
Abstract
Objectives: Allodynia is frequently associated with migraine and other primary headaches. Our aim was to investigate the presence of allodynia and related features in idiopathic intracranial hypertension (IIH), which is a disabling secondary headache disorder.
Methods: We included 46 IIH patients and analyzed their clinical and laboratory findings retrospectively. Allodynia was assessed using the validated 12-item allodynia symptom checklist (ASC-12), in addition to examining pressure (with von Frey filaments) and brush allodynia.
Results: Allodynia was detected in 23 (50%) of IIH patients with ASC-12 and/or instrumental testing. The most commonly reported location was unilateral V1 distribution. The allodynic symptom profile was similar but milder when compared to 143 migraineurs with ASC-12. Only the aggravation of headache with physical activity emerged as a significant variable associated with allodynia in IIH. Among allodynic patients, only eight had previous migraine diagnosis. After onset of IIH, 20 patients reported migraine-like headache, while only three reported non-migrainous headache. In contrast, 13 of 23 non-allodynic IIH patients had non-migrainous headache features (p = 0.0045).
Conclusion: Half of the IIH patients reported allodynia, and these allodynic patients had mostly migraine-like headache profiles. Our study suggested that IIH may trigger some common mechanisms with migraine in pain pathways causing allodynia.
Keywords
Introduction
Cutaneous allodynia (CA) is the perception of pain or discomfort induced by non-noxious stimuli to normal skin (1). The underlying mechanism of allodynia is proposed as increased sensitization of the central nervous system. Sensitization of second-order neurons at the level of the trigeminal nucleus caudalis can result in CA (2,3). This phenomenon is reported in primary headaches such as migraine (2,3), tension-type headache (TTH) (4), cluster headache (5), short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (6) and also with neuropathic pain conditions such as postherpetic neuralgia, chronic regional pain syndrome and cases with post-stroke or post-surgical pain (7).
CA has been found to be associated with female sex, frequent headache, increased body mass index (BMI), disability and depression among migraine sufferers (8). Its frequent association with chronic migraine, which is classified as a complication of migraine, is also notable (9). However, the risk of developing central sensitization and exact factors triggering and sustaining this phenomenon still remain unknown (7).
The presence of CA can be investigated by instrumental testing: Dynamic mechanical (brush) allodynia (BA) is assessed by brushing the skin or applying a gauze pad (10); static mechanical (pressure) allodynia (PA) by using von Frey filaments (11) and thermal allodynia through quantitative sensory testing. Also, a practical and useful questionnaire called The 12-Item Allodynia Symptom Checklist (ASC-12) has recently been developed to detect allodynia interictally (12).
Idiopathic intracranial hypertension (IIH) is a syndrome of increased intracranial pressure of unknown cause characterized by frequent headaches, in addition to visual symptoms and signs (13). IIH has invariably been associated with female gender and obesity, which are also associated with CA in primary headaches (14). It has also been reported that the headache suffered in IIH was not specific and may have migrainous features (15). Some IIH patients with a previous history of episodic headache later have developed chronic daily headaches or a new headache with different features (16). The presence of allodynia in IIH as a secondary headache disorder has not been investigated yet.
We aimed to investigate the presence, severity and modalities of allodynia as well as the headache features in patients diagnosed with IIH and their possible associations.
Methods
Clinical and laboratory investigations of the IIH patients
We investigated all patients’ files fulfilling the modified diagnostic criteria for IIH (17) who were admitted to our headache outpatient clinics. Lumbar punctures, magnetic resonance imaging (MRI) studies, complete blood counts and blood biochemistry analyses were performed on all of them. All patients were examined by neuro-ophthalmologists at time of diagnosis and regularly during the follow-up. Patients with inadequate documentation, those lost to follow-up, or those having a secondary cause such as cerebral venous thrombosis, Behçet’s disease or medication-induced intracranial hypertension were excluded. We did not include IIH patients without papilledema in our study.
We included 46 available patients with IIH followed between 2002 and 2011 to determine the frequency and diagnosis of headaches occurring before and after diagnosis and treatment of IIH, after their informed consent. The character of headache leading to diagnosis of IIH and headaches experienced before were determined by reviewing patients’ files and also by interviewing them in case of any missing data. We classified headaches reported prior to the development of IIH according to International Headache Society (IHS)-2004 criteria (18) and the headache related to IIH was grouped as migraine-like or chronic migraine-like or non-migrainous with or without chronic pattern. The patients fulfilled all criteria for these diagnoses except the exclusion of a headache etiology. The local ethics committee approved our study.
We also investigated current age, age at onset, follow-up duration, sex, medical history, prognosis of headache and of visual acuity. All patients were treated medically or surgically for IIH according to their clinical needs. Patients with IIH who experienced headaches after the standard treatment with acetazolamide and resolution of papilledema were also treated with conventional agents for headache prophylaxis such as low-dose amitriptyline and/or topiramate. We always avoided analgesics to prevent medication overuse headache. None of the patients had peripheral neuropathy or other neurological or dermatological diseases that may affect sensory functions. The possible paresthetic side effect of topiramate was carefully considered, and the temporal relationship was taken into account.
Investigation for allodynia
We translated and validated the ASC-12 questionnaire and then administered it to all IIH patients, preferably during their office visits or by telephone calls (20 patients). ASC-12 questions were directed retrospectively to detect the presence of allodynia during the most severe type of headache. The patients responded to the ASC-12 questions during interictal periods, and this questionnaire typically covers the allodynia in daily life in general. On the other hand, the time of the investigation for allodynia by instrumental testing (during a period with or without headache) was recorded and is shown in Figure 4.
The daily activities explored in ASC-12 were combing hair; pulling hair back; shaving face; wearing eyeglasses, contact lenses, earrings, a necklace or tight clothing; taking a shower; resting the face or head on a pillow and exposure to heat or to cold. Certain items were sex-specific; some were not applicable to every patient. ASC-12 items were scored as 0 (never, rarely, does not apply to me), 1 (less than half the time) or 2 (half the time or more). Based on these scores, allodynia could be defined as absent (scores 0–2), mild (3–5), moderate (6–8) or severe (9–24). We also included 143 consecutive patients diagnosed with migraine with or without aura as the control group for ASC-12.
Twenty-six IIH patients were further tested during their routine visits both for BA and PA. BA was investigated with two tools in all patients: by folding a 4 × 4-inch gauze pad 10 times at a frequency of two times per second (2/s) (19) and also by using a brush with soft nylon hairs. To detect PA, we applied von Frey hairs of three different weights (0.32 g, 8.30 g and 24 g) three times to each area, holding down for 1 s and releasing. The skin areas tested were the V1-3 and C2-3 dermatomes bilaterally. There were no reports of allodynia outside the head of our IIH patients and therefore we did not systematically test extracephalic allodynia. All patients citing allodynia according to ASC-12 or reporting allodynia during instrumental testing were accepted to be allodynic for further analyses.
At the time of instrumental testing, patients were asked to rate their current headache intensity on a scale of 0 to 10 to detect whether they had a mild (scores 1–3), moderate (4–6) or severe (7–10) headache.
Statistical analysis
Descriptive statistics were applied, and the IIH patients with and without allodynia were compared with Chi-square tests, Fisher’s exact test and independent samples t test, where appropriate. SPSS 15 software was used and the significance level was set at p < 0.05.
Results
Clinical and laboratory findings of IIH patients
We included 46 patients (four male patients) with a mean current age of 40.6 ± 10.6 years and with a mean age at onset of 35.3 ± 11.3 years. The duration of IIH symptoms was 360 days (range five to 3960) before the diagnosis. The follow-up period was 12.73 months (range one to 112 months). Associated conditions were hypothyroidism in three patients, diabetes mellitus type II in two patients (without evidence of polyneuropathy) and hypertension in two patients, whereas major depression, panic disorder, glaucoma and pemphigus vulgaris were each seen in one patient. Average BMI was 30.77 kg/m2 (range 22.49–42.45). Cerebrospinal fluid (CSF) analysis was normal except for increased CSF opening pressure (median: 350 mmH2O; range 200–840). Cranial contrast-enhanced MRIs and biochemistry analyses were normal in all of them. Magnetic resonance venography (MRV) was performed in 35 of the patients, showing normal results.
The most severe presenting symptom was headache in 44 patients; two others complained mostly of cloudy vision besides headache. Among all, three patients had minimal vision loss (0.9/0.9; 0.9/0.8; 1.0/0.8: Right (R)/Left (L) whereas another one had vision loss of 0.3/0.7 (R/L); these four patients underwent optic nerve fenestration.
Eleven patients were diagnosed with migraine (23.9% of the main IIH group), seven with TTH (15.2%) according to IHS-2004 criteria, before the onset of IIH symptoms. There was one patient diagnosed with chronic migraine before the IIH onset, who also had papilledema when admitted to our clinic.
Characteristics of patients having idiopathic intracranial hypertension (IIH) with and without allodynia.

CSF: cerebrospinal fluid; *diagnosed according to the 2004 International Classification of Headache Disorders (ICHD) criteria for primary headaches except for the exclusion of specific etiology of IIH. **Fisher’s exact test two-sided using the approximation of Woolf; odds ratio (OR) 8.667 with 95% confidence interval: 1.998 to 37.596; ***the associated headache features could clearly be retrieved from the files in only 44 patients and headache frequency could be ascertained in only 42 patients; the percentage in parentheses represents the ratio of these patients; †one patient had previous chronic migraine.
Headache prognosis was excellent in only 10 IIH patients (21.7%) who did not complain of headache in their follow-up period, whereas the remaining 36 patients (78.3%) had either relapses (12 patients; 26.1%) of IIH or continuing headaches during the course.
Results of ASC-12
All IIH patients and 143 migraineurs as the control group responded to ASC-12 questions. Among our IIH group, allodynia was cited by 18 patients (39.1%), being moderate in nine and mild in nine patients. None of the IIH patients reported severe allodynia. The percentages and severity of allodynia are shown in Figure 1 in comparison to the control group of migraineurs. Among the IIH patients with allodynia, only four had a previous migraine and one had chronic migraine. Headache related to IIH was migraine-like in 17 out of these 18 cases; moreover, secondary headache had a chronic course in 10 of these 17 patients. On the other hand, nine of 10 patients with non-migrainous headache related to IIH did not report allodynic symptoms.
The distribution of severity of allodynia in 46 idiopathic intracranial hypertension (IIH) patients, according to ASC-12 questions, in comparison to the control group of 143 migraineurs.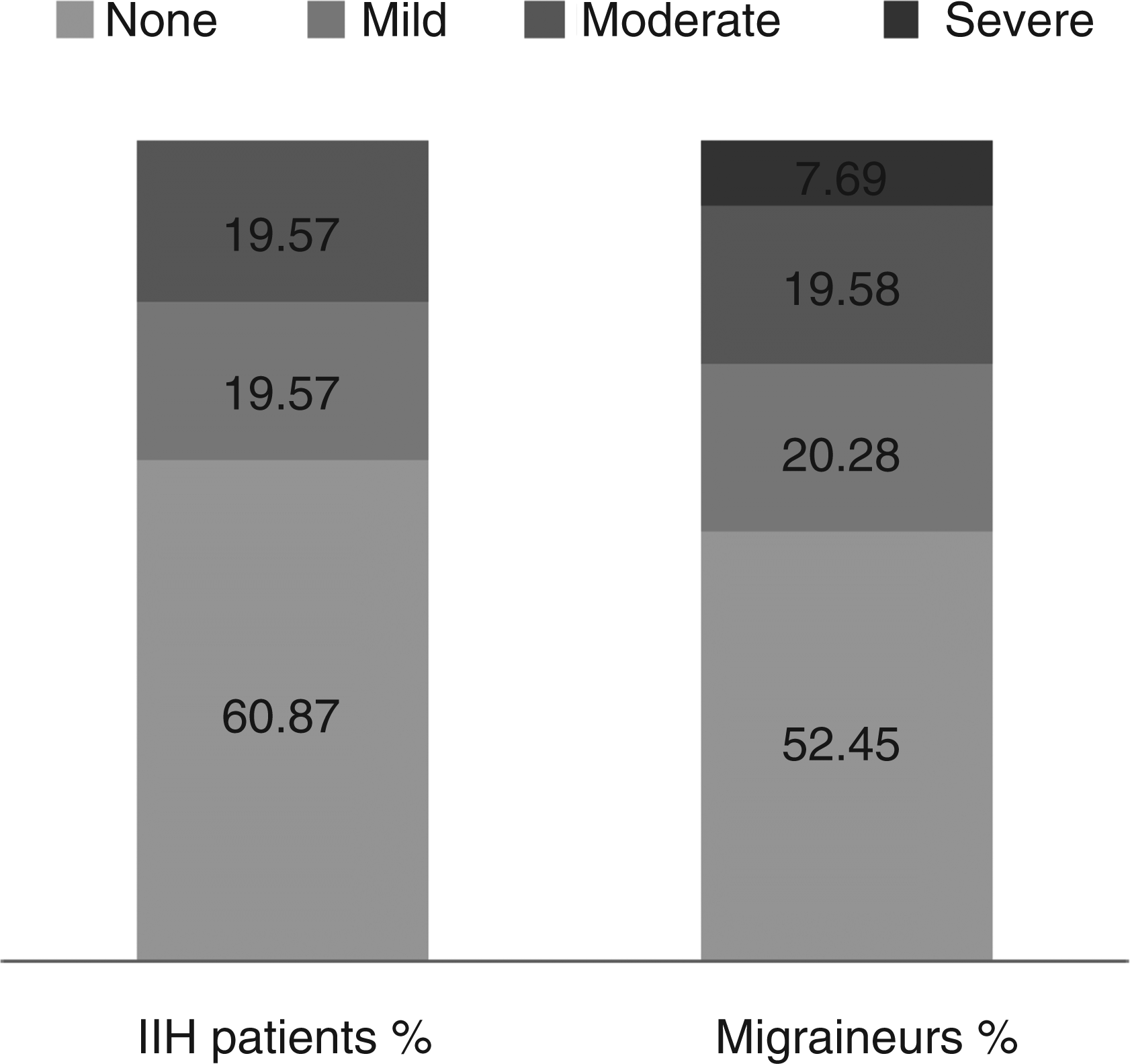
In the control group with migraine, the rate for allodynia was found to be 68/143 (47.6%), with 11 migraineurs reporting severe allodynia. The answers to the ASC-12 questions are shown in Figure 2 for both groups. The overall allodynic profile of IIH patients was similar but somewhat milder when compared to migraineurs, as shown in Figure 2.
Daily life activities bringing out allodynia as asked by the questions of ASC-12 in idiopathic intracranial hypertension (IIH) patients in comparison to the control group of migraineurs.
Results of instrumental testing for allodynia
Cited locations for allodynia in IIH patients.

IIH: idiopathic intracranial hypertension.
By instrumental testing, we detected both BA and PA in nine (34.6%) patients, only PA in four patients and only BA in just one patient (Figure 3). Nine of them had also reported allodynia during their most severe type of headache according to ASC-12, retrospectively. Figure 4 shows the relationships of the instruments used to test allodynia with the actual severity of headache during testing of these 26 patients.
Distribution and overlap of pressure allodynia (PA) as tested by von Frey hairs and brush allodynia (BA) in idiopathic intracranial hypertension (IIH) patients as well as non-allodynic patients. Allodynia in relation to actual severity of headache, during instrumental testing procedures.

Twenty-two of these 26 patients were examined one month to 10 years later after the lumbar puncture investigation. Eleven of them were found to be still allodynic, and eight had papilledema indicating elevated intracranial pressure at the time of investigation for allodynia. Four patients were tested at the same time with diagnostic lumbar puncture; allodynia was detected in three of them, showing no difference. Eighteen of 26 patients examined by instrumental testing had papilledema during the investigation; 11 of them were allodynic. On the other hand, five of eight patients without papilledema were non-allodynic. Thus the presence of allodynia did not significantly correlate to the presence of papilledema.
The demographic and clinical features of the IIH patients with and without allodynia are presented in Table 1 comparatively. Only the aggravation of headache with physical activity emerged as a significant variable associated with allodynia.
Nine IIH patients having complaints for less than three months were called the early-diagnosis group. Intracranial pressure (ICP) values were 475.5 ± 210, 4 mmH2O (mean 460, range 250–840), and five of them were allodynic. The remaining 37 patients with symptoms for more than three months were called the late-diagnosis group. Eighteen of them had allodynia with ICP values of 355.6 ± 114.2 mmH2O (mean 460, range 200–750). Five non-obese patients had an ICP in the range of 200–250 mmH2O; four of them were allodynic.
As a result, the presence of allodynia detected by ASC-12 questions or instrumental testing did not correlate to the time delay from debut of headache nor to the measured ICP level/papilledema. We further investigated the clinical features and the presence of allodynia and found that there were no significant differences between patients with and without MRV.
There were eight patients who had a diagnosis compatible with medication overuse headache at the time of IIH. Of them, four had a previous migraine, one had probable migraine and two had previous TTH. In this subgroup, six were allodynic; three patients cited mild allodynia according to ASC-12; one cited moderate allodynia together with BA and PA, one had only BA and the last one had BA and PA but did not report allodynia according to ASC-12 questions.
Seven of 46 patients were followed without medication because of remission of headache and papilledema. While 30 of the remaining 39 patients were taking only acetazolamide, seven patients received topiramate and two of them additionally had an antidepressant medication. We could not detect any significant difference of allodynia in patients given topiramate (seven allodynic versus two non-allodynic patients) in comparison to the patients not using this medication (16 allodynic versus 21 non-allodynic patients).
In the final analysis, we detected allodynic symptoms in 23 IIH patients; 20 of them reported migraine-like headache after onset of IIH, while three reported non-migrainous headache. Of 23 non-allodynic patients, headache was non-migrainous in 13 (p = 0.0045 and odds ratio (OR): 8.667 with Fisher’s exact test, two-sided using the approximation of Wolf).
Discussion
Headache is the main presenting and disabling symptom of IIH that is a well-established cause of secondary headaches. Despite this well-known fact, studies about the characteristics and associations of headache in IIH and its possible classification according to The International Classification of Headache Disorders (ICHD) are rare (15,16,20–22). Furthermore, allodynia in IIH patients was not reported before, even though this association could easily be expected because of some clinical features shared with primary headache patients with allodynia, such as being prevalent in obese females with a chronic headache pattern. We showed that allodynia as a clinical marker of central sensitization was present in half of the patients with IIH and associated with a migraine-like headache profile.
Headache profile of IIH
ICHD-II criteria required that a presenting headache could be attributed to IIH when the headache develops in close temporal relation to increased ICP and improves after withdrawal of CSF. The headache should be progressive with at least one of the following: (a) daily occurrence, (b) diffuse and/or constant non-pulsating pain or (c) aggravated by coughing or straining (18). The quality and location of the headache in IIH seemed to be rather uncharacteristic, however, but may resemble a fairly severe chronic migraine associated with daily visual non-aura symptoms and could be hemicranial or pulsatile (21) as also seen in our results. Moreover, our study supported the fact that patients with IIH often continue experiencing headaches, despite the apparent normalization of their ICP. Thus headache seemed to be a poor marker of IIH. The spontaneous ICP normalization further increases the possible delay in diagnosis in some cases. It was reported that 67% of 82 patients with IIH had headaches classifiable by ICHD-1 criteria after their initial presentation, diagnostic lumbar puncture and successful treatment for increased ICP (16). Thus, patients with IIH would not necessarily meet the IHS criteria in the strictest sense, but would otherwise fulfill the descriptors listed for the headache subtype assigned. Similar to the previous reports, our patients had mostly moderate or severe throbbing headache related to IIH accompanied by nausea and less frequently by vomiting (13,21,22).
Pathophysiology of IIH and its headache
Headache from raised ICP might be produced by displacement or irritation of pain-sensitive elements, including the venous sinuses, meningeal coverings, blood vessels and intracranial portions of the trigeminal, glossopharyngeal, vagus and upper cervical nerves. It seems reasonable to suggest that these changes also initiated the central sensitization related to allodynia in our patients with IIH. Episodic increase of ICP or plateau waves superimposed on a baseline of chronically elevated ICP are frequently associated with headache. This phenomenon may be related to traction on dural structures or distortion of the brainstem (23).
The pathophysiology of IIH is still not completely understood although several mechanisms such as parenchymal edema, increased cerebral blood volume, excessive CSF production, venous outflow obstruction or compromised CSF resorption and possible contribution of inflammatory factors have been proposed (21,24). Although IIH has been recognized for more than a century as a benign disorder except for the risk of blindness in a minority, some patients experience a chronic disabling course with continuing headache for years that limits their capacity to work and to participate in social life (21,22,25). Thus, pathophysiological studies are needed in order to optimize the biological understanding and therapy for this disabling chronic headache disorder.
Our findings indicate that IIH leads to a migraine-like headache in some patients, presumably by triggering some unknown mechanisms and causing allodynia, whereas IIH patients with non-migrainous headaches mostly do not have allodynia. Hence, not only the primary underlying pathological mechanism but also the associated features of headache and their pathological correlates could have some relationship to central sensitization and allodynia. According to ICHD criteria, headaches could not be diagnosed as migraine if they are attributed to another disorder. Thus IIH patients having migraine-like headache attacks (but not previous migraines) could not be ascribed easily to a co-existent migraine. However, we have the impression that IIH may trigger a “new-onset migraine” in some cases, which could persist for years after the remission of papilledema and normalization of CSF pressure. But this is a speculative hypothesis at this point, needing further studies.
The strongest and most consistent risk factors of IIH are obesity and female gender. However, our findings showed that neither CSF pressure nor BMI had any correlation with allodynia.
Allodynia in patients with chronic migraine
The patients with chronic migraine with allodynia were less likely to remit, and persistent chronic migraine had the largest incidence of severe allodynia according to ASC-12 studies (26). Thus studies suggested that central trigeminovascular neurons are chronically sensitized in patients experiencing migraine headache ≥15 days per month depending on the close relationship of chronic/transformed migraine with allodynia (9,27). The exact temporal and causal mechanisms that link allodynia and migraine frequency are poorly understood. The important points are whether the presence of allodynia has any prognostic or therapeutic significance in all kinds of headache patients and whether modifying the candidate risk factors for CA produces clinical benefits. Using preventive medications more aggressively to decrease headache frequency may therefore be desirable and may prevent CA to avoid central sensitization and prevent damage to the periaqueductal grey (PAG) in primary as well as in some secondary headaches like IIH.
Allodynia assessment and mechanisms
Allodynia has been evaluated using either a questionnaire (12) or instrumental testing (10,11,28) in several studies. The ASC measures overall CA and its subtypes retrospectively, and CA was found to be associated with frequency, severity and all associated symptoms of migraine (12). LoPinto et al. compared the prevalence of dynamic (brush) allodynia (32.7%) with a gauze pad and static (pressure) mechanical allodynia (32.7–43.6%) using von Frey hairs in migraine patients and found that PA was more common than BA, and there is a considerable although incomplete overlap (11). These findings were very similar to our findings of allodynia in IIH patients, indicating that the mechanisms and pathways responsible for allodynia modalities in migraine and IIH are possibly shared. Thermal allodynia (mediated by C nociceptive and A-delta nociceptive fibers) measured by questions of tap sensitivity to heat and cold (e.g. taking a shower, washing your face) was rare in IIH patients, but quantitative sensory testing was not applied in our study. BA, assessed by brushing the skin, was likely mediated by A-delta mechanoreceptive and capsaicin-insensitive A-delta fibers measured by questions about combing hair and pulling the hair back. Our results showed that this is the most frequent type of allodynia in IIH. Von Frey filaments have been used to assess static PA, which is mediated by A-delta nociceptive fibers, loaded on questions about pain while wearing earrings, a necklace, or tight clothing.
Association of allodynia and aggravation of headache by physical activity in IIH
The headache of IIH was aggravated by physical activity and, not surprisingly, that was significantly associated with the presence of allodynia. Pain aggravation by movement and avoidance of movement (kinesiophobia) are often reported by patients during migraine attacks. It is believed to be a sensitive and specific measure to identify migraine attacks when compared to tension-type headache (18,29). In contrast, aggravation of headache by physical activity was found to be associated with pure frequent episodic TTH in a large Danish study (30). Our study showed that 47.73% of patients with IIH also have this symptom associated with allodynia. The effects of Queckenstedt's maneuver, performed both in the upright and in the supine body position, were investigated in migraineurs during acute attack and supported a possible role for cerebral venous congestion in the generation of migraine pain and suggest body position may influence the clinical expression of that process (31).
Possible mechanisms underlying allodynia in IIH
Trigeminal pain-sensing neurons (nociceptors) innervating the dura are sensitive to mechanical stimulation in pain models (32,33). This may explain the worsening of headache in response to increased mechanical forces such as sudden head movements or increased ICP. Transient receptor-potential vanilloid 4 (TRPV4) is a possible candidate that contributes to the osmo- and mechanosensitivity of dural afferent nociceptors. Further, activation of TRPV4 within the dura of freely moving animals induced some behaviors (i.e. cephalic and extracephalic allodynia) that, interestingly, were blocked by an antagonist of the TRPV4 channel. Wei et al. speculated that TRPV4 contributes to the mechanosensitivity of dural afferents and may play a role in the worsening of headache during cough or changes in ICP (34). Other mediators such as bradykinin, histamine, serotonin and prostaglandin E2 have also been shown to produce both excitation and mechanical sensitization of meningeal nociceptors (35). Moreover, inflammatory mediators such as cytokines are believed to promote nociceptor sensitization (35). Assuming the recent suggestions of inflammatory contributions to the pathogenesis of IIH (24) are valid, these candidates could also be involved in the pathogenesis of IIH with allodynia.
There are some limitations of our study. Our study design was retrospective but we included a reasonable number of IIH patients who were diagnosed and followed-up in a single center and were systematically investigated for allodynia with many tools. Migraineurs were found to be sensitive to thermal stimulation during the interictal period (36), but, after applying ASC-12, we observed that IIH patients experienced mechanical allodynia much more than thermal allodynia. Considering that thermal allodynia is rare in the absence of other allodynia types, we did not investigate thermal allodynia with quantitative sensory testing, which could be cumbersome and time consuming. Extracephalic CA, which has been found to be mostly thermal type in migraineurs (37), has been reported by a minority of our IIH patients with ASC-12, as shown in Figure 2.
IIH is a chronic condition that may worsen after a period of stability, warranting long-term follow-up (22,25). One drawback of our study was that we could not investigate all patients at the time of diagnosis or during their most severe headache. In IIH, the headache is more or less chronic although varying in intensity, and a simultaneous recording of allodynia during the headache is complicated in a retrospective study. However, we showed for the first time that allodynia is present in half of the patients with IIH. More accurate knowledge of the prevalence and characteristics of allodynia in different headache forms may contribute to understanding changes in the physiological properties of nociceptive neurons that give rise to allodynia. This may have clinical implications, since allodynia may be associated with reduced triptan efficacy against acute migraine attacks (38). Allodynia is correlated with the frequency of migraine attacks (12), which may be decreased by preventive drugs, so there is a possible relationship. However, our IIH patients getting prophylactic medications did not report significantly fewer allodynic symptoms compared to the remaining patients.
In conclusion, we detected allodynia with migraine-like headache related to IIH. Mechanical stimulation of dural afferents by raised ICP together with the involvement of some unknown mediators may trigger the same mechanisms with migraine and lead to allodynia as well as a migraine-like headache in IIH patients.
Footnotes
Funding
This study was supported by the Istanbul University Scientific Research Fund (Project no. 5148).
Acknowledgement
We thank Erdem Tüzün for critically evaluating our manuscript.
Conflict of interest statement
The authors declare that there are no conflicts of interest.