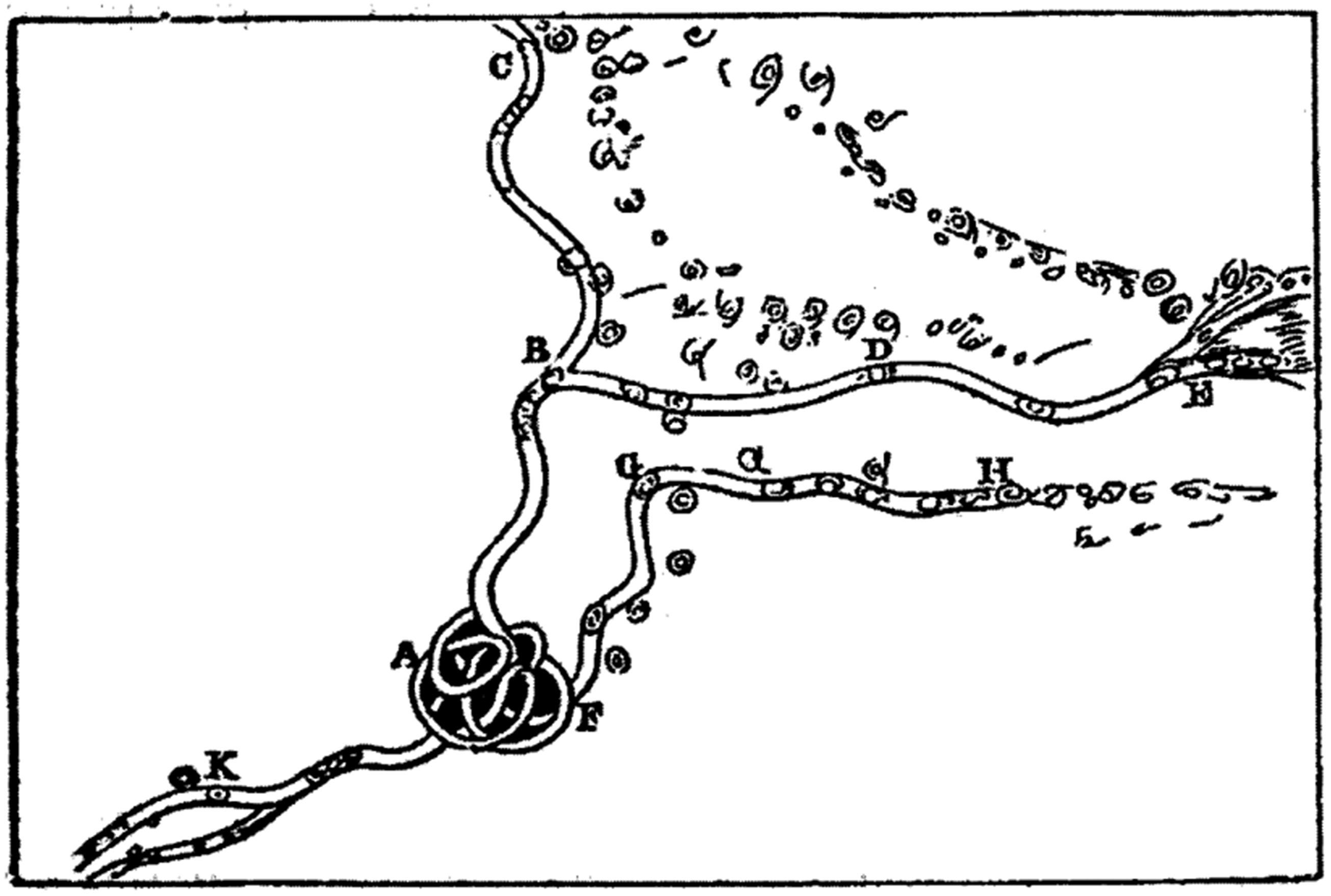
David Brewster's 1838 illustration of his own muscae volitantes.
Thomas Wharton Jones, writing the third edition of his textbook two decades after Lawrence’s original edition, was much more definitive about the causes of muscae volitantes (Figure 2). Citing Brewster’s technique for making them easier to see, he stated unequivocally that: Hitherto a very common opinion as to the nature of floating muscae has been that they are subjective sensations, depending on some intrinsic change of the state of the optic nervous apparatus…; but that they are truly objective sensations, occasioned by the presence of particles in the interior of the eye, but extrinsic and in front of the retina, throwing their defracted shadows on the retina, admits of mathematical demonstration.

Illustration of muscae volitantes from Thomas Wharton Jones The Principles and Practice of Ophthalmic Medicine and Surgery.
Wharton Jones did admit, nonetheless, that the nature of the particles had ‘not yet with certainty been demonstrated’, and suggested that they were ‘seen most distinctly, and are therefore most troublesome, where there exists an irritable state of the retina… Such a state of the retina may therefore be viewed as the general condition on which floating muscae considered as a disease, depend.’ Such a state could result from a number of causes, including a ‘Morbid sensibility of the system generally, arising from pressure of business, anxiety, and distress of mind.’
The nervous character
By the middle of the 19th century, therefore, a consensus was building that muscae volitantes were objective visual phenomena, but that those of a ‘nervous character’ were nonetheless more prone to be aware of them, and distressed by them. This observation had been made by Beer, and also by the ophthalmic surgeon James Ware, who in 1814 presented three cases of patients with particularly intrusive muscae to the Medico-chirurgical Society of London. Ware’s first case, dating back to 1786, was of a 30 year old woman, whose husband had recently died, who had woken one morning to find the whole of her vision covered by ‘a great number of small yellow motes [that] appeared to dance before every object to which she directed her eye’. In addition to these ‘yellow sparks, if the eyes were exposed to a strong light, the air appeared full of small particles resembling globules of quicksilver [mercury] in continual motion’ (20). When he saw the patient in 1790, Ware noted that ‘impressions which a strong light made on the eyes continued for some time after the light was excluded’, that ‘her arms and legs trembled, and her heart beat violently’, and that she ‘had a dull heavy pain in the back of her head; which pain sometimes extended to the forehead and sockets of the eyes… a strong beating in her temples, with a noise in her ears; and was in general remarkably irritable.’ When Ware saw her again in 1815, things had improved: ‘The moats were still occasionally perceived; but they had become so faint, that she could only see them in a strong light, and when she took pains to look for them.’ Similarly, his second patient, a 31-year-old nobleman, described ‘a considerable number of intersecting moats or beams which floated continually before both his eyes … perceived when the eyelids were closed, almost as strongly as when they were open’. Objects could appear as if ‘seen through a pane of glass sprinkled with water’. Yet 12 years later this patient ‘retained the perfect sight of both eyes’, and only saw the muscae ‘if he took pains to look for them’. Ware concluded that the ‘common exciting cause of these moats, appears to me to be too close application of the mind to objects that occasion anxiety or distress’ (20).
As the century went on, it became increasingly clear that signs or lesions could not be found to correlate with many patients’ symptoms. Such conditions were called ‘neuroses’, a term first introduced in the 18th century by the Scottish physician William Cullen. Many of the neuroses became encompassed within an influential ‘nervous turn’ in disease understanding that occurred in the 1860s and 1870s, pioneered by the American physician George Beard and the Scottish surgeon John Erichsen, driven in part by increasing numbers of patients experiencing persistent symptoms in the aftermath of railway accidents.
Beard’s seminal monograph on ‘hysteria, neurasthenia, and spinal irritation’ was published in 1874 (21). His use of the ‘old and almost forgotten term, neurasthenia’ was widely copied. ‘When the exhaustion shows itself chiefly in the brain,’ Beard noted, one might typically see ‘symptoms of insomnia, headache, vertigo, flashes before the eyes, muscae volitantes, tinnitus, etc.’ This was also Erichsen’s view (22). In his monograph on the railway and other injuries of the nervous system, published in 1866, he presented two extensive descriptions of the subjective visual phenomena that could arise after remote injury. The first case concerned what Erichsen termed concussion from ‘indirect violence’, most usually a shock of some sort: The organs of special sense usually become more or less seriously affected. Commonly, muscae volitantes and spectra, rings, stars, flashes, or sparks — white, colored, or flame-like — are complained of. The eyes often become over-sensitive to light; and this intolerance of light may amount to positive photophobia … The hearing may be variously affected. Not only does the patient commonly complain of the noises in the head and ears that have already been described, but the ears, like the eyes, may be over-sensitive or too dull … Loud and sudden noises are peculiarly distressing to these patients (22). After a time the patient usually suffers from irritability of the eyes, and cannot bear a strong light, even that of an ordinary window, in the daytime, or un-shaded gas or lamp-light. In consequence of this irritability of the eyes, the brows become involuntarily contracted, and the patient acquires a peculiar frown so as to exclude light as much as possible. This intolerance of light may amount to perfect photophobia… [it] is usually accompanied by muscae volitantes and spectra, rings, stars, spots, flashes, and sparks, or an appearance of white-colored flame … There is an undue retention of the image in many cases; and where the patient has looked at any fixed object, such as the sun or the fire, complementary spectral colors, often of the most beautiful character, of varying degrees of intensity, will develop themselves in succession (22).
Disappearance and reappearance
In 1829, the poet Alfred Tennyson wrote to his grandfather, complaining that he was troubled by muscae volitantes, for which he had undergone cupping. Anxiety about his eyesight was to accompany him constantly through what turned out to be a very long life. In 1832, he wrote to his aunt to inform her that his ‘blindness increases daily’; twelve years later he returned to the subject, complaining that the ‘animals [muscae volitantes] that you mention are very distressing and mine increase weekly: in fact I almost look forward with certainty to being blind some of these days’; ten years after that he was reporting ‘some 15 new specks in my right eye’. Tennyson lived to be 84 and never did lose his vision (23).
By the time of Tennyson’s death in the 1880s, developments in instrumentation were rendering the chambers of the eye more accessible to assessment, and innovations in histology and microbiology had demonstrated the central role of infection and inflammation in many diseases of the eye. Subjective visual phenomena largely disappeared from ophthalmological textbooks; the whole question of the nature of visual perception became sequestered within the new field of psychophysics, and eventually came to rest within experimental psychology (24). The problem of the origin of the muscae volitantes was largely regarded as solved, that is, that they were caused by the shadows of objects within, or disruptions of the vitreous humour of the eye (25). Other subjective phenomena were, as outlined in Müller’s Elements, redefined as objective phenomena that were the physiological consequences of alterations in blood flow to the retina, and so on. Patients who reported these phenomena – particularly those patients who appeared distressed by them – became labelled as hysterical, neurasthenic, and thereby unreliable. Subjective visual phenomena disappeared from the clinical literature and remained invisible for most of the 20th century. One exception was the hallucinogen persisting perception disorder, first described in 1954 as a rare consequence of exposure to hallucinogenic substances, and first included in the Diagnostic and Statistical Manual of Mental Disorders in 2000 (26). This, alongside studies of patients who appeared to have developed a persistent or permanent form of migraine visual aura, provided the context in which VSS emerged as a distinct clinical entity in the first decade of the 21st century.
The philosopher Kay Toombs, who herself suffered from multiple sclerosis, defined the essential features of illness in terms of five losses: the loss of wholeness, the loss of certainty, the loss of control, the loss of the freedom to act, and the loss of a familiar world (27,28). Many patients with VSS, like the patients described by Ware, accommodate to their symptoms, which become normal for them (29). Others cannot accommodate to the loss of their familiar – visual – world, and for them VSS is, much as it was for the patients described by Erichsen, a distressing source of disease. Such patients now, as they did 200 years ago, seek explanation, reassurance, and, where possible, treatment.
In conclusion, therefore, ophthalmological and general medical literature in the 19th century contains extensive descriptions of subjective visual phenomena, including (most distinctly in the brilliant but doomed Hocken’s 1842 treatise on amaurosis (12)) descriptions of constellations of symptoms highly reminiscent of the experiences now designated as visual snow syndrome. The 19th-century literature sits on the boundary between physiological and psychological explanatory frameworks, with a gradual consensus emerging that many of the experiences described were essentially normal, only garnering meaning and becoming distressing in the context of other psychological stressors. Such an explanatory framework remains relevant, over 200 years after the publication of Beer’s Lehre der Augenkrankheiten, and its rendering into the English language.
Article highlights
Symptoms consistent with visual snow syndrome can be found in 19th-century medical literature. Subjective visual phenomena became associated with the nervous character and thereby disappear from the clinical literature of the 20th century.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.