
Abstract
Objective
Visual snow syndrome (VSS) is closely linked to migraine and involves variable visual disturbances. The present study aimed to investigate the associations between VSS and migraine, as well as VSS and anisometropia.
Methods
We studied 148 patients with VSS (54 males and 94 females, mean age 30.0 years) and 157 control participants. The mean and difference between left and right spherical equivalent refractive values, as well as the presence of migraines, were compared in patients with VSS and healthy controls. Multivariable logistic regression analyses were performed to assess the association between migraine and symptoms (palinopsia, entoptic phenomena, nyctalopia, photophobia, hyperesthesia and tinnitus) in patients with VSS.
Results
Patients with VSS exhibited a greater difference in left and right spherical equivalent refractive values and a higher prevalence of migraine compared to controls. Logistic regression analyses revealed a significant association between migraines and palinopsia. During the follow-up period, we observed spontaneous improvement in symptoms in 10 patients.
Conclusion
VSS is closely associated with migraine, and anisometropia was more frequent in VSS. The high prevalence of VSS in young individuals may reflect the age-related decline in migraine prevalence.
This is a visual representation of the abstract.
Introduction
Visual snow syndrome (VSS) is characterized by persistent visual disturbances consisting of tiny, dynamically flickering dots across the entire visual field resembling the “static” or “snow” of a poorly tuned analog television. 1 Viana et al. 2 examined the sex ratio, mean age, age at onset, retention rate of additional symptoms and prevalence of migraine in 100 patients with VSS from Italy and the UK. Their findings indicated that VSS typically manifests in individuals in their 20s, with a mean age of around 30 years, and approximately 70% of patients experiencing migraine.
Migraine is linked to VSS 3 ; however the precise relationship remains unknown. While several reports indicate a high migraine prevalence in VSS,1,2,4,5 few studies have made comparisons with healthy controls. Kondziella et al. 6 identified 38 cases of VSS among 1015 adults but found no significant difference in the prevalence of migraine or migraine aura between VSS and controls, possibly due to sample size limitations. We hypothesized that the prevalence of migraine is higher in patients with VSS than in healthy controls and that migraine contributes to VSS development.
Furthermore, several ophthalmological examinations have been conducted in patients with VSS, including assessments of visual acuity, visual field testing and optical coherence tomography (OCT),4,5 with most of these tests yielding normal results. However, the spherical refractive value, which is routinely examined in ophthalmology, has not been examined. Anisometropia is a condition in which there is a large difference in refractive values between the left and right eye. 7 If one eye is emmetropic or myopic and the other is hyperopic, the hyperopic eye may develop anisometropic amblyopia. Even if amblyopia does not develop, the differences in refractive values between the left and right eyes remain, leading to insufficient binocular vision and biased viewing in one eye. In addition, when correcting anisometropia with glasses, the refractive values of the lenses differs between the left and right eyes, resulting in a difference in the size of the images seen through the lenses (anisometropic images). Conversely, Tang et al. 8 reported that patients with VSS exhibit binocular vision dysfunction, such as stereopsis and fusion, although the cause remains unclear. Therefore, we hypothesized that a large difference exists between the left and right spherical equivalent refractive values in patients with VSS.
The present study examined the relationship between VSS and migraine, as well as between additional symptoms of VSS and migraine or aura. Moreover, the association between anisometropia and VSS was evaluated.
Methods
Study design
This was a retrospective case–control study of patients with VSS using clinical data. Data were collected consecutively and analyzed retrospectively. Patients aged ≥12 years who visited our institution between January 2019 and October 2024 were included in this study
Standard protocol approval, registration and patient consent
Informed consent was obtained from all participants prior to participation in the study. The study protocol was approved by the Institutional Ethics Committee of Mishima General Hospital. All procedures adhered to the tenets of the Declaration of Helsinki.
Study participants
In this study, we conducted a cross-sectional analysis of two populations: patient and control groups. We recruited the patient group prior to the control group. Articles about VSS were posted on the website of our medical institution, and patients exhibiting symptoms of VSS were recruited. Patients aged ≥12 years who met the diagnostic criteria for VSS were included. For patients aged ≤18 years, parental consent was required. These patients reported experiencing “visual snow” characterized by multiple dots, powder, sandstorms or noise, with symptoms that were continuous and constant. The diagnosis of VSS was confirmed using the diagnostic criteria proposed by The International Classification of Headache Disorders 3 : (A) dynamic, continuous, tiny dots across the entire visual field, persisting for more than three months; (B) additional visual symptoms of at least two of the following four types: palinopsia, enhanced entoptic phenomena, photophobia and impaired night vision (nyctalopia); (C) symptoms are not consistent with typical migraine visual aura; and (D) symptoms are not better accounted for by another disorder. Cases that met all criteria were diagnosed as VSS. The exclusion criteria included children aged <12 years, patients with ophthalmic or intracranial structural disease associated with significant visual loss and those unable to undergo adequate ophthalmic examination. We estimated the sample size needed to test the prevalence of migraine in patients and controls. The prevalence of migraine in the patient and control groups was set at 50% and 20%, respectively, with a standard deviation of 0.5. The power was set to 0.8 and the significance level was set to 0.05. As per these parameters, the sample size needed for this study was estimated to be 44 in both groups. In total, 148 patients (54 men and 94 women; mean ± SD age 30.0 ± 11.1 years) were included in this study (Table 1). All patients with VSS were followed up for at least six months and were interviewed about any changes in their symptoms since their initial visit. We rated the subjective symptoms of each patient for five categories, namely sandstorms, palinopsia, entoptic phenomenon, nyctalopia and photophobia, using a five-point scale; 0 = none; 1 = aware but not bothered; 2 = bothersome, but no daily interference; 3 = difficulty reading/writing; and 4 = unable to continue reading or writing due to symptoms. We defined improvement as one or more symptom improving by at least one grade for at least three consecutive months.
Demographic date of patients with visual snow syndrome.

SERV = spherical equivalent refractive value
p-values are the results from the Mann–Whitney U-test with Bonferroni's correction for multiple comparisons.
Subsequently, we recruited a control group with a similar mean age and sex ratio to the patient group. The inclusion criteria for controls were participants aged ≥12 years without any ophthalmologic or intracranial structural disease that significantly affected vision. For participants aged <18 years, parental consent was required. In this study, the presence of migraine may be a confounding factor between the patient and control groups. Because the prevalence of migraine is higher in women,9,10 the sex ratio of the control group was consistent with that of the patient group. In total, 157 individuals (58 men and 99 women; mean ± SD age, 32.1 ± 10.4 years) were recruited as a control group. Controls were recruited from patients who visited our ophthalmology outpatient clinic for diseases, such as conjunctivitis, chalazion and mild dry eye, that did not involve abnormalities in visual function or the visual pathway, such as the retina or optic nerve. None of the healthy participants experienced an organic brain disorder. The exclusion criteria for controls were children aged ≤12 years, experiencing VSS, and ophthalmologic diseases such as glaucoma, moderate to severe cataracts and retinal diseases that result in decreased visual acuity or visual field. However, participants with a history of migraine were included in the control group to compare migraine-related parameters with those of the patient group. We interviewed control participants with migraines about attack frequency and the presence or absence of aura.
Visual acuity measurement and spherical equivalent refractive value
The corrected visual acuity of all participants was measured using a Snellen visual acuity chart at a testing distance of 5 m. The collected data were converted to the log MAR (i.e. log of the minimum angle of resolution) scale. The spherical equivalent refractive value used for correction was calculated as the mean of both eyes and the difference between the left and right eyes in each participant.
OCT measurement
The thickness of the ganglion cell complex (GCC) in all participants was measured using spectral domain-OCT (RS-3000; NIDEK, Gamagori, Japan). GCC parameters were obtained using the macular map protocols. Global GCC thickness was measured from the internal limiting membrane to the inner plexiform layer boundary. Global GCC thickness was determined for right and left eyes.
Statistical analysis
The Shapiro–Wilk normality test indicated that the parameters (mean and difference of both spherical equivalent refractive values; and GCC thickness) for patients with VSS and control participants were normally distributed. Moreover, we assessed the differences in spherical equivalent refractive values (mean and difference between left and right eyes) between patients with VSS and control participants using the Mann–Whitney U-test with Bonferroni's correction (independent, two-tailed testing, p < 0.025). The differences in the right and left eyes of GCC thickness between patients with VSS and control participants were also analyzed using the Mann–Whitney U-test with Bonferroni's correction (independent, two-tailed testing, p < 0.025).
In all participants, we performed multivariable logistic regression analyses to determine the association between the development of VSS and various parameters (mean and difference of spherical equivalent refractive values, and the presence of migraine). Odds ratios (OR) and 95% confidence intervals (CI) were calculated for each factor. p < 0.05 was considered statistically significant for all analyses.
Within the patient group, multivariable logistic regression analyses were also conducted to assess the association between migraine and symptoms (palinopsia, entoptic phenomena, nyctalopia, photophobia, hyperesthesia, and tinnitus). Furthermore, we performed multivariable logistic regression analyses to determine the association between migraine aura and symptoms, and between spontaneous improvement of symptoms and parameters (sex, age of onset, presence of migraine, presence of aura and attack frequency). Univariable logistic regression analyses were also performed to determine the association between each improved symptom and parameters linked with spontaneous improvement.
Multiple regression analyses were conducted to investigate the association between attack frequency and additional symptoms in patients with VSS. The t-statistic and 95% CIs were estimated for each factor. p < 0.05 was considered statistically significant for all analyses. The regression model was constructed following the identification of potential confounding variables.
All analyses were conducted using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), 11 a graphical user interface for R (R Foundation, Vienna, Austria). There are no missing data in this study.
Results
We initially screened 159 patients; however, 10 were excluded for not having more than two additional visual symptoms, and one for experiencing non-continuous symptoms (Figure 1). No visual field defects were observed across all patients, and they were not diagnosed with any ophthalmological diseases by ophthalmologists. Many patients with VSS exhibit additional symptoms. Our cohort included cases of palinopsia (104 cases), entoptic phenomena (103 cases), nyctalopia (121 cases), photophobia (121 cases), hypersensitivity of hearing or sensory (hyperesthesia) (84 cases) and tinnitus (79 cases) (Table 1). A history of migraine was noted in 91 patients, and 36 of these experienced an aura as a precursory symptom. 3 The patient group included four individuals with depression and two with attention-deficit hyperactivity disorder. Although these patients had been previously administered neuro-psychiatric drugs, their medical history suggested that these medications had no effect on the development of VSS. We inquired about factors that may have triggered the onset of VSS. In total, 11 patients reported possible trigger factors, including four cases of head trauma, and one case each of glaucoma attack, cervical spine injury, cold-like symptoms, early placental abruption, altitude sickness, exposure to strong light and gas poisoning. We confirmed that the corrected visual acuity of all participants did not decrease. 3 The differences in spherical equivalent refractive values between the left and right eyes of patients with VSS and control group were 0.65 diopter and 0.45 diopter, respectively. No significant difference was observed in the mean spherical equivalent refractive values between the two groups; a larger difference in spherical equivalent refractive values was observed in patients with VSS compared with the control group (p = 0.035). Additionally, no significant difference was observed in GCC thickness between the two groups.
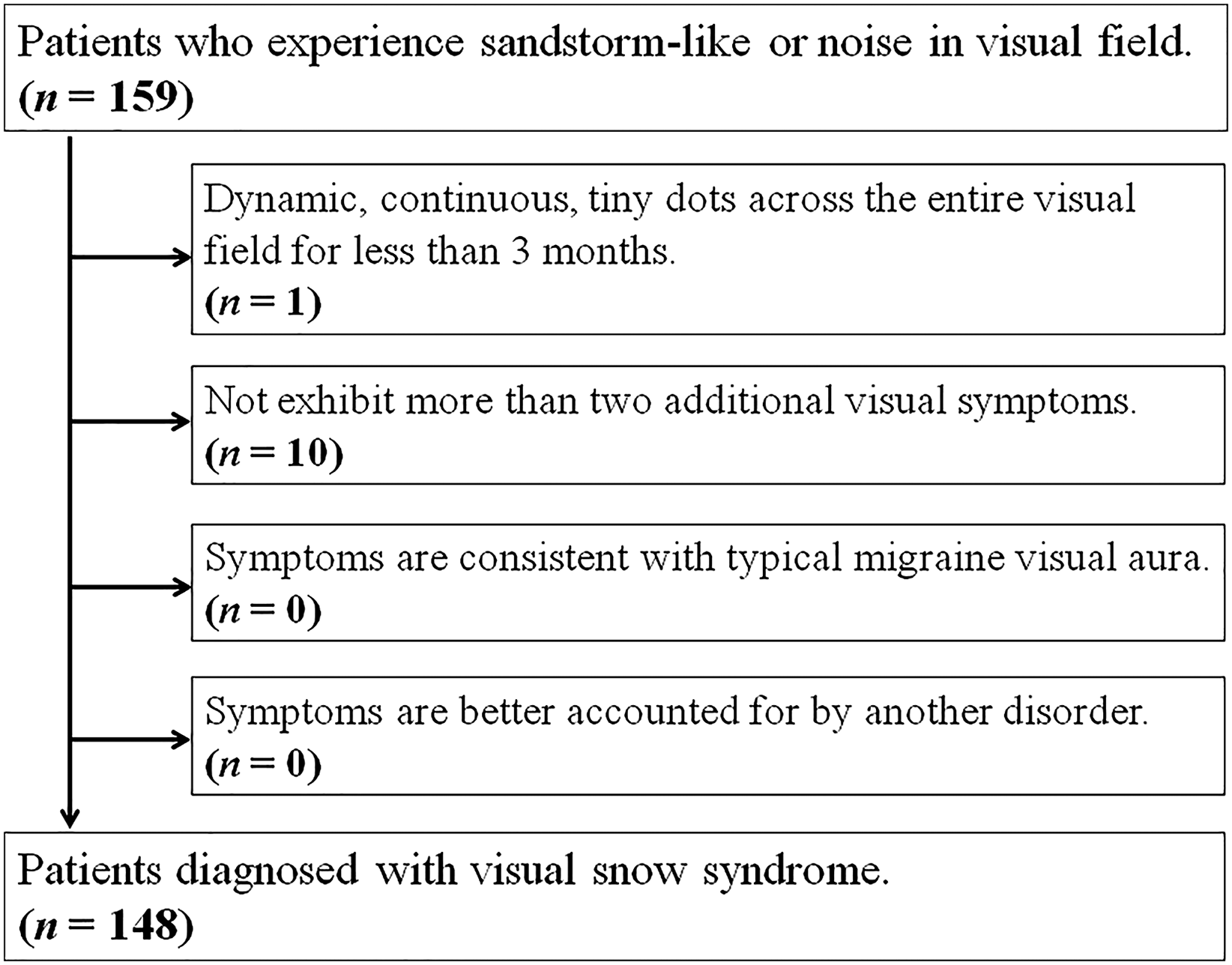
Flowchart for selecting patients to participate in the study. We diagnosed visual snow syndrome using the diagnostic criteria proposed by the International Classification of Headache Disorders. 5 We initially screened 159 cases of suspected visual snow syndrome. Among them, one case in which symptoms persisted for less than three months and 10 cases in which did not exhibit more than two additional visual symptoms were excluded.
Logistic regression analyses revealed a significant association between the development of VSS and difference in spherical equivalent refractive value (OR = 1.40; 95% CI = 1.02–1.93; p = 0.0048) and migraine (OR = 7.78; 95% CI = 3.97–15.3; p = 2.4 × 10−9) (Table 2). In patients with VSS, logistic regression analyses revealed a significant association between migraine and palinopsia (OR = 3.09; 95% CI = 1.41–6.78; p = 0.0049) (Table 3). Similarly, logistic regression analyses revealed a significant association between migraine aura and palinopsia (OR = 3.65; 95% CI = 1.26–10.6; p = 0.017) and entoptic phenomenon (OR = 3.33; 95% CI = 1.23–9.05; p = 0.018). We observed spontaneous improvement of partial or all symptoms in 10 of 148 patients with VSS during follow-up (Table 4). Logistic regression analyses revealed a significant association between spontaneous improvement of symptoms and attack frequency (OR = 1.22; 95% CI = 1.03–1.44; p = 0.022) (Table 3), as well as between spontaneous improvement of symptoms (sand-storms: OR = 1.27; 95% CI = 1.01–1.37; p = 0.039; entoptic phenomenon: OR = 1.16; 95% CI = 1.01–1.35; p = 0.040; nyctalopia: OR = 1.22; 95% CI = 1.02–1.47; p = 0.028); and photophobia: OR = 1.27; 95% CI = 1.01–1.37; p = 0.039) and attack frequency. No significant association was observed between attack frequency and additional symptoms (Table 5).
Odds ratio of each factor related to development of visual snow syndrome.

CI = confidence interval; OR = odds ratio; SERV = spherical equivalent refractive value.
Odds ratio of each factor related to migraine, presence of aura and spontaneous improvement of symptoms in patients with visual snow syndrome.

CI = confidence interval; OR = odds ratio.
Patients with visual snow syndrome who experienced spontaneous improvement of symptoms.

Attack = migraine attack frequency per month.
The intensity of symptoms at the first visit and the intensity of the symptoms after improvement were rated on a five-point scale: 0 = none; 1 = aware of symptoms but not bothered; 2 = there are symptoms that bothered, but no interference to daily life; 3 = able to read and write, but often has difficulty doing so due to symptoms; and 4 = unable to continue reading or writing due to symptoms.
Correlation between attack frequency and additional symptoms in patients with visual snow syndrome.

CI = confidence interval.
Discussion
We observed a larger difference in spherical equivalent refractive values and a higher prevalence of migraines in patients than in controls. Logistic regression analyses revealed significant associations between migraine and palinopsia. An association was also observed between aura and palinopsia and entoptic phenomenon. During the follow-up period, we observed spontaneous improvement in symptoms in 10 patients.
Characteristics of patients with VSS
In the present study, the mean age of patients with VSS at their first visit was 30.1 years, with the majority of patients falling within the age range of 20–29 years, accounting for 54 out of 148 cases. This trend is consistent with findings from other countries. In a previous study reporting 100 cases of VSS in the UK and Italy, the mean age of patients was 30 and 32 years, respectively. 2 Moreover, reports examining 28 cases in Korea 4 and 33 cases in India 5 found the mean ages of patients with VSS to be 25.4 and 29.7 years, respectively, indicating that patients with VSS tend to be younger in Asia as well.
Pathophysiology of VSS
The etiology of VSS is currently unknown. However, based on the results of recent functional neuroimaging studies the speculated main cause of the disease is alterations in brain function, including the visual cortex. Schankin et al. 12 estimated cerebral glucose metabolism using positron emission tomography in patients with VSS and observed hypermetabolism in the anterior part of the lingual gyrus. Conversely, Shibata et al. 13 reported hypoperfusion in the same area of three patients with VSS using [123I]-N-isopropyl-p-iodoamphetamine single-photon emission computed tomography. Thus, previous studies commonly report changes in the activation of the lingual gyrus; however, reports of increases and decreases in cerebral glucose metabolism or cerebral blood flow are inconsistent. Puledda et al. 14 examined the functional connectivity of each part of the brain using functional magnetic resonance imaging (fMRI) in patients with VSS, and they found altered connectivity internally within the visual network; between the thalamus/basal ganglia and lingual gyrus; as well as between the visual motion network and both the default mode and attentional networks. Further, patients with VSS presented decreased connectivity during external sensory input within the salience network, and between V5 and precuneus. The precuneus is involved in visual–spatial perception, such as stereopsis, 15 and episodic memory. Conversely, Puledda et al. 16 found reduced blood-oxygen-level-dependent (BOLD) responses to the visual stimuli concerning baseline in patients with VSS compared to that in controls in the bilateral anterior insula using fMRI. The insular cortex is a true anatomical integration hub with heavy connectivity to an extensive network of cortical and subcortical brain regions serving sensory, emotional, motivational and cognitive functions 17 ; meanwhile, the anterior insula is involved in emotional, olfactory, taste, visceral autonomic and limbic functions. 18 This result may reflect the difference in external stimuli between patients with VSS and healthy controls.
Association between VSS and migraine
Migraine affects approximately 11% of the global population, and the annual prevalence in Japan has been reported to be 8.4% (3.6% in men and 12.9% in women). 9 Notably, 39–72% of patients with VSS have a history of migraine.19,20 The visual symptoms of VSS are known to be affected by migraine attacks, and Schankin et al.1 reported that 36% of patients who experienced changes in visual symptoms had a headache attack within three days before or after the worsening of visual symptoms.
Palinopsia is the persistence of a visual image even after the removal of the stimulus, and it may be due to persistent depolarization resulting from impaired habituation in patients with migraine. The present study found a significant association between migraine and palinopsia in patients with VSS. These results are consistent with previous findings that the prevalence of palinopsia is high during non-attack episodes in VSS with migraine. 3 Palinopsia has been reported in various neurological and psychiatric disorders including stroke, brain tumors and epilepsy, as well as retinal diseases, and as a side effect of certain drugs. 21 It is also known to accompany migraine, along with aura, photophobia and hyperesthesia even in the absence of VSS. 22 In patients with VSS, some have migraine without palinopsia, whereas others have palinopsia without migraine. Although the mechanism of palinopsia development is not fully understood, Cummings et al. 21 described palinopsia as a type of visual hallucination resulting from an impaired suppression of normal visual input. Neuronal behavior in patients with epilepsy and palinopsia may differ from that in individuals with migraine and palinopsia. 22 Palinopsia in epilepsy occurs de novo, is stereotyped, and is not affected by environmental light; whereas palinopsia in migraineurs occurs due to the persistence of the image from seconds to minutes after the removal of the visual stimulus and is affected by environmental light. Epileptic palinopsia occurs as a result of synchronized neuronal excitation of the visual cortex, whereas palinopsia in migraine may be a persistence of visual memory due to impaired habituation of visual cortical neurons. Sensitization and impaired habituation may be innate behaviors of neurons and may undergo dynamic changes due to ascending inhibitory or excitatory influences. 23 Visual symptoms in VSS change depending on factors such as eyelid closure and surrounding brightness, and it has been reported that palinopsia in patients with VSS is often affected by environmental light. 1 Therefore, the mechanism of palinopsia in VSS may be more similar to that associated with migraine.
Migraine with aura is a debilitating disorder characterized by paroxysmal attacks with reversible neurological symptoms, with or without ictal pain. Although its pathophysiology remains unclear, cortical spreading depression (CSD) and, in painful attacks, trigeminovascular system activation have been implicated. 24 The aura has traditionally been closely associated with CSD, comprisinng a wave of neuronal and glial depolarization that propagates across the cortex. 25 CSD is associated not only with migraine aura, but also with the prognosis of neurovascular diseases such as traumatic brain injury, cerebral hemorrhage and ischemia. 26 Previous reports indicate that cerebral blood flow in the occipital-parietal area decreases during aura in patients with migraine.27,28 This phenomenon is considered evidence of CSD in migraine with aura. 29 Moreover, Bramanti et al. 30 observed that BOLD responses weakened in the occipital region in proportion to the frequency and severity of migraine attacks using fMRI. Similarly, decreased cerebral blood flow, including in the occipital cortex, was observed during aura. VSS is speculated to be related to functional alteration in the occipital cortex, with a previous study reporting reduced cerebral blood flow in that region. 13 VSS is also epidemiologically associated with migraine with aura, 3 suggesting a shared mechanism between VSS and aura pathogenesis.
Entoptic phenomenon
Entoptic phenomena are visual artifacts arising from the interaction of light with the specific anatomic structure of the human eye. 31 The entoptic phenomena are one of the additional visual symptoms of VSS; however, they are also observed in healthy individuals. The dichroic macular pigment in the Henle fiber layer in the fovea enables humans to perceive entoptic phenomena when viewing polarized blue light. 32 Haidinger's brushes and Maxwell's spot are known as entoptic phenomena. Haidinger's brushes consist in the appearance of a yellowish bow tie perceived in the presence of linearly polarized white light and originate from the particular spatial distribution of dichroic carotenoid molecules forming a sort of embedded radial polarizer in the foveal region. 33 Maxwell's spot is perceived when viewing a uniformly illuminated field of unpolarized light for which the wavelength is alternated between one that is predominantly absorbed and one that is predominantly transmitted by macular pigment. 33 The mechanism of the entoptic phenomena can be explained as a phenomenon occurring within the eyeball, primarily involving the retina. However, because the cause of VSS is thought to originate in the brain, including the visual cortex, 12 the entoptic phenomena in VSS may also involve the visual cortex.
Visual function in patients with VSS
Previous studies have reported that patients with VSS do not experience decreased visual acuity.4,5 However, no studies have examined the spherical refractive value in patients with VSS. In patients with anisometropia, an imbalance in visual input exists between the left and right eyes due to aniseikonia, which may affect the patient's binocular visual function. Zhou et al. 34 reported that defects in eccentric fixation and fixation stability were observed in both the amblyopic and healthy eyes in patients with anisometropic amblyopia. Additionally, Nasr et al. 35 examined the response of the visual cortex to binocular visual stimuli in patients with anisometropic and strabismus amblyopia using fMRI. They observed that patients with anisometropia had greater responses to binocular stimuli across the V1–V4 regions than healthy participants. Moreover, they found a greater increase in the size of the V1 portion area, which responded preferentially to fellow eye stimulation in anisometropic compared to strabismic individuals. Similarly, the difference in response amplitudes to binocular stimulation was greater in regions that responded preferentially to the fellow versus amblyopic eye in anisometropic than in strabismic participants. The visual cortex of patients with anisometropia exhibits heightened sensitivity to visual stimuli than that of healthy individuals and responds differently to stimulation of the left and right eyes. This suggests that a functional alteration of visual processing exists in the visual cortex of patients with anisometropia. Many patients with VSS experience a decline in binocular vision, which impacts their daily lives. 8 Functional changes in brain regions associated with visual processing, such as the temporal lobe, limbic system and parietal lobe, have been reported in patients with VSS. 12
Symptoms of VSS may improve spontaneously
In recent years, Japan has been experiencing a declining birthrate and an aging population, with the proportion of elderly people increasing. The population of Japan by age group in 2021 was 4.5 million people aged 0–4 years, 4.97 million people aged 5–9 years, 10.87 million people aged 10–19 years, 12.62 million people aged 20–29 years, 13.67 million people aged 30–39 years, 17.75 million people aged 40–49 years, 16.98 million people aged 50–59 years, 15.24 million people aged 60–69 years, 16.45 million people aged 70–79 years and 12.06 million people aged ≥80 years, respectively (Table 6). 36 However, in the present study, although patients with VSS were widely distributed from their teens to their 60s, the majority of patients were aged 20–29 years (54 cases, 36%), with 117 cases (79%) in the teen to 30s and only eight cases (5%) in the ≥50s age group. Thus, a large discrepancy exists between the age distribution of patients with VSS in the present study and the population distribution in Japan.
Number of patients with visual snow syndrome by age group and age group population of 2021 in Japan.

There is currently no established treatment for VSS. Various medications have been tried to treat VSS, including antidepressants such as selective serotonin reuptake inhibitors and tricyclic antidepressants, as well as antiepileptic drugs such as topiramate, lamotrigine and gabapentin. 37 However, improvement rates for these drugs ranged from 14% to 21%, with no effect in the majority of patients. Moreover, symptoms worsened in approximately 25% of patients. Wong et al. 38 reported that mindfulness-based cognitive therapy improved the modulation of resting-state fMRI connectivity in patients with VSS. Han et al. 39 highlighted that chromatic tint lens reduced subjective visual snow ranging from 15% to 100%, whereas Lauschke et al. 40 observed that color filters, particularly in the yellow–blue color spectrum, subjectively reduced VSS symptoms. Treatment with these color lenses can help patients in their daily lives, but it does not permanently improve their symptoms. During the follow-up of this study, we observed spontaneous improvement of partial or all symptoms in 10 of 148 patients with VSS (Table 5). In addition, logistic regression analyses revealed associations between spontaneous improvement of the symptoms (e.g. sand-storms, entoptic phenomenon, nyctalopia and photophobia) and frequency of migraine attacks (Table 7). All 10 patients with symptom improvement had photophobia, and seven had migraine. Light, such as sunlight and LED lighting, is a trigger for migraine attacks, and 38.1% of patients with migraine experience attacks induced by light. 41 All 10 patients continued to use sunglasses or other light-blocking devices at all times to alleviate photophobia, and the seven patients with migraine experienced a reduction in attack frequency. The reduction in the number of migraine attacks by blocking light may be one of the causes of the improvement in VSS symptoms.
Univariate analysis with spontaneous improvement of symptoms (sand-storms, palinopsia, entoptic phenomenon, nyctalopia and photophobia).

CI = confidence interval; OR = odds ratio.
The prevalence of migraine increases from childhood until around the age of 30 years in both men and women, peaking at 24.4% in women and 7.4% in men, before decreasing with age.9,10 Furthermore, approximately two-thirds of women experience improvement after menopause, and the prevalence drops to <10% by the time they reach their 60s. 10 The high prevalence of migraine in patients with VSS (39–72%) suggests that the lower prevalence of migraine in older adults may contribute to the reduced prevalence of VSS in this age group. However, other factors may also explain the predominance of younger patients in the present study. Recruitment through articles on our institutions’ websites may have disproportionately attracted younger individuals familiar with the internet. In addition, symptoms habituation in older adults could be a factor, as VSS typically manifests early in life. Older individuals may be less likely to report symptoms after decades of being accustomed to them.
Limitations
Patients were recruited through our institution's website, possibly leading to a younger patient cohort that was more familiar with the internet. The distribution of patients across age groups in this study may be somewhat biased because we were unable to conduct a uniformly comprehensive survey of patients with VSS throughout Japan. We observed improvement in symptoms of VSS during the observation period in 10 patients; however, permanent improvement could not be confirmed.
Conclusions
We examined 148 patients with VSS and found that, consistent with observations in other countries, the majority of patients in Japan were young adults in their teens and 30s. We observed a larger difference between left and right spherical equivalent refractive values in patients with VSS than in controls. During the follow-up period, we observed an improvement in VSS symptoms in 10 of the 148 patients. Additionally, many patients with VSS experience migraine, and the decline in migraine prevalence with age may contribute to the lower prevalence of VSS among older individuals. Appropriate treatment for migraine may alleviate symptoms of VSS to some extent.
Clinical implications
We studied 148 patients with VSS, and most of them were in their teens to 30s. The prevalence of migraine in VSS is high, and migraine in patients is associated with palinopsia. Anisometropia may be associated with the development of VSS. Ten patients exhibited spontaneous improvement, which is potentially associated with the attack frequency of migraine. The high prevalence of VSS in young individuals may be related to the decline in migraine prevalence with age.
Footnotes
Acknowledgments
This study was conducted at the Research Team for Neuroimaging, Tokyo Metropolitan Institute for Geriatrics and Gerontology, Tokyo, Japan. We thank all the participants and the medical staff who cooperated in the study. Financial support from the Visual Snow Initiative is gratefully acknowledged.
Data availability
All data used for analysis are presented as tables and figures within this article. Additional data will be shared upon ethics approval upon request by other investigators for the purpose of replicating the results.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
Informed consent was obtained from all participants prior to participation in the study. The study protocol was approved by the Institutional Ethics Committee of Mishima General Hospital.
Funding
The authors received no financial support for the research and authorship of this article, but the authors received funding for publication from the Visual Snow Initiative.