
Abstract
Background
This multicenter cross-sectional study aimed to determine the frequency and characteristics of secondary headaches in different geographic regions, including Turkey, the Middle East, Asia, and Africa.
Methods
Patients were admitted to the study on a particular day each week for five consecutive weeks between 1 April and 16 May 2022. Before the study, all researchers underwent a constructed briefing about the use and code of the ICHD-3 criteria. The study was conducted in two stages. In the first stage, data on secondary headaches were compared between the regions. In the second stage, the sub-diagnoses of secondary headaches were analyzed only in Turkey.
Results
A total of 4144 (30.0%) of the 13,794 patients reported headaches as the main symptoms at admission. A total of 422 patients were excluded from the study. In total, 1249 (33.4%) of 3722 patients were diagnosed as having secondary headaches (Turkey [n = 1039], Middle East [n = 80], Asia [n = 51], Africa [n = 79]). The frequency of secondary headaches (Turkey 33.6%, Africa 30.1%, Middle East 35.5%, Asia 35.4%) did not differ significantly between the regions (p > 0.05). The most common subtype of secondary headaches was headache attributed to substances or their withdrawal in all the studied regions. There was a female predominance in all regions, but it was lower in Africa than in Turkey. The severity and density of headaches differed significantly between the regions, with patients from Africa reporting milder pain than patients from other regions. In Turkey, the most common sub-diagnoses of secondary headaches were medication overuse headache, idiopathic intracranial hypertension, and cervicogenic headache.
Conclusion
In the present study, one in three patients with a headache had a secondary headache. Headache attributed to substances or their withdrawal was the most common subtype of secondary headaches in all the studied regions. The female predominance of secondary headaches was lower in Africa than in Turkey. The severity and density of headaches differed significantly between regions, with patients from Africa reporting milder pain.
Keywords
Introduction
Headaches are among the most common neurologic disorders prevalent in every country, affecting both sexes and all socio-economic levels. In developing countries, studies regarding the epidemiology, etiology, and experiences of headaches are markedly rare (1). Headaches have highly variable severity, from benign to life-threatening disorders, and they are traditionally classified as primary or secondary in etiology. Whereas primary headaches form the great majority, secondary headaches are important in terms of differential diagnosis and differential treatment regimen. Secondary headaches are classified in the third edition of the International Classification of Headache Disorders (ICHD-3) into eight major classes: headaches attributed to trauma, vascular disorders, non-vascular intracranial disorders, drug substance or withdrawal, infection homeostasis, cranium-neck-eyes-ears-nose-sinuses-teeth-mouth-other facial or cervical structure, and psychiatric disorders (2). Headaches have a highly variable prevalence in the literature depending on the study setting. There are few hospital-based studies about secondary headaches conducted in different countries (3–7).
The present study aimed to investigate differences in the frequency and clinical characteristics of secondary headaches in different regions such as Turkey, the Middle East, Asia, and Africa.
Methods
The present cross-sectional multicenter study was conducted using the Head-MENAA protocol (8). Patients were admitted to the study on a particular day each week for five consecutive weeks between 1 April and 16 May 2022. Study days were selected using the “Research Randomizer Program.” All consecutive patients that were admitted due to headaches were screened for eligibility. All volunteer patients with headaches were included in the study. The researchers obtained online informed consent forms from all participants.
Age over 18 years The presence of headache as the primary reason for admission to the hospital.
Age under 18 years Patients who did not report headaches at admission to the hospital Patients who did not agree to participate in the study.
Trained neurologists evaluated all patients as per the gold standard for headache diagnoses. Before the study, all researchers underwent a constructed briefing about the use and coding of the ICHD-3 criteria (2). A structured, standardized questionnaire was administered to the volunteer participants of the study (Head-MENAA Study Questionnaire- Online Supplemental material 1). The pain intensity (headache severity) was measured using a numeric rating scale (NRS). The headache density was determined as the number of days of headache per month.
The neurologists coded secondary headache subtypes using the same questionnaire according to the ICHD-3 criteria (2). The last part was left open-ended for diagnoses in the appendix, which could be included in the main text of the classification later. Invitations were sent to 32 countries from the Middle East, Asia, and Africa for their involvement in the study. Due to various intervening factors (e.g. Ramadan, summer vacation, failure to obtain ethics committee approval within the specified time), only 70 researchers from 13 countries could participate. Turkey was evaluated separately to analyze the data more accurately because 83% of the patients participating in the study were Turkish. Ivory Coast, Chad, Senegal, Sudan, Ethiopia, and Morocco from Africa; Egypt and Iran from the Middle East; Tatarstan, Turkish Republic of Northern Cyprus, Azerbaijan, and Mongolia from Asia also joined the study. The acronym of the study was determined as Head-MENAA (Middle East, North Africa, Asia) by using the initials of the names of the regions participating in the study. Ethics committee approval was obtained by the study coordinator (H.G.) from SBU Van Training and Research Hospital Clinical Research Ethics Committee (Decision no: 2022/05-01, Date: 2 March 2022).
The study was performed in two stages. In the first part, the patients were divided according to regions (Turkey, Middle East, Africa, and Asia), and data on secondary headaches were compared between regions. In the second part, the data of sub-diagnoses in secondary headaches were analyzed in Turkey. Regions other than Turkey were not included in the second part because the numbers of subjects from the other regions (Middle East, Africa, Asia) were insufficient to evaluate sub-diagnosis frequencies.
Statistical analysis
Normality control of continuous variables was done with the Shapiro-Wilk test. Parametric tests were used for the variables that fit the normal distribution, and non-parametric tests were used for the ones that did not. Independent Sample t-test and Mann Whitney U test in comparison of two independent groups, One-Way ANOVA and Kruskal Wallis tests in comparison of more than two groups, Tukey was used as the post-hoc test. The chi-square test was applied in the analysis of categorical data. The analysis of the data was made in SPSS 20.0 program. The statistical significance level was taken as p < 0.05.
Results
A total of 4144 (30.04%) of the 13,794 patients reported headaches as the main symptom on admission to the hospital or outpatient clinic. Most patients were included in the study from public centers; the minority were from private offices (Turkey [n = 223], Iran [n = 151], Egypt [n = 11]). A total of 402 patients (357 from Turkey, two from the Middle East, five from Asia, and 38 from Africa) were excluded from the study, due to not consenting to participate. A total of 20 patients from Turkey were excluded because they were aged younger than 18 years. In total, 1249 (33.45%) of 3722 patients were diagnosed as having secondary headaches according to the ICHD-3 criteria. The patients with secondary headaches were from different sections such as an outpatient clinic of neurology (n = 1035), neurology ward (n = 18), emergency department (n = 30), consultation (n = 31), and also private offices (n = 116) (Table 1). The subjects were separated according to regions (Turkey [n = 1039 (83.18%)], Middle East [n = 80 (6.4%)], Asia [n = 51 (4.08%)], Africa [n = 79 (6.3%)]) (Table 2) (Figure 1). The subtypes of secondary headaches and secondary headaches frequency were not different between the regions (Turkey 33.6%, Africa 30.1%, Middle east 35.5%, Asia 35.4%) (p > 0.05). In all regions, there was a female predominance. In pairwise comparisons, the female frequency was lower in Africa (n = 47 [59.5%]) than in Turkey (n = 775 [74.6%]) (p = 0.024). The mean ages of patients were not different between the regions (p = 0.44): Turkey (43.2 ± 0.5 [range, 18–95] years), the Middle East (42.3 ± 1.6 [range, 18–77] years), Asia (45.0 ± 2.1 [range, 18–78] years), Africa (41.3 ± 1.7 [range, 18–85] years) (Figure 2). Most patients’ headaches were attributed to substances or their withdrawal in all regions (Turkey [n = 290 (9.38%)], Middle East [n = 27 (12.00%)], Asia [n = 14 (9.72%)], Africa [n = 26 (9.92%)]) (Table 1, Figure 3).
The reference types and secondary headaches' subtypes according to regions.

M.East: Middle East, N.Policlinic: Neurology policlinic, N.Service: Neurology service,
E.Service: Emergency service, ICHD-3: International Classification of Headache Disorders, ICHD-3; 5: Headache attributed to trauma or injury to the head and/or neck, ICHD-3; 6: Headache attributed to cranial or cervical vascular disorder, ICHD-3; 7: Headache attributed to non-vascular intracranial disorder, ICHD-3; 8: Headache attributed to a substance or its withdrawal, ICHD-3; 9: Headache attributed to infection, ICHD-3; 10: Headache attributed to disorder of homeostasis, ICHD-3; 11: Headache or facial pain attributed to disorder of the cranium, neck, eyes, ears, nose, sinuses, teeth, mouth or other facial or cervical structure, ICHD-3; 12: Headache attributed to psychiatric disorder, %: among patients with headache.
The frequencies of secondary headaches in Turkey (n:1039).
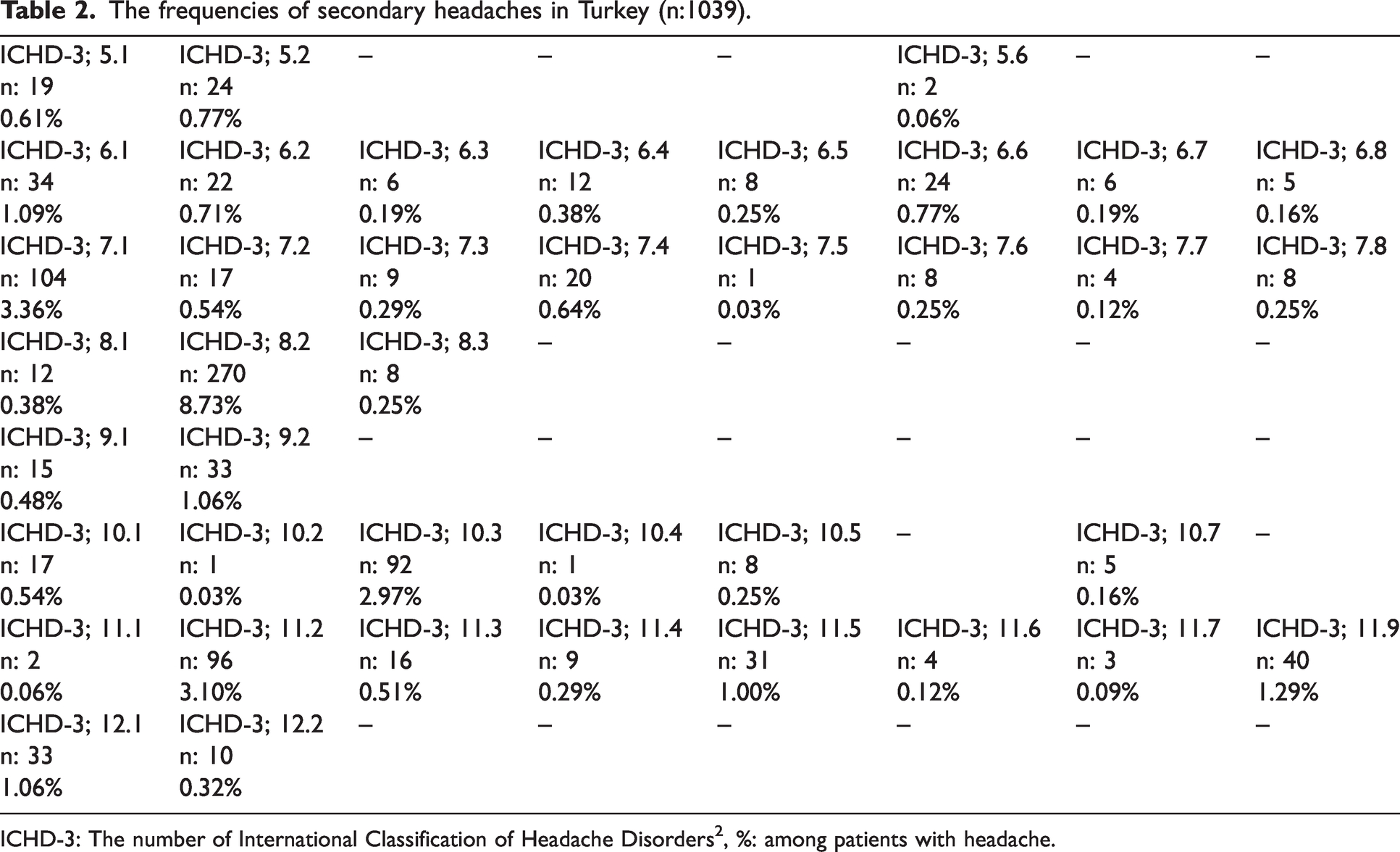
ICHD-3: The number of International Classification of Headache Disorders2, %: among patients with headache.

The summary of evaluated cases in the study.

The frequencies of secondary headaches and demographic data according to regions.

The frequencies of secondary headaches' subtypes according to regions.
Pain severity, as measured using an NRS, was different between the regions (p = 0.002). In pairwise comparisons, it was observed that the patients in Africa (6.37 ± 2.14 [range, 3–10]) presented to the hospital with milder pain than those in Turkey (6.96 ± 0.09 [range, 1–10]), the Middle East (6.87 ± 0.30 [range, 2–10]), and Asia (6.86 ± 0.27 [range, 5–9]) (p = 0.047). The density of headaches (the number of days with headache per month) was different between the regions (p < 0.001). In pairwise comparisons, it was detected that the patients in Africa (5.93 ± 1.06 [0–30]) referred to the hospital with a lower density of headaches than those in Turkey (11.68 ± 0.53 [0–30]), the Middle East (15.97 ± 1.73 [2–30]), and Asia (11.19 ± 2.15 [0–30]) (p < 0.001) (Figure 4).

The density and severity of pain in secondary headaches according to regions.
In the second part of the study, the most common three sub-diagnoses of secondary headaches were medication overuse headache (MOH) (ICHD-3; 8.2) (n = 270, [8.73%]), idiopathic intracranial hypertension (IIH) (ICHD-3; 7.1) (n = 104, [3.36%]), and cervicogenic headache (CGH) (ICHD-3; 11.2) (n = 96, [3.10%]) (Table 2, Figure 4) in Turkey (2). The mean ages were 43.1 ± 15.5 (range, 18–95) years, 43.3 ± 12.4 (range, 20–69) years, and 44.0 ± 16.7 (range, 18–77) years, respectively. Female predominance was again found in all three sub-diagnoses groups (MOH [n = 199]: 73.70%, IIH [n = 75]: 72.71%, CGH [n = 79]: 82.3%). MOH headache was observed in 10% of patients with migraine and 11.9% of patients with tension-type headache (TTH).
Discussion
In this multicenter study, we investigated secondary headaches in different regions (Turkey, the Middle East, Asia, and Africa). Among 3722 subjects with headaches, 1249 (33.4%) were diagnosed as having secondary headaches according to expert physicians using the ICHD-3 criteria (2). The frequency of secondary headaches did not significantly vary across the regions (Turkey 33.6%, Africa 30.1%, Middle East 35.5%, Asia 35.4%). Our rates were higher than most reported data, possibly due to the hospital-based approach and evaluation by headache experts from Neurology outpatient clinics (5,9–13). Previous studies reported different frequencies: Iran (20.1%) (5), China (27%) (9), Germany (31%) (10), Spain (29.4%) (11), the United States of America (21%) (12), and Japan (18.4%) (13). On the other hand, our rate was lower than in a study in Africa (47.1%) (4). These rates highlight the significance of accurate diagnosis for secondary headaches and suggest potential regional influences. Methodologic differences in questionnaire use and headache diagnosis by experts may account for these differences. The current study was performed with a standardized questionnaire and headache expert examinations to ensure a reliable estimation of secondary headache frequency.
In this study, the mean ages of patients did not differ significantly among the four examined regions: the approximate age was 43 years in Turkey, 41 years in Africa, 42 years in the Middle East, and 45 years in Asia. The mean age of patients with secondary headaches varies depending on the underlying cause. For example, giant cell arteritis-related headaches and intracranial neoplasm-related headaches typically affect adults aged over 50 years (14,15). Meningitis-associated headaches can occur at any age but are more common in children and young adults (16). Idiopathic intracranial hypertension (IIH)-related headaches have a mean age of 29.4 years (17). The relationship between age and different types of secondary headaches requires further investigation.
The severity and density of headaches play a crucial role in diagnosing and treating secondary headache disorders (17). A recent systematic review emphasized their significance and suggested thorough evaluations for patients with severe or persistent headaches (18). Our study observed significant differences in pain severity and density among regions, with patients from Africa reporting milder pain. However, the literature indicates that African-American women may experience more severe and undertreated chronic pain conditions (19). Our study, by contrast, found African individuals to be more sensitive to pain. Cultural, social, and physiologic factors may contribute to these differences, warranting further investigation (20,21). Considering headache severity and density is essential for managing secondary headaches, and understanding regional variations requires comprehensive research.
In the present study, the most common causes of secondary headaches in Turkey were medication overuse headache (MOH), IIH, and cervicogenic headache (CGH). Similarly, MOH and CGH were the two most frequent causes of secondary headaches in the literature (10–12). In this study, MOH ranked first among secondary headache subtypes as mentioned previously (22). The incidence of MOH varies globally, with studies reporting frequencies ranging from 0.5% to 7.2% (23). For instance, Denmark reported a prevalence of 1.8%, while Mongolia, Russia, and Iran recorded higher rates of up to 7.2% (24,25). The mean age at MOH diagnosis in our study was 43.12 ± 15.49 years; the peak frequency is typically observed between 50 and 60 years (25). In Turkey, MOH frequency was higher and the mean age was lower compared with the other countries, possibly due to limited awareness and easy access to medication (22). The female/male ratio of MOH in Turkey, 3 to 1, aligns with literature findings (female/male: 4/1) (25). Our study found a frequency of approximately 3.1% for CGH among patients with headache with a notable female predominance (female-to-male ratio of 4.64), different from the reported ratio (26,27). Further research is needed to explore the underlying factors contributing to this significant sex disparity in CGH.
Our study in Turkey examined the frequency of IIH among patients with headache. The results showed a frequency of 3.36% in admitted patients, with a female-to-male ratio of 2.58, consistent with literature reports (28,29). A study in North India found a higher frequency of IIH in patients with chronic daily headache compared with Western populations (30). The mean age at diagnosis was 43.32 ± 12.38 years, whereas previous population-based studies reported an age range of 23 to 36 years for IIH (31–33). The mean age at diagnosis in Turkey was higher than reported, although some patients were admitted for follow-up visits.
In Sub-Saharan Africa (SSA), secondary headache disorders caused by various infections are prevalent and contribute to a significant burden of disability and economic impact on patients and society (34). Sleep disorders, which are also prevalent in SSA, have been linked to infectious diseases such as human African trypanosomiasis and HIV (35). Similarly, a study conducted in Egypt identified meningitis as the second most common cause of secondary headache, following post-traumatic headache (35). In the Middle East and North Africa (MENA) region, other infectious diseases such as tuberculosis, HIV/AIDS, and brucellosis have also been associated with secondary headaches (34). In our current study, we investigated the frequency of headaches attributed to infections according to the ICHD-3 criteria (2). We found that the frequency of headaches attributed to infections varied across different regions, with Turkey at 1.55%, the Middle East at 1.33%, Asia at 2.08%, and Africa at 0.76%. In practice, most patients with acute headaches attributed to a systemic infection do not come directly to the Neurology department. In this study, we only included the subjects from the Neurology departments. This may explain the low frequency of headaches attributed to infections in the present study. If we collected the subjects from other departments, such as emergency and infectious diseases we would probably find a higher frequency of headaches attributed to infections. These findings highlight the need for a deeper understanding of the complex interplay between neuroinfections, the immune system, neuroinflammation, and neurologic disorders to develop improved diagnostic tools and therapeutic approaches for the management of secondary headaches in these regions.
Non-communicable diseases such as hypertension, diabetes, and ischemic stroke are also major contributors to secondary headache disorders in the MENA region (36). Another review emphasized that mostly in regard to headache as a secondary symptom of elevated blood pressure (37). Moreover, a recent study from Iran showed that patients with ischemic stroke were more likely to experience headaches than those without stroke (38). In the present study, headache attributed to cranial or cervical vascular disorder (ICHD-3; 6.1) (2) was observed in Turkey (3.78%), the Middle East (4.00%), Asia (4.86%), and Africa (3.43%). Also, headache attributed to ischemia (ICHD-3; 6.1) (2) was observed in 1.09% of patients in Turkey.
Cranial and cervical artery diseases, such as giant cell arteritis and carotid artery dissection, have been reported as potential causes of secondary headache in the MENA region (36). A study from Turkey reported that giant cell arteritis was the second most common cause of secondary headaches in the population (39). In the current study, headache attributed to arteritis (ICHD-3; 6.4) (2) was detected at a rate of 0.38% in Turkey.
Limitations and future directions
The present study has several methodologic limitations.
First, because this is a hospital-based survey, the data cannot be used to estimate the prevalence of secondary headaches in the general population. Future studies may be performed door-to-door in the general population.
Second, a heterogeneous number of patients was included in the study from different regions. The number of subjects from Africa, the Middle East, and Asia may be considered insufficient for a prevalence study. Subsequent studies should have a homogeneous number of patients from Turkey, Africa, the Middle East, and Asia.
Also, future directions for this research could involve conducting longitudinal studies to explore the long-term trends and changes in the frequency, characteristics, and sub-diagnoses of secondary headaches in different geographic regions, as well as investigating potential cultural and environmental factors that may contribute to the observed differences.
Conclusion
Secondary headache disorders are a major health issue, one in three patients with headaches in hospitals has a secondary headache in the MENA region. Headache attributed to substances or their withdrawal is the most frequent secondary headaches in the sample of present study. The secondary headache frequency was not different between Turkey, Africa, the Middle East, and Asia. The female predominance of secondary headache in Africa was lower than in Turkey, for as yet unknown reasons. African patients presented to the hospital with milder pain (severity/density) than in other regions. Healthcare providers in the MENA region should be aware of different underlying conditions associated with secondary headaches and use appropriate diagnostic tools to ensure timely and accurate diagnosis and treatment of patients.
Article highlights
In the present hospital-based study, one in three patients with a headache had a secondary headache. Headache attributed to substances or their withdrawal is the most frequent secondary headaches in the sample of present study. African patients presented to the hospital with milder pain (density/severity) than in other regions.
Authors’ information
Authors and affiliations (by institutional alphabetical order) of the Head-MENAA study group
Binyam Alemayehu, Dereje Melka, Michael Tesfaye Ketema, Yared Mamushet Yifru: Department of Neurology, Addis Ababa University, College of Health Sciences, Tikur Anbessa Hospital, Addis Ababa, Ethiopia
Faculty of Medicine, Al Neelain University, The National Centre for Neurological Science, Khartoum, Sudan: Etedal Ahmed Abu Elbasher Ibrahim
Neurology Clinic, Ankara Bilkent City Hospital, Ankara, Turkey: Merve Onerli Yener
Department of Neurology, Balıkesir University Faculty of Medicine, Balıkesir, Turkey: Nermin Tepe
Department of Neurology, Bulent Ecevit University Faculty of Medicine, Zonguldak, Turkey: Esra Aciman Demirel
Neurology Clinic, Bursa Dr. Ayten Bozkaya Spastic Children’s Hospital and Rehabilitation Center, Bursa, Turkey: Sibel Cekic
Department of Neurology, Celal Bayar University Faculty of Medicine, Manisa, Turkey: Aysın Kisabay Ak, Fatih Celik
Neurology Clinic, Center Universal Hospital de Cocody, Abidjan, Ivory Coast: Agbo Panzo Segla Achi Cedric
Neurology Clinic, City Clinical Hospital, Kazan, Russia: Valeeva Kadria Gumanovna
Department of Biostatistics and Medical Informatics, Cukurova University, Adana, Turkey: İlker Ünal
Neurology Clinic, Fann Hospital of Dakar, Dakar, Sénégal: Seck Lala
Department of Neurology, Faculty of Medicine, Gazi University, NÖROM, Ankara, Turkey: Doga Vuralli
Department of Neurology, Giresun University Faculty of Medicine, Giresun, Turkey: Demet Seker, Husniye Aylin Hakyemez, Vedat Ataman Serim
Department of Neurology, Pain and Headache Unit, Hacettepe University, Faculty of Medicine, Ankara, Turkey: Melike Cakan
Department of Neurology, Harran University Faculty of Medicine, Sanlıurfa, Turkey: Dilek Agircan, Tulin Gesoglu Demir
Neurology Clinic, Haydarpasa Numune Training and Research Hospital, Istanbul, Turkey: Buse Rahime Hasirci Bayir
Department of Neurology, School of Medicine, Istanbul Medipol University, Istanbul, Turkey: Abdulkadir Ermis, Burcu Polat, Elmir Khanmammadov
Neurology Clinic, Istanbul Training and Research Hospital, Istanbul, Turkey: Tugba Okluoglu
Department of Neurology, Istanbul Faculty of Medicine, Istanbul University, Istanbul, Turkey: Elif Kocasoy Orhan, Esme Ekizoglu, Ozgu Kizek
Neurology Department Clinical Neurophysiology Unit, Medical Faculty, Karadeniz Technical University (KTU), Trabzon, Turkey: Oznur Kirbasoglu, Sibel K. Velioglu
Neurology Clinic, Kartal Dr. Lutfi Kirdar City Hospital, Istanbul, Turkey: Samiye Ulutas, Tulin Akturk
Neurology Clinic, Kastamonu Training and Research Hospital, Kastamonu, Turkey: Birsel KUL
Neurology Clinic, Kutahya Health Sciences University, Kutahya, Turkey: Sibel Canbaz Kabay
Department of Neurology, Maltepe University Faculty of Medicine, Istanbul, Turkey: Miruna Florentina Ates, Nilgun Cinar, Sude Kendirli Aslan
Neurology Clinic, Marmara University Pendik Training and Research Hospital, Istanbul, Turkey: Berin Gulatar Turkoglu
Department of Neurology, Mersin University Faculty of Medicine, Mersin, Turkey: Ozum Yolcu
Department of Neurology, National Reference Teaching Hospital of N’Djamena, N’Djamena, Chad: Foksouna Sakadi
Neurology Clinic, Nevsehir State Hospital, Nevsehir, Turkey: Esra Demir UNAL
Neurological Clinic “New Technologies LTD,” Baku, Azerbaijan: Ilaha Azizova
Shams University and Neuromed Clinics, Cairo, Egypt: Ramez Reda Moustafa, Ahmed Gomaa Nowar
Center of Psychiatry, Neurology and Neurosurgery, Tanta University Hospital, Tanta, Egypt: Marwa Yassien Badr
Department of Neurology, Tehran University of Medical Sciences, Tehran, Iran: Elham Jafari, Somayeh Nasergivehchi
Neurology Clinic, Umraniye Training and Research Hospital, Istanbul, Turkey: Gizem Gursoy
Neurology Clinic, University of Health Sciences, Konya Beyhekim Training and Research Hospital, Konya, Turkey: Ahmet Kucuk
Neurology Clinic, University of Health Sciences, Sisli Hamidiye Etfal Training and Research Hospital, Istanbul, Turkey: Tuba Cerrahoglu Sirin
Neurology Clinic, University of Health Sciences, Antalya Training and Research Hospital, Antalya, Turkey: Ruhsen Ocal
Department of Neurology, University of Health Sciences, Erenkoy Mental and Nervous Diseases Training and Research Hospital, Istanbul, Turkey: Fusun Mayda Domac
Neurology Clinic, University of Health Sciences, Haseki Training and Research Hospital, Istanbul, Turkey: Ayla Culha Oktar
Neurology Clinic, University of Health Sciences, Adana City Training and Research Hospital, Adana, Turkey: Zeynep Selcan Sanli
Neurology Clinic, University of Health Sciences, Van Training and Research Hospital, Van, Turkey: Gokhan Gorken, Muhammet Okay Orun, Mustafa Kiraz, Sibel Ozkan
Department of Neurology, Faculty of Medicine, University of Kyrenia, Kyrenia, Cyprus: Pinar Gelener
Supplemental Material
sj-pdf-1-cep-10.1177_03331024231194024 - Supplemental material for Secondary headache disorders in Turkey, the Middle East, Asia, and Africa: A cross-sectional, multicenter study
Supplemental material, sj-pdf-1-cep-10.1177_03331024231194024 for Secondary headache disorders in Turkey, the Middle East, Asia, and Africa: A cross-sectional, multicenter study by Ahmet Evlice, Hamit Genç, Derya Uluduz, Betul Baykan, Hayrunnisa Bolay, Isin Unal-Cevik, Najib Kissani, Otgonbayar Luvsannorov, Mansoureh Togha, Aynur Ozge and on behalf of Head‐MENAA study group in Cephalalgia
Footnotes
Authors’ contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding information
The authors received no financial support for the research, authorship, and/or publication of this article. However, they would like to express their heartfelt gratitude to the Global Migraine and Pain Society for their support in establishing a network and providing unrestricted support.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.