
Abstract
Background and Objectives
Prolonged screen exposure is often cited as a trigger for pediatric headache. We present initial findings evaluating the association between adolescent screen use type, duration, and school disability.
Methods
New patients aged 12–17 years presenting to a headache clinic were screened and surveyed regarding headache characteristics, behavioral habits, school attendance, and screen utilization.
Results
99 adolescents (29 M, 70 F) with average age 14.8 years and average headache frequency of 17 days per month completed the survey. Patients missed an average of five full days and three partial days of school due to headaches over the 90 days prior to survey completion.
No statistically significant correlation was found between type or duration of screen exposure and monthly headache frequency, school attendance, or school functioning. A small positive association was seen between increasing duration of computer use, total hours screen use, and school absenteeism. While most adolescents reported prolonged screen use (58.6%) and luminosity (64.6%) worsened headaches, no statistical difference was seen in average number of headache days per month.
Conclusions
Average monthly headache frequency in an adolescent population was not significantly correlated with type or duration of screen exposure. Further studies are needed to elucidate how screen utilization impacts school related headache disability.
Introduction
Frequent or severe headache has an estimated prevalence of 6% in children aged 5–17 years in the United States (1). These children often experience functional limitations in daily activities including school attendance and the pursuit of hobbies (1,2). Previous research has demonstrated reductions in quality of life among pediatric migraine patients including scholastic and emotional functioning as equivalent to or greater than those seen in pediatric patients with rheumatoid conditions, cancer, and other chronic illnesses (3).
Because of the extensive disease burden associated with pediatric headache, analysis of headache triggers represents an important area of pediatric research. The presence of intense light stimuli and complex visual stimuli for example, have been linked to migraine development (4). Given the visual complexity and luminosity associated with electronic screen use, this connection has prompted investigation into screen exposure and headache development within the pediatric population.
Screen use and exposure are often reported by patients and families as a trigger or exacerbating factor for headaches. Rossi et al. (5) analyzed a sample of 320 children aged 3-14 years with recurrent or chronic headaches in the Milan region of Italy between 1996 and 1999 where all children were asked to complete a questionnaire concerning the location and type of headaches experienced, associated symptoms, and precipitating factors. Results indicated exposure to computers or television was a precipitating factor for headache in 30.7% of those with migraine with aura, 22.6% in those with migraine without aura, and 3.8% in those with tension-type headache (5). Similarly, a study evaluating the prevalence of headache triggers in a clinic-based pediatric migraine population (n = 102) found that video gaming was the fourth most common individual trigger in 64.7% of the patients (6). Headache has also been found to occur more often in children who watch television longer and there is further evidence to suggest increased risk of headaches with the number and duration of cell phone and cordless phone calls in adolescents (7,8).
Additional studies have led to conflicting evidence regarding screen exposure and headache development. A population-based, cross-sectional study of 13-year-olds in Finland evaluated the associations between different types of headache and leisure activities. The study included 59 children with migraine, 65 children with episodic tension-type headache, and 59 headache-free controls. While the type of leisure activity was not significantly correlated with headache type, the children with migraine and episodic tension-type headache were found to use computers more often than children without headache. Further analysis also demonstrated that one additional day of computer usage in a week significantly (p = 0.02) raised the odds of belonging to the migraine group (20% increase) and the tension-type group (30% increase), as compared to controls (9). Likewise, another population-based study of 1025 adolescents aged 13-17 years in Germany investigated the association between use of different types of electronic media (mobile phones, computer, playing with game consoles, watching television, listening to music) and headache. In this study, the prevalence of any type of headache increased with increasing duration of listening to music daily (p = 0.0026); though, no other statistically significant associations between the use of electronic media and different headache types were found (10). A more recent cross-sectional study of young adults (mean age of 20.8 years) in France demonstrated that participants in the highest screen time exposure quintile had an increased risk for migraine; however, there was no meaningful association found between screen time exposure and non-migraine headache (11).
There are limited data suggesting a positive association between screen use and headache in pediatric patients and there remains an overall paucity of knowledge in this area with a lack of understanding in terms of how screen exposure may additionally impact headache-related disability, including headache frequency and daily functioning especially related to school, in these patients. With this gap in the literature in mind, we conducted our current study to further evaluate the association between adolescent screen exposure–particularly in terms of screen use type and duration–and school related headache disability. We hypothesized that adolescents with the highest reported screen use would experience increased self-reported headache frequency as well as increased school absenteeism and impaired school functioning.
Methods
Participants
This pilot study was approved through the Institutional Review Board of Children’s National Hospital. All new patients aged 12–17 years presenting to the Headache Clinic at Children’s National Hospital at the Sheikh Zayed Campus from August 2017 to August 2018 were invited to participate in the study as a convenience sample. Exclusion criteria included patients less than 12 years of age, follow-up patients, and patients with significant developmental delay or intellectual disability precluding their ability to independently complete the study survey. Written informed consent was obtained from participants’ parents. All study participants also documented assent to participate in the study. In-person certified interpreters were present for all study activities including consent, assent, and survey translation for non-English speaking patients.
Measures
All eligible study participants were asked to individually complete a written survey comprised of 20 questions regarding headache frequency over the preceding three months, headache characteristics, behavioral habits, school attendance and functioning, and screen utilization. The survey was created internally for this pilot study and is not validated.
Television watching, computer use, cell phone use, video gaming, and tablet use comprised the technology types assessed and correlated with headache frequency. Screen use was evaluated within a single day (24 hour) period. Participants were asked to report their screen utilization for all devices listed (television, cell phone, computer, video games, tablet) by choosing one of the following time categorizations: 0 hours per day, less than 2 hours per day, 2–3 hours per day, or greater than 4 hours per day. Total screen time was evaluated by taking the midpoint or the minimum of a response option by device and summing the results.
To evaluate school related disability, patients were asked to report full days of school missed, partial days of school missed, and days with less than half normal functioning in school over the preceding three months.
Analysis
Comparisons of headache frequency on questions of headache location and other binary responses were calculated using the Wilcoxon Mann-Whitley nonparametric test due to the skewness of the distributions. For responses with more than two options the Kruskal-Wallis nonparametric test was used. For comparisons of continuous measures (e.g., television usage) with headache frequency we used the Spearman Correlation Coefficient. Box plots were also provided to show differences in distribution of headache frequency for selected patient characteristics. Chi-squared statistics were calculated when comparing two categorical measures (e.g., public/private vs type of internet use).
Results
A total of 371 patients were seen at the Children’s National Headache Clinic at the Sheikh Zayed campus between August 2017 and August 2018. Of this number, 99 patients (29M, 70F) met inclusion criteria and agreed to participate in the study. The most common reason for failure to participate was lack of time. No patients screened over this period met the exclusion criteria for intellectual disability/developmental delay.
Patient Demographics
Study participants were mostly female (70%) with an average age of 14.8 years (Table 1). Headache frequency amongst participants averaged 17 days per month with a median headache frequency of 15 days per month. Headache pain was most frequently localized to the frontal head (57%), bitemporal head (49%), and behind the eyes (35%). Pain quality was described as throbbing (82%) and pressure like (61%) in most patients. Common associated headache symptoms included photophobia (81%), phonophobia (64%), lightheadedness (55%), and nausea (54%). Migraine was the most common primary headache diagnosis amongst our study population with chronic migraine without aura in 33%, migraine without aura in 29%, and migraine with aura in 15%. A family history of headache was present in 70 patients with 87% of those endorsing a positive history of migraine.
Patient demographics (n = 99).

A majority of patients endorsed wearing corrective lenses with either glasses or contacts (54%). Headache frequency was not found to be statistically different amongst those patients wearing corrective lenses (p = 0.946).
Screen use and headache frequency
We found no statistically significant difference between the duration of screen use or type of screen utilized (television, computer, cell phone, video game, tablet) with respect to the average monthly headache frequency among our study population (Tables 2 and 3). Similarly, total hours of screen use spent on devices was also not found to correlate with monthly headache frequency (p = 0.344) (Figure 1). In analyzing total hours of screen use spent on devices by headache diagnosis, there was no difference seen in total screen time across the different diagnostic categories (p = 0.881). While most patients reported that prolonged screen use (58.6%) and lighting from screens (64.6%) worsened their headaches, no significant difference was seen in headache days experienced per month (Figure 2). In those patients reporting headache worsening with prolonged screen use, total hours of screen use spent on devices was not significantly correlated with headache frequency (p = 0.252).
Duration of screen use by device and monthly headache frequency.

p-value based on Kruskal-Wallis test.
Screen device type and monthly headache frequency.


Total hours of screen use and monthly headache frequency.

Subjective report of screen use and luminosity worsening headache and monthly headache frequency.
Screen use and school related headache disability
Patients reported missing an average of five full days (M = 2) and three partial days (M = 1) of school due to headaches over the preceding 90 days prior to survey completion. A small positive association (p = 0.038) was seen between increasing duration of computer use (4+ hours/day) and days of school missed (see Table 4). No other statistically significant correlations between device type and duration of screen use were found with respect to school attendance or school functioning.
Screen use by device and full school days missed due to headache.
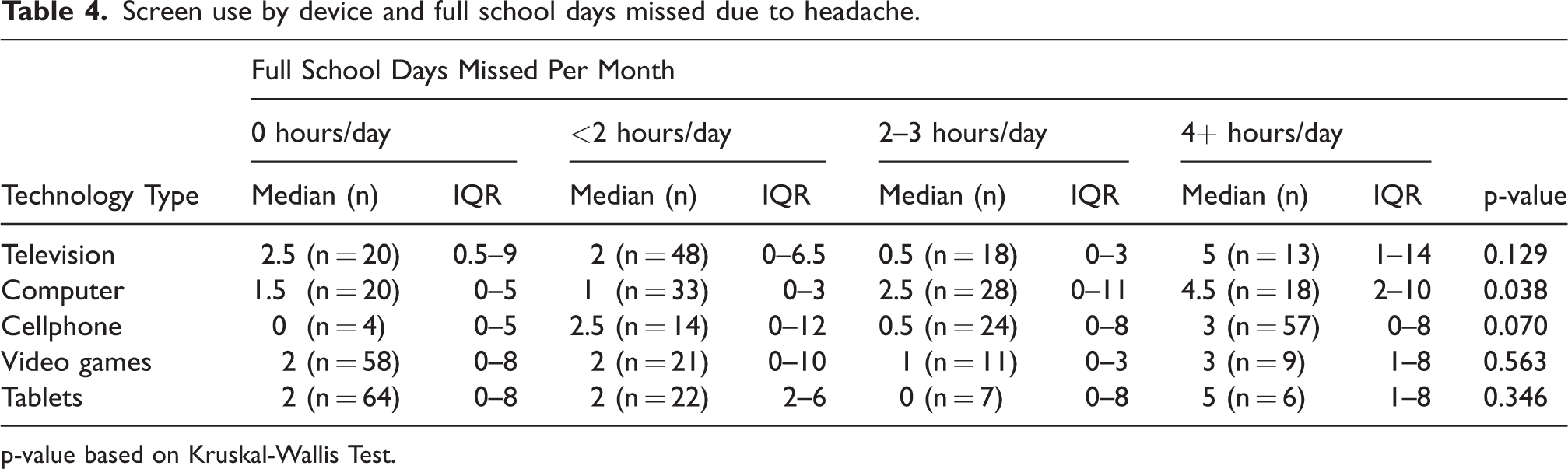
p-value based on Kruskal-Wallis Test.
Similarly, there was no statistical correlation seen between total hours of screen use spent on devices and partial school days missed (p = 0.430). However, there was a correlation of 0.24 with full school days missed which did meet statistical significance (p = 0.016) (Figure 3).

Total hours screen use and full/partial school days missed due to headache.
Likewise, in comparing patients with and without corrective lens use, there was no significant difference seen in full school days missed due to headache (p = 0.320), though significance was achieved for partial school days missed due to headache (p = 0.023). Yet, in evaluating combined full and partial school days (assuming a partial day is equal to half of a full day) missed amongst patients with and without corrective lens use, significance was not demonstrated (p = 0.135).
Discussion
Previous research investigating the association between pediatric screen exposure and headache disability has yielded varying results. Perhaps due to patient reports that screen use can be a headache trigger, many unique approaches to the question have been utilized in efforts to clarify what the relationship might be, if one exists at all.
Interestingly, our findings did not demonstrate a statistically significant correlation between device type or duration of screen exposure (including television, computer, cell phone, video games, and/or tablets) and monthly headache frequency, school attendance, or school functioning. A previous study conducted by Suris et al. (12) assessing whether problematic internet use was associated with various somatic complaints including headache, also did not demonstrate statistical significance. In the Suris’ study, a random sampling of adolescents in Switzerland between April and July 2012 was conducted via a cross-sectional survey of 3067 mean age of 8th graders 14 years. Participants were divided into average (n = 2708) and problematic (n = 359) internet user classifications by the Internet Addiction Test (IAT) and compared for somatic complaints including back pain, weight problems, headache, musculoskeletal pain, sleep problems, and sight problems. While results of the initial bivariate analysis indicated that 15.3% of average internet users reported headaches, 27.2% of problematic internet users reported headaches; however, at the multivariate level, headaches associated with problematic internet use did not remain statistically significant (12).
Moreover, our data did not show a significant correlation between total hours of screen use and monthly headache frequency nor a difference in total hours of screen use by headache diagnostic category. This contrasts the aforementioned 2016 findings of Montagni et al. (11) who in their study of French young adults found participants in the highest screen time exposure quintile were at an increased risk for migraine. Yet, our study data appears comparable with the population-based cross-sectional study conducted by Cerutti et al. (13) in Central Italy from February 2013 through June 2014 to determine whether migraine or tension-type headaches were associated with abuse of the internet and/or mobile phones and to evaluate if technology abuse was associated with sleep disturbances and other reported somatic symptoms. In this study headache was reported in 28% of the total sample (n = 841). 39.6% of study subjects were non-abusers of both technology types, 26% were found to abuse mobile phones only, 14.9% internet only, and 19.5% were found to be abusers of both media types. There was no significant relationship found between students with and without headache and abuse of the internet and mobile phones. After excluding the no headache group, headache type (migraine and tension-type headache) was also not found to be statistically correlated with the abuse of media (13).
Notably, our study did find a small positive association between increasing duration of computer use (4+ hours/day) and school absenteeism as well as a correlation between total hours of screen use and full days of school missed, though not partial days of school missed. In their cross-sectional association analysis of screen-based activity and physical complaints among a sample of 31,022 Nordic adolescents in the Health Behavior in School-aged Children 2005/06 (HBSC) study, Torsheim et al. (14) evaluated daily hours spent on screen-based activities and levels of physical complaints by participant self-report. Results demonstrated recurrent headache ranging from 15–31% in boys, and 26–44% in girls. Boys’ computer use, computer gaming, and television viewing were associated with increased odds of headache, as compared to computer use and television viewing in girls. Television viewing, computer use, and video gaming for three hours or longer were also associated with increased headache frequency. Overall, the study found that time spent on screen-based activities is a potential contributing factor to physical health complaints, including headache (14). Similarly, Bener et al. (15) performed a cross-sectional study of 1400 school children aged 6–14 years, of United Arab Emirates nationality between October 1995 and June 1996 to assess the genetic and environmental factors associated with migraine and headache. A total of 1159 (82%) of the children consented to participate and data was collected using screening questionnaires followed by confirmatory clinical interviews. In this study, 13.7% (159) of children fulfilled International Headache Society (IHS) criteria for migraine. In the children with migraine, results indicated the most common environmental exposure was playing at the computer (45.9%, n = 79). Results of logistic regression analysis of migraine and potential associated environmental factors also demonstrated a relative risk of 2.20 (p = 0.0487) for long hours watching television and a relative risk of 1.98 for playing at the computer (p = 0.0280) (15). Earlier associations between prolonged computer use and headache have previously been suggested by Palm et al. (16). In their study evaluating associations between computer use and health complaints in teen students, working on a personal computer or playing personal computer games more than three hours was found to significantly increase chances of headache compared to those with less use (16). While our findings are indicative of positive associations between more prolonged computer use and total hours of screen use and school absenteeism, these findings must be cautiously interpreted in light of the current study design and size.
Whereas most adolescents in our study reported prolonged screen use (58.6%) and luminosity (64.6%) worsened their headaches, no statistical difference was reflected in the average number of headache days experienced per month (p = 0.76 and p = 0.87 respectively). This may in part be due to some patients utilizing screen activities as a distraction technique or relaxation tool in the setting of acute headache pain or worsening, which may then be perceived as mitigating or non-contributory. For example, previously reported benefits of screen and media use in children have included exposure to new ideas and knowledge as well as opportunities for social interaction (17).
The present study has several limitations. First, the study represents a small sample size that may not be sufficient to detect meaningful differences in screen usage patterns. Our findings may also not generalize to patients younger than 12 years of age, whose patterns of screen use may not be reflective of those seen in this study. In addition, external validity of this study may be limited as children attending a specialized headache clinic may present differently as compared to children seen in general pediatric clinics for headache. Also, a majority of patients reported corrective lens use with either glasses or contacts, which may have influenced their susceptibility, and perceptual pain experience related to screen use. While our findings did not demonstrate a statistically significant difference in headache frequency amongst those reporting corrective lens use, considering our sample size, further studies would be necessary to validate this finding. Moreover, we did not specifically clarify if corrective lens wear included use of tinted lenses, prism, or blue light spectrum blockers which may be utilized by some patients to help alleviate headache attributed to screen-based sensitivity.
Furthermore, the retrospective nature of the study model/questionnaire may introduce recall bias in how patients responded to survey questions, particularly in terms of self-reported screen use and headache disability. The questionnaire requested screen time reported in estimated hourly blocks as opposed to the exact duration of screen use and exposure and was not validated prior to administration. The timing of survey administration may have also played a role in patient-reported headache frequency or perceived headache-related school disability. For example, students completing the survey over the summer or during a school vacation may have lower reported headache frequency and disability in comparison to other times of the year. While this is a recognized limitation, it should be noted that in our current study, a minority of patients completed the survey over the summer months July through September. Of the 18 participants who completed the survey over these months, 13 were enrolled in school for a period of one-month or longer over the preceding 90-day period with respect to our regional academic calendar. Likewise, as there are a wide variety of screen-based technologies currently available, this study did not consider all such technology types by only including television, computer, cell phone, video games, and/or tablet use. By excluding devices such as smart watches or electronic readers this may have influenced a patient’s reported screen usage. Specific screen size and luminosity factors were also not accounted for in the present study. Similarly, the survey did not address multi-screen use patterns (i.e., using a cell phone while watching television), referred to as “media multitasking,” which may result in an incorrect estimation of the total duration of screen exposure and lead to differing effects on headache frequency and disability ratings.
Additionally, the present study did not survey other possible factors such as ambient lighting or patient positioning with screen use which may have impacted a patient’s self-reported headache experience. Previous studies in young adults have indicated associations between prolonged computer use of three hours or more per day with neck/shoulder pain and headache (18), and a more recent school-based cross-sectional study in Malaysia indicated lying position and darkroom lighting with electronic device usage as potential predictors of physical and behavioral complaints (19).
Finally, the current study was conducted over a one-year period 2017 to 2018 and is insufficient to evaluate how adolescent screen use and headache patterns may change and evolve over time. With the onset of the global COVID-19 pandemic in 2020, there was a rapid and marked transition to virtual and screen-based platforms for nearly all activities of daily living related to learning and work. For instance, in their large cross-sectional national sampling of 5412 adolescents over the pandemic, Nagata et al. (20) found mean total daily screen use of 7.7h/day increased from 3.8h/day pre-pandemic. Preliminary survey data from these authors received from 113 headache patients seen over Summer 2020 to Winter 2021 also indicated an increase in headache frequency in approximately 45%, with one-third of patients reporting screen use for school >6 hours per day, and worsened headache with screen use in up to 62% (21). Thus, it will be important for future prospective long-term analyses tracking adolescent screen usage and headache disability to take into account sociocultural factors that may significantly impact behavior.
Conclusions
Overall, this study did not demonstrate a positive correlation between type of screen use, duration of screen use, and average monthly headache frequency in an adolescent population between the ages of 12-17 with a history of headache. A small positive correlation between increasing duration of computer use (>4 hours/day), total hours of screen use, and school absenteeism is reported. Despite these findings, adolescents surveyed believed that duration of screen exposure (58.6%) and screen luminosity (64.6%) worsened their experience of headache. This study adds to the pediatric headache literature by supporting a lack of clear association between screen use and headache development, as well as inconclusive evidence between screen use and school impairment, among an adolescent population. Future prospective, longitudinal studies utilizing real-time screen monitoring through application-based technologies are needed to better understand childhood and adolescent screen use patterns and how they may influence the self-reported patient experience of headache.
Clinical Implications
Average monthly headache frequency in adolescents aged 12–17 years was not significantly correlated with type or duration of screen exposure. Despite this, most adolescents reported prolonged screen use (58.6%) and luminosity (64.6%) worsened their headaches. Considering these findings and the widespread adoption of virtual learning, further studies are needed to elucidate how daily, monitored screen utilization impacts pediatric headache disability.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024221113468 - Supplemental material for Pediatric screen exposure and school related headache disability
Supplemental material, sj-pdf-1-cep-10.1177_03331024221113468 for Pediatric screen exposure and school related headache disability by Raquel Langdon, Alexandra Mandel, Mark Cameron, Emily Pierce, Emily McCracken, Jeffrey Strelzik, William McClintock, James Bost and Marc DiSabella in Cephalalgia
Footnotes
Acknowledgements
The authors would like to thank Sharon Sorto, Jessica Keats, Mary Furda, and Marni Jacobs for their support of the current study. The authors alone are responsible for the content and writing of this publication.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial or grant support from any funding agency in the public, commercial, or not-for-profit sectors for the research, authorship, and/or publication of this article.
Ethic Approval and Patient Consent
This study was approved by the Institutional Review Board of Children's National Hospital. Written informed consent was obtained from participants' parents and documented assent from all study participants prior to study participation.
Supplemental material
Study survey to be made available as supplemental material online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.