
Abstract
Background
Secondary headaches attributed to exposure to or the overuse of a substance are classified under chapter eight in the International Classification of Headache Disorders 3rd edition. Three distinct sub-chapters consider: 1. Headache attributed to exposure to a substance, 2. Medication overuse headache, and 3. Headache attributed to substance withdrawal. Headache attributed to exposure to a substance refers to a headache with onset immediately or within hours after the exposure, while medication overuse headache is a headache occurring on 15 or more days per month that has developed as a consequence of regular usage of acute headache medication(s) for more than three consecutive months in a patient with a pre-existing primary headache disorder. The withdrawal of caffeine, oestrogen, and opioids is most often associated with the development of headache.
Discussion
Despite the current headache classification, there is no certainty of a causal relationship between the use of any substance and the development of headache. Some substances are likely to provoke headache in patients that suffer from a primary headache disorder like migraine, tension-type headache or cluster headache, while others were described to cause headache even in people that generally do not get headaches. Toxic agents, such as carbon monoxide (CO) are difficult to investigate systematically, while other substances such as nitric oxide (NO) were specifically used to induce headache experimentally. If a patient with an underlying primary headache disorder develops a headache, in temporal relation to exposure to a substance, which is significantly worse than the usual headache it is considered secondary. This is even more the case if the headache phenotype is different from the usually experienced headache characteristics. Medication overuse headache is a well-described, distinct disease entity with only marginally understood pathophysiology and associated psychological factors. Managing medication overuse headache patients includes education, detoxification, prophylactic treatments and treating comorbidities, which is reflected in available guidelines. Viewing medication overuse headache as a separate entity helps clinicians and researchers better recognise, treat and study the disorder.
Conclusion
Identification of substances that may cause or trigger secondary headache is important in order to educate patients and health care professionals about potential effects of these substances and prevent unnecessary suffering, as well as deterioration in quality of life. Treatment in case of medication overuse and other chronic headache should be decisive and effective.
Introduction
According to the International Classification of Headache Disorders 3rd edition (ICHD-3), headache is defined as secondary when it occurs for the first time in close temporal relation to another disorder that is known to cause headache or fulfils other criteria for causation by the disorder (1). In other words, a secondary headache is a headache co-occurring with another disorder that is recognised to be capable of causing headache. Two scenarios are possible. First, new onset headache occurs with a disorder that is known to cause headache. Secondly, the primary headache substantially worsens in temporal relation with another disorder known to cause headache.
These principles also apply to chapter eight of the ICHD-3 – headache attributed to a substance or its withdrawal (1). Diagnosis of a “headache attributed to use or exposure to a substance” requires a) scientific evidence (clinical experience and pathophysiological concept) that the substance causes headache and b) temporal relation between the use of the substance and the onset of the headache. The headache must develop or worsen with the use of the substance and it must significantly improve or resolve after the cessation of the exposure. This chapter is further divided into headache attributed to use of or exposure to a substance, medication overuse headache (MOH) and headache attributed to substance withdrawal.
We summarize the currently existing scientific evidence about secondary headaches attributed to exposure to or overuse of a substance as well as its withdrawal. A MEDLINE search (15 January 2020) for articles containing “secondary headache” OR “medication overuse headache” was performed. The search returned 1118 articles, of which 358 were marked as review articles. We focused on the most recent articles of the past 5 years, which consisted of 481 articles of which 128 were review articles.
Headache attributed to use of or exposure of a substance
Classification and epidemiology
Headache attributed to use of or exposure to a substance is defined as a headache caused by exposure to a substance with onset immediately or within hours after the exposure. The ICHD-3 further classifies the substance-induced headaches according to the substances that precipitate it. For details of classification criteria and clinical characteristics of headaches attributed to different substances such as nitric oxide (NO), phosphodiesterase, carbon oxide (CO) and others, we refer to chapter eight of the ICHD-3 (1).
There is a substantial clinical evidence supported by pathophysiological knowledge and clinical observation that substances such as NO donors (2), cocaine (3), or phosphodiesterase inhibitors (4) can cause headache in healthy people. In these cases, the causal relationship between the use of a substance and headache and subsequently the diagnosis of secondary headache is easy because healthy subjects without a previous history of headache develop it in temporal relationship with use of a substance or medication. In this case, it is easy to argue in favour of a secondary headache as a separate entity. It is also supported by clinical observation if headache resolves later and if it re-occurs when this person is exposed to the same substance again. However, the latter demands following the patients and may not prove to be a very useful diagnostic criterion in everyday clinical practice. However, the association of a particular substance and the occurrence of headache does not prove their causal connection and different aetiologies of the headache must be considered. The parallel occurrence of headache and substance intake may simply be a coincidence, as common symptoms are frequent, headache may have occurred by chance and may be totally unrelated to the previous exposure to any described substance. The headache may also be a symptom of a systemic disease unrelated to the drugs given to treat the underlying condition. Nonetheless, it will be described as associated with headache.
It also must be taken into account that the prevalence of headache is very high in the general population and subjects can experience more than one headache type. Patients with migraine are well known to be more sensitive to certain stimuli that may trigger a migraine attack. Hence migraine patients will suffer from headache more easily following exposure to certain substances than others. Some substances may lead to headache regardless of the presence or absence of an underlying primary headache disorder. This is also reflected in the ICHD-3: Two separate diagnoses should be given whereat an exposure to a substance resulted in a different headache phenotype than would normally be associated with their primary headache disorder (1).
Pathophysiology
The same substances (e.g. NO donors or phosphodiesterase inhibitors) provoke attacks of pre-existing migraine or tension-type headache (5,6). Causal relationship here is supported by the current pathophysiological concept and the fact that provoked attacks and non-provoked attacks are phenotypically identical. It can be argued however, whether the provoked attack should be classified as a worsening of primary headache due to substance exposure as a separate entity of secondary acute headache attributed to the substance. If the phenotype is clearly different from the previously experienced attacks, it is more likely that this particular episode of headache is not directly one of the underlying primary headache and represents an episode of a new acute secondary headache attributed to the substance.
For example, NO has been shown to provoke immediate headache and delayed migraine attack in people with migraine but also in healthy subjects (7,8). NO-induced mechanisms causing headache are complex and include vascular and neuronal aspects. NO causes vasodilation through the cyclic guanosine monophosphate cascade and promotes dural vasodilation (9). There is evidence that NO also releases calcitonin gene-related peptide (CGRP) from rat’s dural afferents, which in part mediates an increase in meningeal blood flow (10). Furthermore, NO is implicated in the neuroimflammatory cascade of migraine headache (11). And finally, in animal models, NO has been shown to be involved in central nociception and to increase pain responses (12).
Treatment
Evidently, the most effective treatment is the cessation of substance exposure that is responsible for the headache. In some cases, additional therapy is required to expedite the regeneration process, and should either be purely symptomatic or be adapted to the presenting headache phenotype.
The utility of the GTN model has been discussed extensively in animals and humans, both for the understanding of pathophysiology and for the screening and testing of therapeutic drugs (13). Nitroglycerin (NO donor) induced migraine has been aborted or averted successfully by several acute antimigraine drugs of differing mechanisms, including prednisolone, sodium valproate and sumatriptan (14–16). Nitric oxide synthase inhibitors have been extensively studied as potential effective antimigraine drugs (17,18).
Medication overuse headache
Classification and epidemiology
As defined in the ICHD-3, MOH is a headache occurring on 15 or more days per month in patients with a pre-existing primary headache disorder and developing as a consequence of regular use of acute or symptomatic headache medication(s) for more than three consecutive months (1). Patients with MOH are mostly women, on average 40–45 years old. Most of them have migraine, some have tension-type headache or a combination of both. On average, they have suffered from primary headache for 20 years and overuse medication for about 5 years (19). Population-based prevalence studies demonstrated that about 0.5–2% of the general population suffer from chronic headache combined with overuse of headache medication (20–23). MOH is associated with low socio-economic status (24,25). This is even more pronounced in countries with large socio-economic disparities (26,27). Personal or family history of migraine or tension-type headache, as an underlying biological trait, is the most important factor for developing MOH (28,29). Another important risk factor is overuse of any kind of headache medication (30). Further risk factors include musculoskeletal pain, depression, and family history of substance abuse (31–33). MOH is associated with depression and anxiety, obsessive-compulsive disorder, obesity as well as sleep complaints (34–38).
Pathophysiology
Pathophysiology of MOH is still poorly understood. Genetic studies described candidate polymorphic variants in genes of the dopaminergic gene system (DRD4, DRD2, SLC6A3), and genes related to drug-dependence pathways (WSF1, BDNF, ACE, HDAC3) as possible determinants for MOH susceptibility or of frequent drug consumption (39). Chronic administration of triptans or analgesics results in abnormal modulation of the serotoninergic system, sensitization of different nociceptive pathways and even structural changes in particular brain regions, such as the ventromedial prefrontal cortex (VMPFC), the nucleus accumbens and the substantia nigra/ventral tegmental area (40–45). The pathophysiological mechanisms associated with the development of MOH are comparable in some parts to dependence mechanisms and addictive components that are generally associated with psychiatric disorders (46). Interestingly, these functional and structural changes may reverse after withdrawal (44–46). Changes in pain processing networks, dependence networks, sensitization of pain pathways and changes of receptor density in the CNS presumably explain the underlying pathophysiology of the disorder in a complex, orchestrated manner with inter-individually different degree of influence but a common phenotypic presentation.
Despite the availability of some fundamental studies that tried to unravel the complex mechanisms associated with the development of MOH using neuroimaging or laboratory techniques, there are no clearly defined unique changes that can be interpreted and agreed on to serve as biomarkers of MOH. Hence, diagnosing MOH remains a clinical diagnosis on the basis of the currently available and generally accepted diagnostic criteria of the ICHD.
Prevention
Education about the relationship between an excessive use of acute medications and development of MOH is an important preventive measure. Most MOH patients have little to no knowledge about the connection between excessive drug intake and headache chronification. National awareness campaigns using online resources, print media, radio interviews, and television broadcasts can effectively reach the general public, GPs and pharmacists and deliver key messages, such as overuse of pain medications can worsen headaches, pain medications should be used rationally and MOH is treatable (47). Information brochures can be effectively used in large population settings and significantly improve clinical outcome in people overusing headache medications (48).
Treatment
An overview of trials and outcome studies is presented in Table 1 (49–60).
Trials and studies on medication overuse headache.
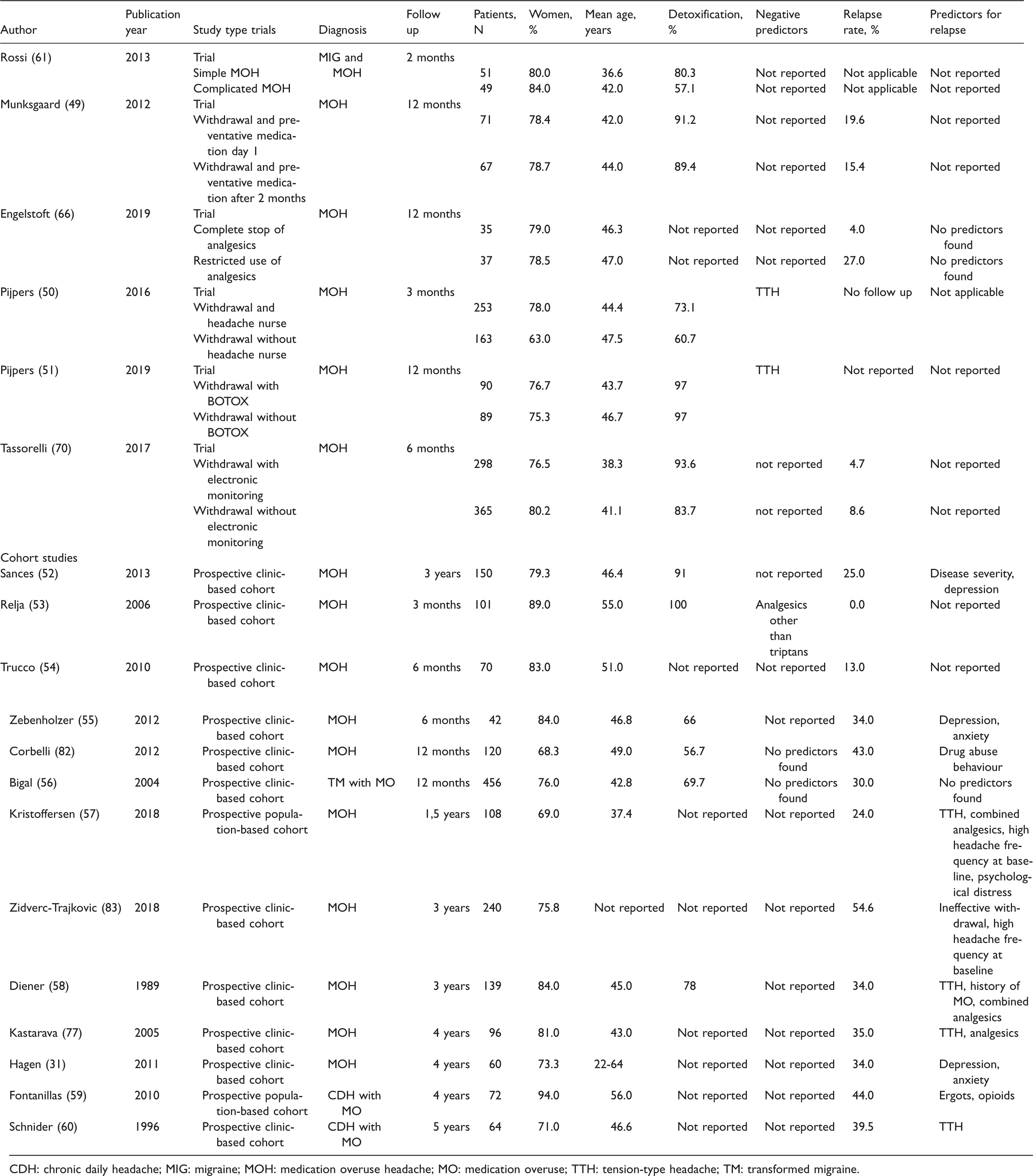
CDH: chronic daily headache; MIG: migraine; MOH: medication overuse headache; MO: medication overuse; TTH: tension-type headache; TM: transformed migraine.
Discontinuation of the overused medication is essential in the treatment of MOH. First, the setting for withdrawal should be decided. The choice is between outpatient and inpatient treatment and depends on many factors such as patient’s motivation, the duration of the overuse, the type of overused drugs, possible previous detoxification failures and comorbidities. An outpatient detoxification can be preferred for highly motivated patients, with a short duration of overuse of simple analgesics and supportive familial environment. Inpatient withdrawal is recommended for patients overusing more complex analgesics (such as opioids, tranquilizers or barbiturates), long duration of overuse, previous failure to withdraw drugs as outpatients and psychiatric comorbidities (19).
Some studies demonstrated that advice alone can be enough and achieve improvement in patients with MOH (61,62). Most headache centres prefer abrupt drug discontinuation for single analgesics and triptans because it does not result in severe withdrawal symptoms, and gradual reduction for benzodiazepines and opioids (63–65). One randomized controlled open-label trial demonstrated a superiority of complete discontinuation compared to restricted drug intake (66,67).
Preventative treatment of the underlying primary headache disorder should be started in parallel to withdrawal. Some authors suggest withdrawing patients first, because in many of them headache improves dramatically, so that the choice of preventative medication can be adapted accordingly. Others argue to start prevention together with withdrawal treatment in order to gain the most benefit out of concurring interventions (68). Recently, after the introduction of effective preventative treatments for chronic migraine such as topiramate, onabotulinum toxin A and monoclonal antibodies targeting CGRP, some authors argued that withdrawal treatment may not be necessary, because effective prevention will improve headache anyway (69). The majority of headache experts, however, consider discontinuation of medication overuse as an essential part of treatment. The COMOESTAS consortium clearly demonstrated that multimodal treatment of MOH including withdrawal and electronic alert system was very effective and improved clinical outcome, significantly reduced direct health care costs and increased patient productivity (70–71). A recent placebo-controlled trial on botulinum toxin A in patients with MOH demonstrated that withdrawal was essential for treatment success, because withdrawal plus onabotulinum toxin A was not more effective than withdrawal alone (72).
Treatment of psychiatric comorbidities has important implications for the management of MOH. Co-existence of mood disorders may lead to poorer adherence to headache treatment, leading to an unsuccessful overall outcome. Comorbid psychiatric disorders add to the overall disease burden, reduce quality of life in headache patients, and may lead to poorer outcomes despite proper treatment. Therefore, a multi-professional approach including withdrawal, preventative medication and psychological support as well as lifestyle modification is the most effective setting for the treatment of patients with MOH (73).
Outcome
Overuse of acute treatment can lead to a poor prognosis of chronic headache and lower quality of life by itself (74). The outcome of patients with MOH is good, about 50–70% of them improve (75). A substantial amount of the patients, however, relapse within 5 years after withdrawal (76–79). The majority of patients relapse during the first year, indicating the first year after withdrawal as being especially critical, and close monitoring is advised to prevent relapsing (77). Predictive factors for relapse were identified as being a combination of migraine and tension-type headache as well as the overuse of opioids (77).
Critical considerations
There is an ongoing debate on the concept of MOH, whether it should be considered as a separate entity or simply represents the worsening of migraine or tension-type headache due to an overuse of headache drugs. This debate influenced the working group of the Classification Committee of the International Headache Society and also reflected pros and cons on withdrawal strategies (69,80).
The authors of this manuscript consider MOH as a separate clinical entity that occurs secondary to a primary headache disorder in those who are predisposed. Diagnostic criteria for MOH have evolved with our understanding of the condition and have also become more practical over time – the latter versions of the ICHD underwent changes including removing the retrospective criteria – allowing practitioners to diagnose MOH already during the first consultation and start appropriate management immediately. Without considering MOH as a distinct disorder, it will be impossible to generate guidelines specifically designed to treat it (64).
In addition, MOH is of great importance as a debilitating condition on a public health level – the Global Burden of Disease 2016 study counted migraine as the second largest cause of disability also because MOH was considered to be a sequela of migraine and tension-type headache (81). Thus, bringing it out as a separate entity in the classification of headaches underlines the gravity of this condition and precise diagnostic criteria help clinicians and researchers better recognise, treat and study the disorder.
However, more data are still needed to address a number of unanswered questions at each level. The clinically known fact that MOH has never been shown to develop without having a background of some primary headache disorder can also be viewed as an argument against its existence. In other words, MOH can represent a complication of a primary headache, in which case it can be a part of a “medications-facilitated” process of chronification of the primary headache disorder itself. After all, progression of primary headache disorder from episodic to chronic can take place without overusing acute medications. In this scenario, such a situation might not be in need of specifically generated diagnostic criteria and/or treatment guidelines (like detoxification) and the goal of the treatment would be concentrating only on treating a (chronic) primary headache syndrome. It is also known that detoxification does not always work – the absence of efficacy after pure withdrawal may contradict the concept of MOH as a separate entity. However, it must be mentioned here that available studies rather indicate that the majority of detoxified patients improve, many returning to the frequency of headaches reported before reaching thresholds of overusing. Nevertheless, failure to achieve improvement after a detoxification should not lead clinicians to the conclusion to continue analgesic acute treatment without limitations – overusing analgesics still represents a poor prognostic factor in chronic and high-frequency episodic primary headache disorders (19).
Article highlights
In a vast majority of instances, headache attributed to use of or exposure to a substance is rather easily diagnosed based on the history and clearly belongs to a subgroup of secondary headaches. Withdrawal of caffeine, oestrogens, and opioids is most often associated with the development of secondary headache. Medication overuse headache is considered to be a secondary headache that develops as a result of regular intake of acute or symptomatic medication(s) used to treat an underlying – usually chronic – primary headache.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.