
Abstract
A study with needle acupuncture was performed in tension-type headache employing a new placebo acupuncture method. Sixty-nine patients (mean age 48.1 years,
Introduction
Over the last two decades, several studies have investigated the efficacy of acupuncture in relieving headache (1–3). Some of them suggested that acupuncture may be useful (1), others showed no superiority to sham acupuncture (2) or alternative treatment regime (3). Because headache is known to be particularly responsive to placebo treatment (4), the choice of a suitable placebo for acupuncture studies is difficult. For clinical acupuncture studies, trials should be single blind, and sham acupuncture or mock transcutaneous electric nerve stimulation (TENS) are the placebo methods required (5). From a methodological point of view, acupuncture with placebo needles seems to be more appropriate because it has the same credibility as real acupuncture (6) without a strong stimulus as in sham acupuncture. In the study by Loh et al. (1), beneficial response to acupuncture treatment for migraine and tension-type headache (TTH) was more likely when the patient had local tender muscular points. In the study by Carlsson et al. (2), tenderness was reduced in some muscles after acupuncture, suggesting that nociception from pericranial muscles may play an important role in the pathophysiology of TTH.
The goal of the present study is to examine whether treatment with acupuncture on local and distal points is able to change or improve VAS or other outcome parameters (CGI, headache frequency, depression scores, analgesic consumption).
Patients and methods
Patients
The required sample size to achieve a 90% power for the expected differences between mean values was calculated as 34 per group.
We included 69 subjects (mean age 48.1 years,
Sample characteristics (baseline values). Standard deviation is indicated in parenthesis. If differences are significant, difference Z (Wilcoxon-test) and P-value are indicated

FQCI=Freiburg Questionnaire of Coping with Illness; D-S = von Zerssen Depression Scale.
Examination
The patients were carefully examined prior to as well as immediately, 6 weeks and 5 months after treatment. Patients were asked to keep a home diary throughout the study (starting 4 weeks prior to the study), recording:
daily consumption of analgesics (usually tablets);
pain intensity (visual analogue scale: range 0–10; 0 = no pain, 10=strongest pain);
site and duration of headache attacks;
and headache frequency (number of days per month with headache).
Furthermore, patients were required to give a rating on the visual analogue scale (VAS) and their impression of improvement on a clinical global impressions (CGI) scale (8) when followed-up. In order to evaluate quality of life parameters and coping strategies, subjects were asked to complete a Nottingham Health Profile (9), an Everyday-Life-Questionnaire (10), a Freiburg Questionnaire of Coping with Illness (11) and a von Zerssen Depression Scale (12).
Treatment
Placebo needle
The tip of the needle is blunt in order to cause a pricking sensation without actually puncturing the skin (6). The needle was inserted through a cube-shaped elastic foam to obscure the patients' vision on the insertion point.
Verum needle
Seirin B-type needles no. 8 (0.3 × 0.3 mm) and no. 3 (0.2 × 0.15 mm) were used for verum acupuncture.
Protocols
The patients underwent two treatments per week for a total of 10 treatments. Verum and placebo needles were inserted at acupoints GB20 (medial to the mastoid process), LI4 (first dorsal interosseus muscle of the upper limbs) and LR3 (first dorsal interosseus muscle of the lower limbs), and depending on the symptoms at acupoints GB8 (above the tip of the ear), GB14 (above the middle of the eye-brow), GB21 (over the middle of upper border of the trapezius), GB41 (lateral to the tendon of the extensor digiti longus V), UB2 (medial end of the eye-brow), UB10 (insertion of the trapezius at the external protuberantia occipitalis), UB60 (middle between the external malleolus and the tendon of the gastrocnemius), LU7 (between the tendon of the extensor pollicis and the radius), TW5 (between the radius and ulna proximal to the wrist), ST8 (in the angle of forehead and temple), ST36 (lateral to the tibia at the level of the tuberositas tibiae), ST44 (between the second and third toe in the fold), DU20 (middle of the skullpan) and Extra1 (middle between the eye-brows). A maximum of 15 needles were inserted but treatment was usually carried out with not more than 6–10 needles. The needles were left in place for 30 min after insertion. The exact localization of those acupoints is described in Cheng (13).
Both the investigator performing follow-up examinations and statistical procedures and the patients were blind to treatment condition (placebo vs. verum); blinding the acupuncture practitioner was impossible due to methodological reasons. According to the results of a credibility questionnaire none of the patients was able to distinguish between verum and placebo acupuncture.
Statistics
Because of the high variance within groups non-parametric methods were employed. Differences between groups were estimated using the Wilcoxon-test, differences between examinations were estimated using the Mann–Whitney-U-test. In addition, we computed decision tree analyses (CART=classification and regression tree). Differences were considered significant with P < 0.05 and 10-fold-cross-validation, respectively.
Results
Prior to treatment, placebo and verum groups did not differ significantly in terms of VAS, headache frequency, sociodemographic data and quality of life parameters, except for more minimizing and wishful thinking (FQCI, subscale 5) in the placebo group (Wilcoxon-test: Z =− 2.125, P = 0.034) (Table 1).
For the entire sample, VAS scores at consultations and headache frequencies decreased significantly (t-test, P = 0.000) at each follow-up without an appreciable difference between the placebo and verum groups (Table 2): VAS of the placebo group was 6.3 (
Measures of frequency of headache days per month, VAS at consultation, mean VAS (over a period of 4 weeks, respectively), consumption of analgesics per month, D-S, FQCI 1 and 5, CGI, NHP, ELQ, LS at follow-ups. Mean and standard deviations (in parenthesis) are indicated. If differences are significant, difference Z (Wilcoxon-test) and P-value are indicated. Follow-up 1, last day of treatment; follow-up 2, 6 weeks after treatment; follow-up 3, 5 months after treatment
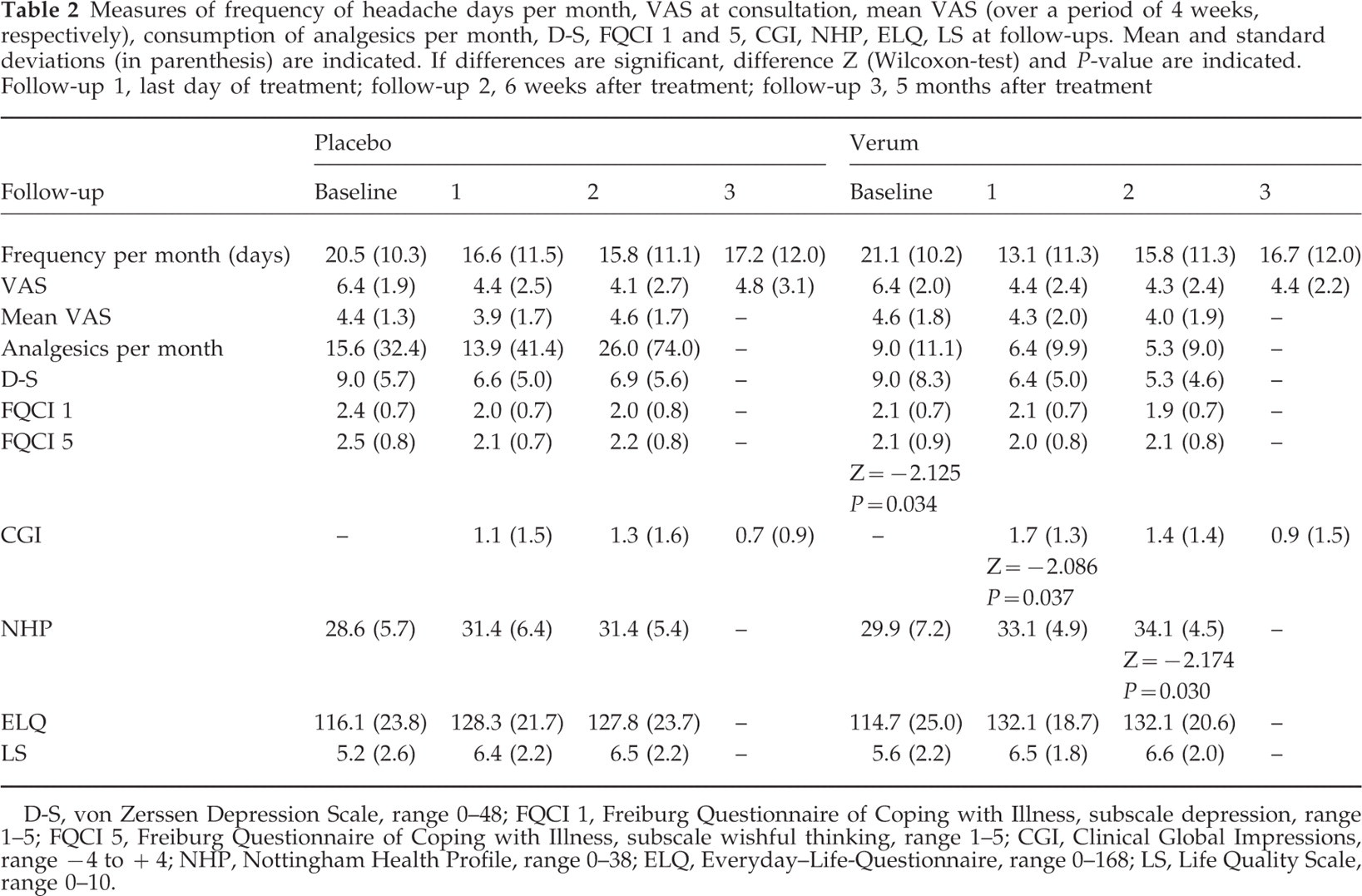
D-S, von Zerssen Depression Scale, range 0–48; FQCI 1, Freiburg Questionnaire of Coping with Illness, subscale depression, range 1–5; FQCI 5, Freiburg Questionnaire of Coping with Illness, subscale wishful thinking, range 1–5; CGI, Clinical Global Impressions, range −4 to +4; NHP, Nottingham Health Profile, range 0–38; ELQ, Everyday–Life-Questionnaire, range 0–168; LS, Life Quality Scale, range 0–10.
In contrast, mean VAS values over a period of 4 weeks did not change significantly: mean VAS of the placebo group was 4.4 (
In both groups there was a non-significant improvement in the values of Everyday-Life-Questionnaire, Life-Quality-Scale (0–10) and von Zerssen Depression Scale of about 5–10% at any follow-up (Table 2). Nottingham Health Profile values increased by about 7.3% at follow-up 1 and 2 in the placebo group; in the verum group there was a statistically significant increase of about 8.5% at follow-up 1 and 11.1% at follow-up 2 (Wilcoxon-test: Z =− 2.174, P = 0.030) (Table 2).
In the placebo group CGI improved about 30% at follow-up 1 and 2, at follow-up 3 there was only an 18% improvement. In the verum group CGI improved markedly and significantly by 43.5% at follow-up 1(Wilcoxon-test: Z =− 2.086, P = 0.037). At follow-up 2 and 3 there was only a non-significant improvement of about 36% and 23%, respectively (Table 2).
Furthermore, frequency of headache attacks (days per month) decreased by about 20% at each follow-up in the placebo group. In the verum group there was a more marked reduction (38%) at follow-up 1; at follow-up 2 and 3 the reduction of frequency was about 20%. None of the differences was statistically significant (Table 2).
In the verum group, the consumption of analgesics decreased by about 29% and 41% at follow-ups 1 and 2, respectively, as compared with an 11% decrease at follow-up 1 and a 66% increase at follow-up 2 in the placebo group. None of these differences was statistically significant (Table 2).
In the CART-analysis clinical global impressions (CGI) improvement correlated with primary headache frequency with 10-fold-cross-validation (limit values: 24.5 and 30.5 headache days per month) and religiousness scores (subscale 4, limit value: 3.1) of the FQCI (Fig. 1). Reduction of headache frequency correlated with primary headache frequency with 10-fold-cross-validation (limit values: 24.5 and 29.5 headache days per month) (Fig. 2). In CART-analysis a value of less than 19.5 in the von Zerssen Depression Score (D-S) resulted in a mean VAS value of 3.78 with 10-fold-cross-validation (Fig. 3).

Decision tree analysis (classification and regression trees=CART) with 10-fold cross-validation regarding headache frequency (days per month) at baseline (FREQ0) and clinical global impressions at follow-up 1 (CGI1) and follow-up 3 (CGI3) and subscale 4 (religiousness) of the Freiburg Questionnaire of Coping with Illness (FQCI 4).

Decision tree analysis (classification and regression trees=CART) with 10-fold cross-validation regarding headache frequency (days per month) at baseline (FREQ0) and headache frequency at follow-up 1 (FREQ1), follow-up 2 (FREQ2) and follow-up 3 (FREQ3).

Decision tree analysis (classification and regression trees=CART) with 10-fold cross-validation regarding von Zerssen depression scale at baseline (D-S0) and mean visual analogue scale at follow-up 1 (MVAS1: over a period of 4 weeks).
Discussion
In acupuncture treatment outcome is a composite of three factors: placebo effects, non-specific physiological responses to the piercing of the skin, and specific responses to stimulation of the particular acupuncture points chosen for treatment. To assess placebo effects, a procedure must be devised that is both non-invasive and credible to the patients (14). When the placebo treatment involves mock needling, it is virtually impossible to blind the acupuncturist. Blinding the patients is possible using the method of Streitberger and Kleinhenz (6) even when the patients are acupuncture-experienced. The credibility of the placebo was assessed and showed similar results (data not shown) as in the study of Streitberger and Kleinhenz (6).
With respect to VAS and headache frequency there was a significant decrease at each follow-up, but there was no difference between placebo and verum treatment. Mean VAS (over a period of 4 weeks) did not change significantly. This supports the findings of acupuncture studies in migraine (15): a reduction of headache frequency is more likely than an improvement of headache intensity.
Quality of life parameters (CGI, Nottingham Health Profile) improved significantly, but only moderately after verum treatment. No significant changes were observed with respect to other variables mentioned above.
In decision tree analyses CGI outcome depended significantly on primary headache frequency. Less than 24.5 days headache per month resulted in more than twice the CGI values, daily headache attacks resulted in a negative CGI value at follow-up 3. Furthermore, a high score for religiousness in subscale 4 of the FQCI revealed the highest CGI values at follow-up 3 (Fig. 1). Changes of headache frequency depended on primary headache frequency in decision tree analyses: more than 29.5 and 24.5 headache days per month, respectively, resulted in little change of headache frequency at follow-up 1, 2 and 3 (Fig. 2). High mean VAS scores at follow-up 1 correlated strongly with high values in D-S (Fig. 3).
Effectiveness of needle acupuncture in TTH is overall disappointing (2, 3). A reason for this finding could be that study populations were not divided adequately regarding headache frequency and depression. Tavola et al. (2) found that the presence of ‘Conversion V’ in the mean Minnesota Multiphasic Personality Inventory Manual (MMPI) profile predicted a low response to acupuncture treatment. Tolksdorf et al. (16) found a low effectiveness of needle acupuncture in patients with depression. In contrast, Creamer et al. (17) found no evidence for a link between psychosocial variables and response to acupuncture among patients with knee osteoarthritis; however, response was significantly related to duration of symptoms.
Holroyd et al. (18) investigated psychosocial correlates and impact of chronic TTH. They found that chronic TTH has a greater impact on individuals' lives than generally assumed and therefore suggested treating affective distress as well as pain. In addition, Holroyd et al. found a presence of headache on more than 25 days per month in two-thirds of patients with chronic TTH, whereas only 12% reported headache on less than 20 days per month. Siniatchkin et al. (19) identified frequency of headaches and depression as predictor variables for transformation of episodic into chronic TTH.
In conclusion, headache frequency and depression are stronger predicting factors of outcome than differences between placebo and verum in acupuncture studies on TTH. Even in the study sub-population with less than 24 days headache per month and with a score of less than 19 in the von Zerssen Depression Score (D-S) (n = 34) there are no significant differences between placebo and verum regarding outcome parameters. Furthermore, the definition of chronic TTH as assessed by the IHS criteria may need to be changed regarding headache frequency.
Footnotes
Acknowledgements
We thank Anja Freitag for her skilfull technical assistance.