
Abstract
Objectives
To compare the effects of acupuncture and medical training therapy in combination or individually with usual care on quality of life, depression, and anxiety in patients with tension-type headache.
Methods
In this single-center, prospective, randomized, controlled, unblinded trial, 96 adults (38.7(+/−13.3) years of age; 75 females/20 males/one dropout) with frequent episodic or chronic tension-type headache were randomized to one of four treatment groups (n = 24). The treatment groups received six weeks of either acupuncture or medical training therapy as monotherapies or in combination (12 interventions each), or usual care. We assessed depressiveness (PHQ-9), anxiety (GAD-7), and health-related quality of life (SF-12) as secondary outcome parameters at baseline, six weeks, three months, and six months after initiation of treatment. Linear mixed models were calculated.
Results
Both, acupuncture (baseline to six-weeks change scores: mean: −2(standard deviation: 2.5 points), three months: −2.4(2.4), six-months −2.7(3.6)) and the combination of acupuncture and medical training therapy (−2.7(4.9), −2.2(4.0), −2.2(4.2)) (each within-group p < .05) significantly reduced depressiveness-scores (PHQ-9) to a greater extent than medical training therapy (−0.3(2.0), −0.5(1.6), −0.9(2.6)) or usual care alone (−0.8(2.9), 0.1(2.8), 0.2(3.6)). We found similar results with anxiety scores and the physical sum scores of the SF-12. No severe adverse events occurred.
Conclusions
Acupuncture and the combination of acupuncture and medical training therapy elicit positive effects on depression, anxiety, quality of life, and symptom intensity in patients with episodic and chronic tension-type headache. Acupuncture appears to play a central role in mediating the therapeutic effects, underscoring the clinical relevance of this treatment. An additive benefit of the combination of both therapies does not appear to be relevant.
Introduction
Tension-type headache (TTH) is the most common neurological disorder and ranked as the second most common cause of chronic illness and injury (1–4). According to the International Classification of Headache Disorders, TTH is classified as infrequent episodic TTH (ETTH, <12 days/year), frequent ETTH (≥12 and <180 days/year), and chronic TTH (CTTH, ≥180 days/year) (4).
Approximately 60% of patients with TTH report limitations in their social activities and ability to work (5). A study of young Italian patients with primary headache found quality of life (QoL) scores to be lower compared with those of unimpaired controls (6). Patients with CTTH especially had significantly lower QoL scores which were comparable with the levels found in patients suffering from migraines in the same study (6). CTTH is further associated with effects on the immediate social environment (7).
Etiologically, TTH is attributed to myofascial and, to a lesser extent, vascular factors leading to nociplastic pain via peripheral and central sensitization mechanisms depending on headache frequency (8). Accordingly, frequent ETTH and CTTH are associated with an increased risk for such dysfunctional nociplastic changes (8).
In addition, TTH is often associated with anxiety and depression (8). Holroyd et al. (9) found that patients with CTTH were three to 15 times more likely than matched controls to receive a diagnosis of anxiety or mood disorders. They also displayed impaired sleep, energy levels, and emotional well-being (9). Furthermore, unfavorable coping strategies such as catastrophizing and avoidance behavior occur more frequently compared with healthy controls, especially in CTTH (10,11).
Thus, it is not surprising that psychotherapeutic approaches and antidepressant medication such as amitriptyline, mirtazapine, and venlafaxine are recommended for patients with high-frequency ETTH or CTTH (8). In this regard, the selection of antidepressants is also primarily based on their ability to have an anti-hyperalgesic effect (12). In previous studies, such drugs have only been investigated over a maximum period of six months and side-effects (e.g., weight gain) may lead to the premature termination of such therapy (8). For this reason, non-pharmacological treatment approaches, such as physical therapy or acupuncture (AP), as individual or as combination therapies provide important alternatives (8). Meta-analyses have shown that both methods can substantially improve disease burden (11,13). In combination with medical training therapy (MTT) or as monotherapy, acupuncture significantly reduced the pain intensity in patients with ETTH and CTTH (14). These findings underline the relevance of conservative and minimally invasive treatments to reduce pain and pain-associated symptoms in TTH. Until now the effects (and comparative effects) of acupuncture and medical training therapy on QoL, anxiety, and depression have been insufficiently investigated. In this study, we compared the effects of acupuncture and medical training therapy in combination or individually with usual care on the quality of life, depression, and anxiety in patients with frequent ETTH or CTTH.
Methods
Design and ethics
This four-arm, prospective, randomized, clinical, unblinded trial was approved by the Ethics Committee of the Hannover Medical School (No.7751_BO_S_2018). The main objective as well as further details on the methods were presented in the trial registration (DRKS00016723) and study protocol (15). As is the general consensus in headache studies, the main outcome parameters were pain intensity, frequency of headaches, and use of analgesics (14). For this purpose, the corresponding sample size calculations were performed based on pain (interaction effect size f = 0.15, α = 0.05, beta = 80% for five measurement points and four study groups) and revealed a target sample of 20 patients per group (14,15). Secondary outcome parameters were QoL measured through the Short Form −12 questionnaire (SF-12), depression and anxiety measured through the Patient Health Questionnaire-9 (PHQ-9), and Generalized Anxiety Disorder-7 questionnaire (GAD-7) respectively. These secondary endpoints have been further investigated through explorative association analyses with some of the main outcome parameters (14).
Participants, inclusion and exclusion criteria
A total of 212 patients were screened. Recruitment was undertaken in pain clinics and practices, a primary care center, and through regional media. Subsequently, the diagnosis (according to the criteria of the International Headache Society, 3rd edition [ICHD-3]) was verified, and comprehensive information about the content, possible risks, and side effects of the study were provided. Participants aged 18 to 65 years, with >1 year of frequent ETTH (headache on 1–14 days/month) or CTTH (headache on >14 days/month) were included. Prior to enrollment, the diagnosis of frequent ETTH or CTTH was confirmed by pain specialists with advanced training in the treatment of headache disorders. All participants were required to continue and document their current therapy throughout the study period, that being abortive as needed (e.g. ibuprofen) and/or prophylactic drugs (e.g. amitriptyline) and non-pharmacological treatments (e.g. relaxation techniques). Exclusion criteria were infrequent ETTH (headache < 1 day/month), insufficient German language skills, treatment of TTH by AP or MTT within the past six months, severe somatic or mental illness, substance abuse, the use of headache medication on more than 10 days/month, >1 migraine/year, pregnant or lactating women, first occurrence of headache after the age of 50 years, or any other medical causes of headache. Further exclusion criteria were any changes in abortive medications, preventive medications, or non-pharmacological approaches from three months before until the end of the study and through the observation period.
Experimental design
A one-month pre-intervention phase (T0) was followed by an intervention phase (T1: baseline/start; T2: end) of 1.5 months (six weeks). Two follow-up appointments were conducted three (T3) and six (T4) months after the start of the intervention (Figure 1). The study and the data collection took place in the Department for Rehabilitation Medicine in Hannover Medical School.

Flowchart of the study.
Randomization
Randomization lists with different permutation block sizes were generated before study initiation. Blinded allocation to one of the four treatment arms was done by randomly drawing one of the opaque sealed randomization envelopes after enrollment in the study.
Interventions
During the six-week intervention period, the 12 treatment sessions were carried out in descending treatment frequency (3 to 2 to 1x/week). The participants of the usual care group (UC) had no additional appointments or interventions/treatments to compensate for the 12 treatment sessions in the intervention groups. A comprehensive medical history was obtained and a physical examination conducted. These participants were in contact with the study physicians and the study nurse at all five examination time points. At the end of the observation period, usual care participants could receive either AP or MTT at no additional cost.
AP (as monotherapy or in combination) was conducted according to the principles of traditional Chinese medicine (TCM) and current scientific literature. The semi-standardized therapy design included 10 to 16 AP points to address aspects of individual TCM diagnosis as well as standardization for treatments with similar symptomatology. In addition to the seven standardized AP points, three to five individual points (Table 1) and one to four local maximal pain points were selected after pain localization diagnosis (meridian localization). Acupuncture needles remained in situ for 30 minutes; directly after insertion and before removal manual stimulation was performed to induce a ‘deqi’ sensation. AP was performed with sterile disposable AP needles (25–40 mm × 0.25–0.3 mm; Suzhou-Tianxie) by an acupuncturist with more than five years of clinical experience. The content of the MTT (as monotherapy or in combination) was composed of strength, endurance, flexibility, and coordination training. This active equipment-based form of physical therapy took place in the training hall of the Department of Rehabilitation Medicine in small groups of four participants, each under the guidance of a qualified physical therapist. The types, dose, frequency, and load of the exercises were individualized. For that purpose, before the start of the intervention phase, a physiotherapeutic anamnesis and testing of the cardiovascular system, muscular strength, endurance, as well as posture and flexibility took place. From these results an individualized and intensity-adjusted treatment plan was created (Table 1). In addition, all participants in the MTT and combination group received a 15-minute self-tailored program to be actively performed three times per week. Participants in the combination group first received MTT and then AP treatment followed by a short 5- to 10-minute break. Both interventions were analogous to those described above and were equal to the sum of the therapy duration of MTT (60 min), rest (5–10 min), and AP (40 min). All interventions were carried out in addition to the pre-established usual care with regards to abortive medications, preventive medications, and mental techniques. Established usual care remained unaltered from three months before commencement until the end of the study and through the observation period.
Detailed description of the interventions (medical training therapy and acupuncture).

*Traditional Chinese Medicine unit of measurement for locating acupuncture points.
Outcomes
All assessments were collected in the form of self-reported questionnaires at the five measurement time points (T0–4) these covered the survey period of the preceding 4 weeks for each measurement point. The validated German versions of the Patient Health Questionnaire-9 (PHQ-9) (16) and the Generalized Anxiety Disorder-7 (GAD-7) (17) were used as modules of the Patient Health Questionnaire-9 (PHQ-9) (18) for continuous assessment of depression and anxiety symptoms. The PHQ-9 assesses depressive symptoms according to the criteria of the Diagnostic and Statistical Manual for Psychiatric Diseases using nine Likert-scaled items for all diagnostic criteria of major depression. The sum score ranges from 0 to 27 and allows a continuous assessment of the progression in order to show the effects of therapy. In addition, an interpretation of this sum score allows a grading of the illness severity (Category 0: 0–4, no depressiveness; Category 1: 5–9, mild depressiveness; Category 2: 10–14, moderate depressiveness; Category 3: 15–19, moderately severe depressiveness; Category 4: 20–27, severe depressiveness) (19). The GAD-7 consists of seven criteria through which a sum-score between 0 and 21 is calculated. From this score the categorical interpretation of the severity of anxiety symptomatology is possible (Category 0: 0–4, no to minimal anxiety symptomatology; Category 1: 5–9, mild anxiety symptomatology; Category 2: 10–14, moderate anxiety symptomatology; Category 3: 15–21, severe anxiety symptomatology) (20). The SF-12 is a cross-disease self-report questionnaire with 12 items to assess health-related physical and psychological QoL. Adverse events and side-effects were immediately documented and classified by one of the study doctors.
Statistical Analyses
Baseline data were descriptively displayed using means and standard deviations (interval scaled data) and as percentage values (ordinal and nominal scaled data). The following main analyses were performed for change scores (changes from T0) for each time point. Associated data were displayed as mean and 95% confidence intervals. Repeated measures mixed models (multilevel analysis) were calculated for the main effects (group and time) and for interaction effects (group * time; group * time * baseline-value; time * baseline-value) including the corresponding group * time *baseline-value detail comparison. For each outcome, a single omnibus model was calculated. Repeated measures (time) were calculated as random intercept and slope regressors, group, and co-variates as fixed effects. All mixed models were performed following checking for potential violations of the underlying assumptions for linear mixed models (heteroscedasticity, non-linearity, normal distribution of the residuals).
Ordinal scaled outcomes were displayed as absolute frequencies using stacking diagrams (group*time). Pearson Chi2-tests (where the underlying assumptions were fulfilled, otherwise Fisher’s exact tests) were calculated for the main effects (group and time effect) and in case of significance, followed by post-hoc comparisons. All analyses were performed using SPSS (Version 24, IBM SPSS, USA). All hypotheses were tested two-tailed. For significance testing, an alpha-error of 5% was considered a valid cut-off and all p-values below are consequently interpreted as significant.
Results
The course of the study is shown in the flowchart (Figure 1). Sixteen of the 96 participants quit early or withdrew consent during the course of the study. No severe adverse events occurred (14). The socio-demographic and baseline characteristics of the study population are shown in Table 2. More than two-thirds of the participants were female and ETTH was observed more frequently (70%) than CTTH (30%). The majority of patients displayed pericranial sensitivity (82%). In all treatment groups, data were homogeneously distributed with the exception of anxiety scores (GAD-7) and an absence of patients with a diagnosis of CTTH with pericranial sensitivity in the MTT group.
Socio-demographic, disease-related, and baseline characteristics of the sample.

All values are separated for group allocation and, likewise, displayed for the total sample. Mean and standard deviations (SD) are used to describe interval and pseudo-interval values, whereas ordinal and nominal values are displayed as numbers/frequencies.
AP, acupuncture group; GAD-7, Generalized Anxiety Disorder 7; ICHD, international classification of headache disorders; MTT, medical training group; NA = not applicable (too low frequencies); PHQ-9, Patient Health Questionnaire-9; SF-12, Short Form 12; TTH, tension-type headache; UC, usual care group; VRS, visual rating scale. * = Data already published by Schiller et al. (2021) (14).
Effects on depression, anxiety, and health-related QoL sum scores
The scores for all linear mixed models with repeated measures are shown in Table 3. There is a strong time effect for all outcomes when baseline values are partialized. Post-hoc significances (significant changes from baseline for each group), marked with asterisks, are shown in Figures 2 and 3. Arithmetic means and 95% confidence intervals are used to show possible time significant differences between groups (21–23).
Linear mixed models outcomes for the interval-scaled outcomes.

F- and p-values for the main effects (time and group) as well as the values for the interaction effects (time * group and time * group * co-variates) are displayed.
GAD-7, Generalized Anxiety Disorder 7; PHQ-9, Patient Health Questionnaire-9; SF-12, Short Form 12.

Mean and 95% confidence intervals of the change scores (absolute differences to the baseline assessment) of depressive symptoms (upper part, PHQ-9, Patient Health Questionnaire-9) and anxiety symptoms (lower part, GAD-7, Generalized Anxiety Disorder 7). Values below zero display a decrease in the symptom severity.

Mean and 95% confidence intervals of the change scores (absolute differences to the baseline assessment) of the health-related quality of life (SF-12, Short Form 12) sum scores. The upper part displays the physical and the lower part the psychological sum score.
Baseline (T0) depressiveness scores ranged from 0–23 in study participants (mean; +/−standard deviation) (6.6; +/− 4.4). A significant reduction in the PHQ-9 sum score from T0 was only observed in the AP (27–37%) and combination group (20 to 26%) at each subsequent time point (T2, T3, T4). The baseline anxiety score ranged from 0-20 in study participants (5.2; +/−4.1). A significant reduction in the GAD-7 sum score from T0 was only observed in the AP (25–36%) group at time points T2, T3, and T4 and the combination group (11 to 23%) at time points T3 and T4 (Figure 2).
The changes in health-related QoL (SF-12) scores are shown in Figure 3. Scores at baseline ranged from 25.1 to 55.9 (physical sum score) and from 22.0 to 60.9 points (psychological sum score). A group effect was found in both health-related QoL sum scores. The interaction effect time*group occurred only when baseline scores were considered as co-variates. Only the AP and combination groups showed a stable significant improvement in scores as a function of time for the physical sum score. The average relative change in physical sum scores reached up to 30% after AP and 20% after combination therapy at the six-month follow-up (T4). Significant changes in mental sum scores could only be observed in the MTT group. This can be explained by the higher number of treatment dropouts and a resulting higher homogeneity of the results compared to the other intervention groups.
Effects on depression, anxiety, and health-related QoL levels
The number of participants with different severity levels for depression and anxiety disorder (categorized by group and by time of measurement) is shown categorically by group and by time of measurement in Figure 4. Main effects (time and group) as well as possible post hoc comparisons have been calculated for each ordinal scaled outcome. Descriptively, the severity of depressiveness showed a positive distributional change over time, which failed to reach statistical significance (Chi2 = 14.5, p = 0.6).
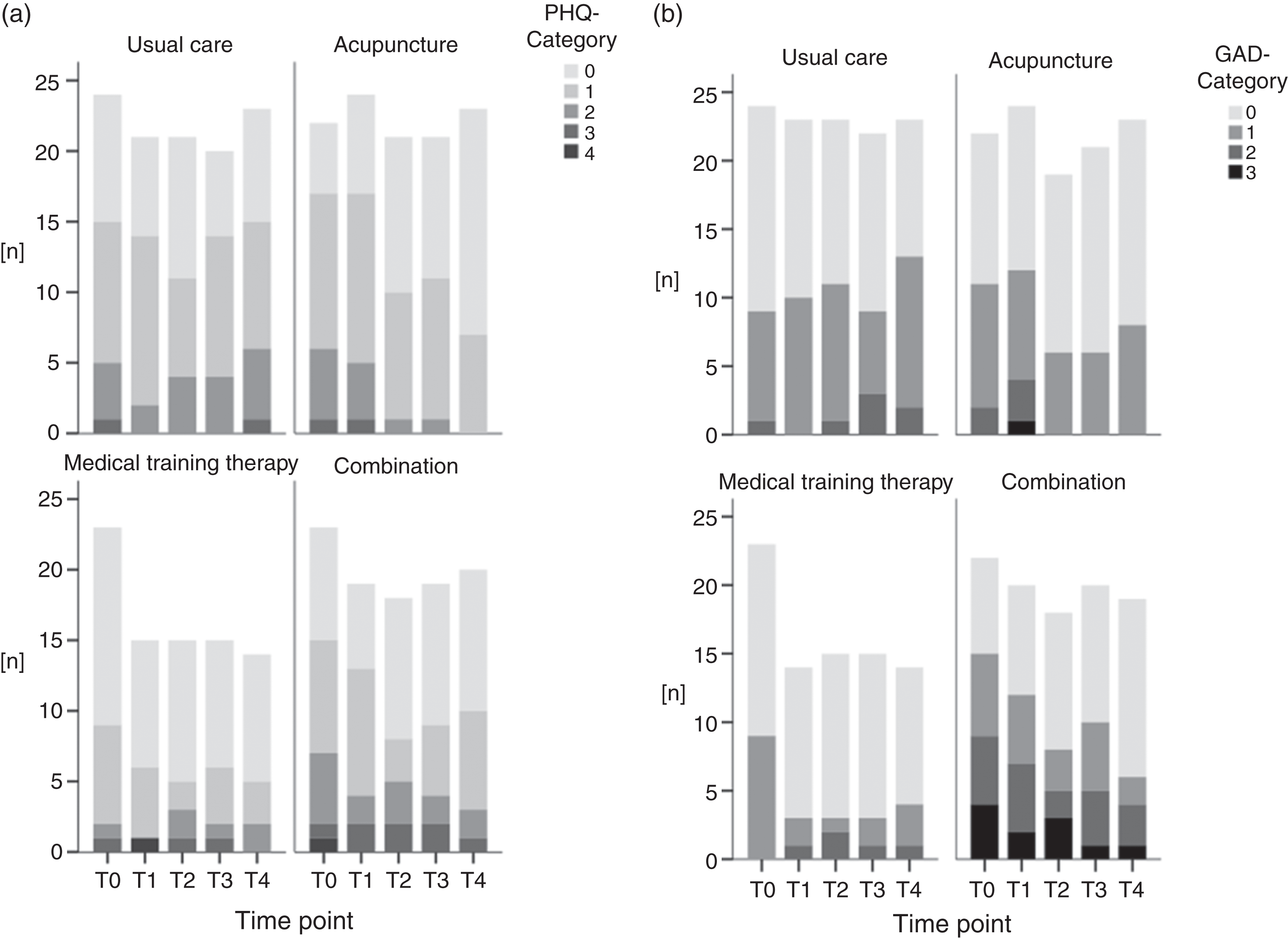
Absolute frequencies for depressive (a) and anxiety (b) symptoms, separated for each time-point and group. PHQ-9 (Patient Health Questionnaire-9) Category 0: 0−4, no depressiveness; Category 1: 5−9, mild depressiveness; Category 2: 10−14, moderate depressiveness; Category 3: 15−19, moderately severe depressiveness; Category 4: 20−27, severe depressiveness. GAD-7 (Generalized Anxiety Disorder 7) Category 0: 0−4, no to minimal anxiety symptomatology; Category 1: 5−9, mild anxiety symptomatology; Category 2: 10−14, moderate anxiety symptomatology; Category 3: 15−21, severe anxiety symptomatology).
Significant group differences with regard to depression levels were found in favor of the AP and combination groups (Chi2 = 27.6, p = 0.01). The proportion of participants with no (Category 0) and low depressiveness (Category 1) increased in these groups, whereas the proportions with medium (Category 2), moderately severe (Category 3), and severe depressiveness (Category 4) decreased over time (see Figure 4A). A similar result has been shown regarding the severity of anxiety symptoms categorized by the GAD-7 (see Figure 4B). Descriptively, the severity of anxiety symptoms showed a positive change in distribution over time. Statistically, no effect could be observed (Chi2 = 7.4, p = 0.8), but significant between-group differences occurred (Chi2 = 58.7, p = 0.001).
Explorative association analyses
The changes in depressiveness, anxiety, and development of health-related QoL (ppsychological = 0.003; pphysical = 0.037) showed an association with a reduction in the frequency of headache days per month between baseline and first follow-up (Table 4). Change in headache frequency was associated with anxiety at baseline in the AP group when the intervention groups were considered (p = 0.04). In the combination group, changes in TTH frequency were associated with baseline anxiety and change scores at T3 (p = 0.02). Furthermore, this group showed an association with baseline health-related QoL psychological sum score (p = 0.02).
Explorative correlation analyses between baseline- and change-scores and interventional effects.

Significant associations are marked in bold letters. GAD-7, Generalized Anxiety Disorder 7; PHQ-9, Patient Health Questionnaire-9; SF-12, Short Form 12. * = statistic significant p < 0,05.
Discussion
We compared the effects of three non-pharmacological treatment interventions on the self-reported psychological comorbidities of anxiety and depression as well as QoL in patients with frequent ETTH and CTTH. To the best of our knowledge, this is the first study to examine two different non-pharmacological treatments individually and in combination with standard therapy. We demonstrated that AP, in particular as monotherapy, but also in combination with MTT, had a substantially positive and lasting effect on the symptom severity of depression and anxiety. These improvements differed significantly from the results of the usual care group. In the categorical evaluation, these findings were supported by an increase in the number of participants whose symptoms were categorized as “none” to “low” in both anxiety and depressiveness, as results of the interventions. The change in scores for depressiveness, anxiety, and health-related QoL was associated with the changes in headache frequency and thus could explain an influence on the frequency of headache days per month. This is in keeping with the current scientific body of evidence that a reduction in headache days is also associated with an improvement in QoL and amelioration of mental comorbidities (24).
The present study results emphasize the importance of AP in terms of mood and QoL in TTH settings. The combination of both, AP and MTT, resulted in an additive effect on pain intensity and frequency (14). As outlined above, usually there is a strong correlation between the reduction of headache days and improvement in QoL. However, AP seems to address mainly headache intensity and QoL together with mental comorbidities (25–28). These pleiotropic effects of acupuncture can be explained by its profound neuro-immunological mechanisms, e.g. via the inflammatory reflex, or in the context of a successful doctor-patient relationship (29). This holistic, biomedical information therapy (29) seems to have an added value compared to MTT. This finding is supported by a study that compared AP and stretching with AP and stretching + physiotherapy in a small group of 44 patients with episodic TTH (30). After 10 treatments within four weeks, both groups showed significant improvements in headache frequency, depression, anxiety, pain catastrophizing, and QoL-measurements. In the absence of group differences, physiotherapy showed no additional benefit (30).
In a three-group comparison of 90 patients with CTTH, the influence of AP, relaxation training, or physical training on subjective well-being was investigated (31). The 24-item Minor Symptom Evaluation Profile (MSEP) questionnaire was used. While this instrument is not suitable to measure depression and anxiety, it can be used to measure relevant health-related QOL dimensions (31). After 10 to 12 treatments within 10 to 12 weeks, significant improvements were seen in all study arms over a period of up to six months compared to baseline. However, at the three-month follow-up, significantly more participants in the physical training group showed improved MSEP-levels compared to the AP group. At the six-month follow-up, an analysis of sub-items of the MSEP showed a significant advantage of the relaxation treatment compared to the AP treatment (31). Nonetheless, with a statistical power of 64%, these findings should be treated with caution. Furthermore, the interventions were performed by three to five physiotherapists in three different clinics. As there is a known strong influence of the practitioner and the practitioner-patient relationship on the results of acupuncture treatments (32), a large degree of confounding can be assumed here.
Meta-analyses have long suffered from methodological differences in the field of acupuncture studies. Consequentially, this often results in non-significant results leading to controversial discussion of the utility of AP in the treatment of TTH (33–35). However, one recent systematic review comes to a more optimistic conclusion in relation to the effectiveness of AP in TTH (36). In many cases, studies fail to create a suitable control/comparison condition (8). This is due to the fact that AP is not an inert form of therapy and is accompanied by ubiquitous non-specific therapeutic effects. These placebo effects are present in every active form of therapy and produce a variety of therapeutic effects depending on the affection, sympathy, and interest displayed by the practitioner, as well as the individual expectations of the patient (37,38). Therefore, it is necessary to use comparative intervention groups with likewise non-inert forms of therapy to produce similarly strong non-specific therapeutic effects (33,39). The elaborately planned and technically complex so-called sham or placebo acupunctures (40) are difficult or impossible to compare due to these contextual influencing variables (39). The major strength of this study was that, unlike many other study designs, three different similarly non-inert complex interventions were compared. In addition, these three groups were compared with standard therapy in the form of patients on a waiting list. Since all groups remained unchanged with regards to their established treatment plans, systematic biases were kept low. In addition, no significant differences in the use of abortive or preventive medication between the study groups were observed. Only four patients (UC: n = 1; AP: n = 2; MTT: n = 1; AP+MTT: n = 0) of the whole study population used an antidepressant as a preventive medication. Only with such a design can the “true” placebo response be observed. Accordingly, in large acupuncture trials, a waiting list control was usually included (41).
In summary, our study supports the implementation of AP as a therapeutic method for frequent ETTH and CTTH as a meaningful add-on treatment option with high patient acceptance and low side effect rates. Furthermore, the authors estimate the contribution of AP to the treatment effect in a multidimensional treatment model to be substantial.
Limitations
The time burden of the combination group may have led to temporal-organizational stress in some participants, which may also have negatively affected the above-mentioned parameters of well-being. In future studies, attention should be paid to appropriately good and patient-oriented time management. Moreover, a review of the results with a larger number of participants seems useful. The high number of dropouts in the MTT group should be considered in future planning of comparable studies. Monitoring of adherence to the self-directed exercise program should be planned to obtain information on the compliance of the participants. Particularly when studying parameters of individual well-being, seasonal influences on mood should be accounted for in future planning, although all study arms were affected equally in our study. Patient recruitment by regional media could have caused a selection bias by having mainly those patients apply to participate who had a particular interest in the interventions offered. However, in the information sheet provided to the patients beforehand, treatment methods were described as equally effective and the participants’ expectations did not differ between the three intervention groups (14). Additionally, results from the UC group could have been influenced by the fact that participants knew that they were not going to receive any of the study interventions leading to an overestimation of intervention effects. This is a general problem of studies using a design of usual care/waiting list although not all research suggests a systematic bias in the estimation of treatment effects (42). In our study, it could be assumed that the close follow-ups and the offer of MTT or AP treatment free of charge after the last follow helped to mitigate some bias triggered by waiting time.
Conclusion
AP as monotherapy and the combination of AP and MTT as add-on therapy to usual care elicited positive effects on depressiveness, anxiety, and QoL in patients with frequent ETTH and CTTH. The proportion of study participants with high-level symptom severity was reduced by these procedures. A possible relationship between the change in these parameters and the frequency of days with headache per month could be presented in an exploratory analysis. In summary, it can be postulated that in terms of depressiveness, anxiety, and health-related QoL, AP seems to play a central role in mediating the effects of therapy. This emphasizes the clinical relevance of this therapeutic procedure in the treatment of patients with TTH.
Key findings
Acupuncture alone, as well as in combination with Medical Training Therapy had positive and sustained effects on depression and anxiety. Acupuncture seems to play a central role in mediating the therapeutic effects in multidimensional treatment approaches for frequent episodic and chronic tension-type headaches with regard to depressiveness, anxiety, and health-related quality of life.
Footnotes
Acknowledgments
We thank the China Academy of Chinese Medical Sciences (CACMS) for the successful collaboration and support in establishing the Chinese-German research outpatient program at the Department of Rehabilitation Medicine of the MHH. Furthermore, we thank V Bono-Contioso and A Ostermann for the personal support of the study participants and organization of the appointments. We thank J Briest and X Liu for their assistance in performing the statistical calculations. We thank K Hoepner and M Lemke for the excellent conduction of physiotherapy. We would like to thank T Weiberlenn and L Jiang for their support in TCM questions. All authors met the ICMJE criteria for authorship. No fees or payments were made for the authorship. Finally, we would like to thank all study participants for their faithful participation in our study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was performed as part of the development of a research clinic for integrative Chinese medicine. The project was sponsored by Tasly Healthcare Deutschland GmbH (Bahnhofstr. 8, 30159 Hannover). Tasly has and will not influence the unbiased and scientific character of this publication.