
Abstract
Abstract
Background
Visual snow syndrome is a phenomenon for which no effective treatment is known. It is highly comorbid with migraine, therefore we performed a retrospective chart review of patients with visual snow syndrome treated with a monoclonal antibody against calcitonin gene related peptide or its receptor.
Findings
We enrolled 15 patients with visual snow syndrome who received at least once a monoclonal antibody against calcitonin gene related peptide or its receptor. None of the patients reported relief of visual snow syndrome whereas those patients with comorbid migraine reported a very good efficacy of the antibody against the migraine headache but not against the migraine aura.
Conclusion
The data suggest that visual snow syndrome is not mediated by calcitonin gene related peptide in a relevant way and that the calcitonin gene related peptide receptor is not involved in the network underlying the visual snow syndrome.
Introduction
Visual snow is a phenomenon which was probably first reported in cocaine abusers (1) and since then has been described by Liu et al. (2) as a migraine-related symptom and found to be associated with several visual, non-visual perceptual and non-perceptual symptoms forming visual snow syndrome (3). The prevalence has been estimated to be 2.2% of the general population with a female preponderance of 1.6 to 1 (ratio) (4). There is general consensus that visual snow syndrome is very difficult to treat and controlled trials are missing (5).
As this syndrome was linked to migraine (2,3) it appeared in the appendix of the International Classification of Headache Disorder, 3rd edition (ICHD-3). Research criteria are presented in order to stimulate research on the clinical and pathophysiological nature of this syndrome (6). In particular, migraine with aura was highly comorbid (3,7). However, a significant comorbidity with common migraine without aura has also been questioned (4).
Since migraine is a frequent comorbid disorder to visual snow syndrome and since calcitonin gene related peptide (CGRP) plays a crucial role in the pathophysiology of migraine, we were interested whether the new monoclonal antibodies used in the treatment of migraine are also efficacious in the treatment of visual snow syndrome (VSS).
Methods
We performed a retrospective chart review in four tertiary headache centres in Germany and Switzerland. All patients with visual snow syndrome according to the criteria of the ICHD-3 were screened as to whether they received a monoclonal antibody against CGRP or the CGRP receptor (i.e., erenumab, galcanezumab, fremanezumab). Diagnosis was based on the ICHD-3 criteria including ophthalmological examination to exclude secondary types of visual snow syndrome. Patients with alcohol or substance abuse were not included. The indication for prescribing such an antibody was either an off-label individual treatment trial or for treating comorbid migraine according to the respective prescription guidelines with at least four migraine days per month not responding to any approved migraine preventive drug. All patients receiving at least one injection of an antibody were enrolled into the analysis. Other treatments against visual snow syndrome were stopped.
We registered demographic data of the patients, clinical data of the visual snow syndrome and, if applicable, the clinical data of a comorbid migraine disorder. Data were collected at every visit (normally every three months), the data from the last visit under CGRP antibodies was used for this analysis. Efficacy of the monoclonal CGRP antibodies against visual snow syndrome was rated according to the clinical information in free wording. Efficacy of the antibodies against migraine was rated by the number of headache days during the treatment period of four weeks or of one month, respectively. Migraine responders were patients with at least 50% reduction of headache days during the last available treatment month compared to baseline. Similarly, efficacy against migraine aura was rated by the frequency of auras during the treatment period. Since the number of patients was low, we did not perform any formal statistical analysis.
Results
In total we enrolled 15 patients who received at least once a monoclonal antibody against CGRP or its receptor. The relevant data including symptoms of visual snow syndrome are presented in Table 1. There were 12 females and 3 males, the mean age at the time of analysis was 35 +/− 13 years. The age at migraine onset and the age at visual snow syndrome onset was 15 +/− 8 and 25 +/− 11, respectively. Except for probably patient 10, all patients had later onset of visual snow syndrome. Patients 4, 6, 7, and 8 received CGRP antibodies off-label only for treating visual snow syndrome.
Demographic and clinical data of 15 patients with visual snow syndrome (VSS) receiving at least one CGRP mAB.
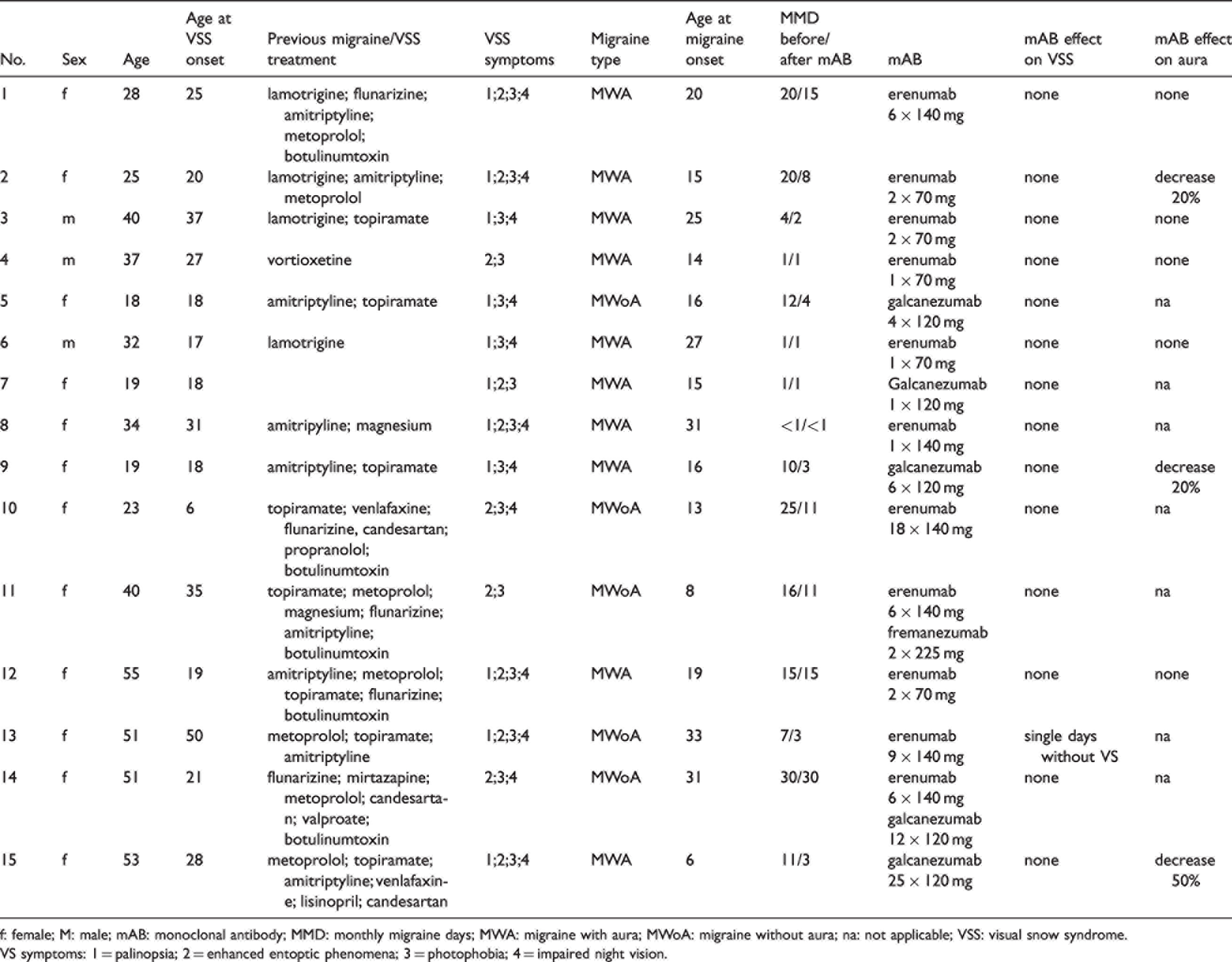
f: female; M: male; mAB: monoclonal antibody; MMD: monthly migraine days; MWA: migraine with aura; MWoA: migraine without aura; na: not applicable; VSS: visual snow syndrome.
VS symptoms: 1 = palinopsia; 2 = enhanced entoptic phenomena; 3 = photophobia; 4 = impaired night vision.
All patients except one reported no effect by the monoclonal antibody on visual snow syndrome at all (i.e., no change in frequency and no change in severity or symptomatology). One patient (patient 13) who had a particular late onset of visual snow syndrome, reported a reduction of continuous visual snow syndrome by three days per month without symptoms; however, this was not rated as a meaningful treatment by the patient. Another patient (patient 15) reported an aggravation of visual snow syndrome during migraine attacks, which was less prominent under treatment with monoclonal antibodies. The continuous visual snow syndrome, however, did not disappear. All medications listed in Table 1 did not show an effect on visual snow syndrome symptoms. All patients had comorbid migraine. Ten patients had migraine with typical aura, all of them with visual aura and one patient (patient 7) with sensory aura in addition. Visual snow syndrome started about 10 years after the first occurrence of migraine.
Regarding migraine treatment, we analysed all patients with at least four migraine days per month (n = 11). We observed a decrease of monthly migraine days from 16 +/− 8 to 10 +/− 8 over a mean observation period of seven months; the 50% responder rate was 64%. Regarding the number of migraine aura episodes, most patients reported no change while under monoclonal antibody treatment. Patient 8 mainly had visual migraine auras without headache and reported no change of the number of aura episodes per month by monoclonal antibody treatment. Two patients reported a small but not meaningful change of aura frequency, and only one patient reported a reduction of aura frequency of about 50%. In summary, in our case series the efficacy of the monoclonal antibodies was clearly shown for migraine headache, but not for migraine aura.
Eight patients had comorbid depression (patients 1, 4, 5, 9, 12–15). Two patients had comorbid anxiety disorder (patients 5 and 9), and one patient each had borderline disorder (patient 3) and bulimia nervosa (patient 15).
Discussion
Our data indicate that there is no efficacy of monoclonal antibodies in visual snow syndrome despite substantial efficacy on the number of migraine days. This suggests that blocking the molecule CGRP or its receptor does not impact the mechanism leading to the perception of visual snow syndrome. The only patient with a mild response to monoclonal antibody treatment was uncommonly old for this syndrome and might therefore have had a concurrent additional, e.g. CGRP-dependent, mechanism, although she fulfilled the ICHD-3 criteria for visual snow syndrome based on the information retrospectively available.
This suggests that CGRP does not play a major role in the pathophysiology of visual snow syndrome. Although the pathophysiology of visual snow syndrome is not fully understood, the epidemiological data point to a link with migraine. Therefore, visual snow syndrome was listed as a migraine complication in the research appendix of ICHD-3. Recently, it has been proposed that the visual snow syndrome is a network disorder of higher cortical functions (8), and that the link with migraine is more likely at the level of “being migraine patient” than having migraine attacks. Consistently, as CGRP treatment does not change the fact that someone has migraine, we conclude that CGRP is not involved in dysfunction of the network that is affected in visual snow syndrome.
For migraine pathophysiology, the role of CGRP has been shown for migraine headache. A link between CGRP and migraine aura has not been convincingly shown yet. In our case series, we could confirm the epidemiological link between visual snow syndrome and both, migraine headache and typical migraine aura. This could be confirmed in our case series with 11 out of 15 patients having migraine with typical aura, although there might be a selection bias due to the label of anti-CGRP monoclonal antibodies for migraine treatment. Our data also add to the findings that typical migraine preventive drugs are not helpful in visual snow syndrome (9).
We can confirm some features of visual snow syndrome which have been presented in large cross-sectional studies, such as the age at onset, a high comorbidity with migraine and in particular with migraine with aura (3). The 100% comorbidity with migraine seen in our case series is probably due to the fact that we enrolled our patients from tertiary headache centres and that monoclonal antibodies are only approved for migraine treatment.
Our study further supports previous data suggesting that migraine aura and visual snow syndrome might share pathophysiological mechanisms despite being distinct conditions (10). Although there was a high comorbidity, four patients with visual snow syndrome did not have migraine aura. Interestingly, although being effective for migraine headache, the monoclonal antibodies had no effect on visual snow syndrome, and almost no effect on the number of migraine aura episodes. This raises the question whether monoclonal antibodies are efficacious in migraine auras independently from their efficacy against the migraine headache or if this is specific for migraine aura in patients with VSS. Currently, monoclonal antibodies are able to reduce headache frequency in both, migraine without aura and migraine with aura (11), but evidence on the effectiveness of migraine aura alone is lacking.
A limitation of this case series is its retrospective nature and that all patients had onset of VSS later in life. Prospective studies would be necessary to confirm our findings.
Key findings
The visual snow syndrome is not influenced by monoclonal antibodies against CGRP or the CGRP receptor. Our data suggest that the frequency of migraine aura in patients with visual snow syndrome does not respond to CGRP or CGRP receptor antibody treatment. We confirm the high comorbidity rate of visual snow syndrome with migraine and in particular with migraine with aura.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.