
Abstract
Objective
To compare clinical features in youth with continuous headache from migraine, persistent post-traumatic headache, and new daily persistent headache to determine if they are similar, contrary to their distinction in the International Classification of Headache Disorders.
Methods
We pursued a single center age- and sex-matched observational study comparing the clinical characteristics of 150 youth (11 – 17 years old) with continuous headache from migraine, persistent post-traumatic headache, and new daily persistent headache. A diagnostic algorithm based on international classification of headache disorders criteria was used to identify those with migraine (headache features of migraine with gradual onset), and persistent post-traumatic headache and new daily persistent headache (based on the circumstances of headache onset regardless of headache features). Fifty participants each with migraine, persistent post-traumatic headache, and new daily persistent headache were matched by age and sex. Participant survey responses on headache characteristics were compared.
Results
Median usual headache severity was 6.0 [95%CI 6.0, 6.0] and was not different across diagnostic groups (H statistic = 1.2, p = 0.55). Headache exacerbation frequency, disability, associated symptoms, and most triggers were not significantly different across groups. The majority of persistent post-traumatic headache and new daily persistent headache had headache features consistent with a diagnose of migraine (72% and 62%, respectively).
Conclusion
Our findings suggest that most persistent post-traumatic headache and new daily persistent headache may represent abrupt onset of migraine.
Keywords
Introduction
Continuous headaches – in which there are not discrete headache-free periods – are considered to be more rare and medically refractory than intermittent headaches (1), but there is a paucity of research on this topic. The International Classification of Headache Disorders, 3rd edition (ICHD-3) diagnostic criteria (2) treats continuous headaches as distinct clinical entities based on whether episodic headaches increased in frequency and became continuous over time (migraine), started abruptly following a head injury (persistent post-traumatic headache; PPTH), or started abruptly without clear cause (new daily persistent headache; NDPH). NDPH is the only diagnosis that requires a continuous headache; this entity is less well-defined by the ICHD-3 in PPTH and migraine. The literature has primarily focused on assessing chronic migraine defined as at least 15 days per month with discrete pain free periods (3).
It has been hypothesized that migraine, NDPH, and PPTH have common biologic underpinnings. NDPH may be a form of status migrainosus (4,5) and PPTH may be migraine precipitated by trauma (6). This is supported by the findings that there are few clinical differences between migraine, PPTH, and NDPH. Individuals with NDPH largely present with features of migraine at rates similar to those with migraine (4,7). Migraine phenotype in PPTH is also high, ranging from 55 to 70% (8,9). Proper comparison of these conditions should focus on continuous headache to control for headache burden. One study that directly compared children and adolescents with continuous headache found no clinically significant differences in headache characteristics or headache-related disability between migraine and NDPH (1). Similar findings have been reported in adults (10). However, no pediatric studies matched for age and sex have directly compared migraine, NDPH, and PPTH while accounting for confounding variables.
We hypothesized that clinical features of youth with continuous headache would not differ whether they had a presentation consistent with migraine, PPTH, or NDPH. We expand upon the current literature by introducing the first age- and sex-matched comparison of these three conditions in youth with continuous headache, which supports describing PPTH and NDPH as circumstances in which migraine can be abruptly triggered, and has implications for treatment.
Methods
Patient survey data
This pre-registered single site cross-sectional study (11) conducted from patient questionnaires collected at the Children’s Hospital of Philadelphia general neurology and headache outpatient clinics comparing headache features in youth with continuous headache with migraine, PPTH, or NDPH. The Children’s Hospital of Philadelphia’s Institutional Review Board approved the extraction of the data from the electronic health record into a research registry, with a waiver of consent and assent to maximize generalizability. Survey data were collected and managed in REDCap (Research Electronic Data Capture) hosted by The Children’s Hospital of Philadelphia (12,13). Patient reported demographics and headache history were collected which included age of headache onset, duration and frequency of severe headaches, the presence of medication overuse headache, headache location, pain quality, headache triggers, and associated symptoms.
Participant selection
Questionnaires were used to categorize each participant based on an algorithm that searches through patient questionnaire responses to identify answers that are consistent with ICHD-3 diagnostic criteria (14). Responses that were consistent PPTH (headache started following head injury) or NDPH (headache started abruptly on a single day) were diagnosed as such, and responses that met headache features consistent with migraine that did not meet criteria for PPTH or NDPH were diagnosed as migraine. Given that diagnosis is based on patient-reported headache features and history, participant selection was masked to the clinician assigned international classification of disease (ICD) diagnosis.
We included surveys from respondents aged 6 to 17 years of any sex and race/ethnicity if the following criteria were met: (1) questionnaire completed between June 2017 and February 2022; (2) report of continuous headache for at least three months, but for no more than 12 months; (3) reported trying two preventive prescription medications or fewer, to control for treatment prior to the start of the questionnaire. Inclusion criteria 2 and 3 controlled for the refractory nature of headaches in the sample. After chart review of the initial case control sorting, additional inclusion/exclusion criteria were added: (4) patients who reported that PTH developed within seven days and transitioned from intermittent to continuous within eight weeks of concussion; this was done to capture participants who had an abrupt onset of continuous headache or transitioned to continuous in a short period of time following a head trauma and removing those who partially recovered from concussion and then developed continuous headache at a later date, and (5) only included those in the migraine group whose headaches took longer than four weeks to progress to eliminate those who had rapid progression of episodic to continuous headache.
Entries categorized as migraine, PPTH, and NDPH were used to match to the same sex, and age-matched to within 120 days. Males were matched first to maximize the number of males in the study given the high level of female predominance in continuous headache. Based on prior comparisons between migraine and NDPH, we calculated that 40 participants per group would be needed to detect non-equivalence of +/−1 on the numeric 0–10 pain scale with 80% power, and an alpha of 0.05 (1). We decided to collect 50 per group as we were comparing across multiple metrics.
To account for possible inaccuracies in patient questionnaire answers, a chart review of the 150 participants was conducted by a UCNS-certified headache specialist (CPG). Nighty-nine charts (66%) had no discrepancy between patient answers and clinician documentation. Of the remaining 34%, about half had some indication in the provider note that there were breaks in headache pain, and the other half called the ICHD-3 diagnosis based on patient responses into question. Frequency of patient survey/provider documentation discrepant charts were similar across the three diagnostic categories. Post-hoc comparison of consistent and discrepant charts did not find any differences in the distribution of results within migraine, PPTH, or NDPH groups, and outcomes did not change if only the consistent charts were compared.
Data analysis
All analyses were performed using custom written code in Matlab (Mathworks, Natick, MA), which is publicly available (15). Median responses were presented for age, headache severity, and PedMIDAS scores since all of these metrics did not have a normal distribution, with 95% confidence intervals determined by bootstrap analysis. Univariate statistical testing across the three diagnostic groups was achieved with cross tabulation using chi-squared analysis for categorical data, and Kruskal-Wallis testing for interval data. H-statistic was reported for Kruskal-Wallis testing for significance. An alpha of 0.05 used as the threshold for significance for headache severity, frequency of bad headache days, and PedMIDAS. Benjamini-Hochberg correction was reported to determine p-value significance for pain quality, associated headache symptoms, and headache triggers to adjust for multiple comparisons. Bonferroni correction was also reported for p-values that reached significance based on Benjamini-Hochberg criteria, which offered stricter criteria for significance given multiple comparisons. In the rare situation where there was missing data because the intake form was not fully filled out, it was noted in the results.
Results
The headache registry included 9363 intake headache questionnaires collected from general neurology and headache clinics between June 2017 and February 2022 (Figure 1). Of the 558 entries that broadly met inclusion criteria in the study, 91 met the above-listed strict inclusion and exclusion criteria for migraine (16%), 67 for PPTH (12%), 145 for NDPH (26%). One-hundred and fifty participants (50 per group) were age and sex matched across the three diagnoses. The sample was 92% female with a median age of 15.4 years [range 11.1, 17.7] and demonstrated effective biological sex and age matching (Table 1). Race and ethnicity demographics of the entire cohort are similar to the 2020 Census data of Pennsylvania demographics (16). Most participants had not tried any preventive medications (87%), and this did not differ between groups (
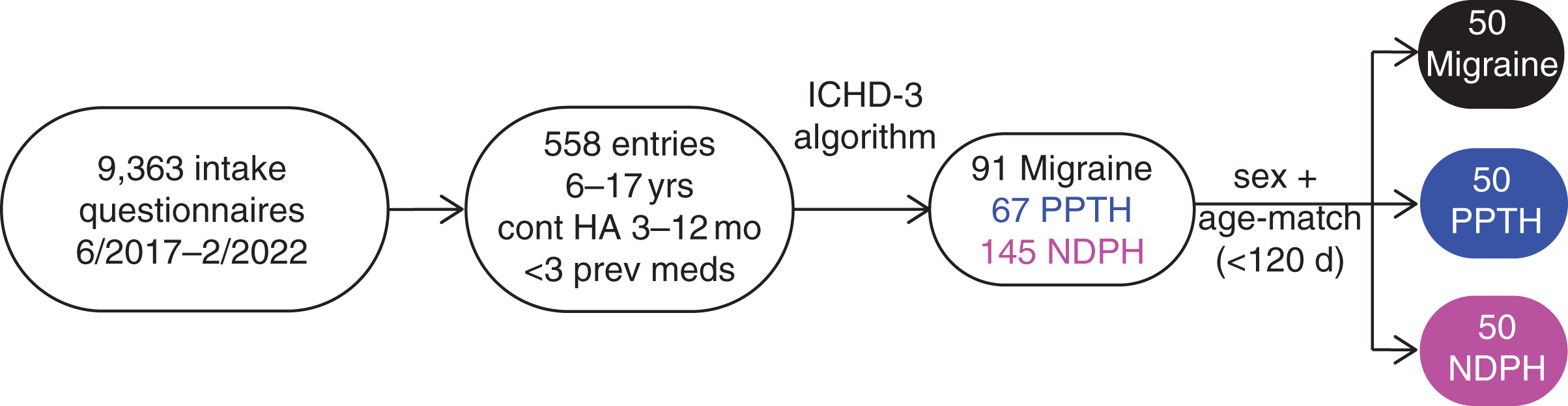
Flowchart demonstrating participant survey selection and matching process.
Demographics and headache history. Characteristics of individuals included in the observational study across the entire sample and separated by diagnosis.

Abbreviations: female (F), male (M), persistent post-traumatic headache (PPTH), new daily persistent headache (NDPH), medication overuse headache (MOH), headache (HA), Pennsylvania (PA).aMatched to within 120 days.
bMatched to biological sex.
cAI/AN is American Indian or Alaskan Native.
dUse of acute HA meds >3 days/week for >3 months.
Medication overuse headache (MOH) defined as use of acute medications (primarily non-steroidal anti-inflammatory drugs) an average of four times a week or greater for at least three months was uncommon in the cohort (7% of participants) and did not differ between groups (
Headache severity, frequency, and disability
Metrics related to headache burden including headache severity (on 0–10 numeric scale), frequency of headache exacerbations, and headache-related disability were compared (Figure 2). The median usual headache severity of the entire sample was 6.0 [95%CI 6.0, 6.0] indicating moderate headache severity (Figure 2a). The median headache severity did not significantly differ between migraine (median 6.0, [95% CI 6.0, 7.0]) PPTH (median 6.0, [95% CI 5.0, 6.0]), and NDPH (median 7.0, [95% CI 5.0, 7.5]; H = 1.2, p = 0.55). Of note, the NDPH group showed a more bimodal distribution than the other two groups with a smaller peak seen at a headache severity score of 4, and a larger peak seen at a headache severity score of 8. Most participants reported at least two to three bad headache days per week above baseline (Figure 2b). The frequency of bad headaches did not differ between diagnostic groups (

Headache burden of participants by headache diagnosis: migraine (black), persistent post traumatic headache (PPTH; blue), and new daily persistent headache (magenta). (1) Distribution of average headache pain on 0–10 scale, inverted triangles show median values with 95% confidence intervals. (b) Frequency of headache exacerbations. (c) Median pedMIDAS scores with 95% confidence intervals.
The median PedMIDAS score across the entire sample was 55.0 [95%CI 35.0, 65.5] indicating severe headache-related disability. The range of PedMIDAS scores was large, and there were no significant differences between groups for raw PedMIDAS score (H = 2.6, p = 0.28). Indeed, 47% of all participants reported a PedMIDAS score of more than 50, indicating severe disability base on the PedMIDAS disability grading system. Of note, interpretation of PedMIDAS data is somewhat limited because it was not reported in 16% of participants with PPTH, and 10% of participants with NDPH. Headache burden outcomes did not change when only charts that had concordant answers between patient survey and provider note were compared.
Headache pain quality
The questionnaire allowed patients to select multiple adjectives to describe their pain quality. For this study, headache pain quality was characterized as pulsating (pulsating, throbbing, or pounding), pressure (pressure pushing out, pressure pushing in, dull, or tightening), and/or neuralgiform (sharp, stabbing, burning, or pinching). Pulsating pain and pressure were reported by most participants (79% and 69%, respectively), and neuralgiform pain was reported less often, but still in over half of participants (54%). There were no significant differences across diagnostic groups (Table 2), which remained the case when only charts with concordant answers between patient survey and provider note were compared.
Headache pain quality. Metrics include the total number and percentage of participants in the entire sample, and by diagnostic group who reported head pain that had a pulsating (described as pulsating, throbbing, or pounding), pressure (described as pressure pushing out, pressure pushing in, dull, or tightening), or neuralgiform (described as sharp, stabbing, burning, or pinching) quality. Statistical significance is defined as p < 0.017 based on Benjamini–Hochberg correction for multiple comparisons with FDR of 5%.
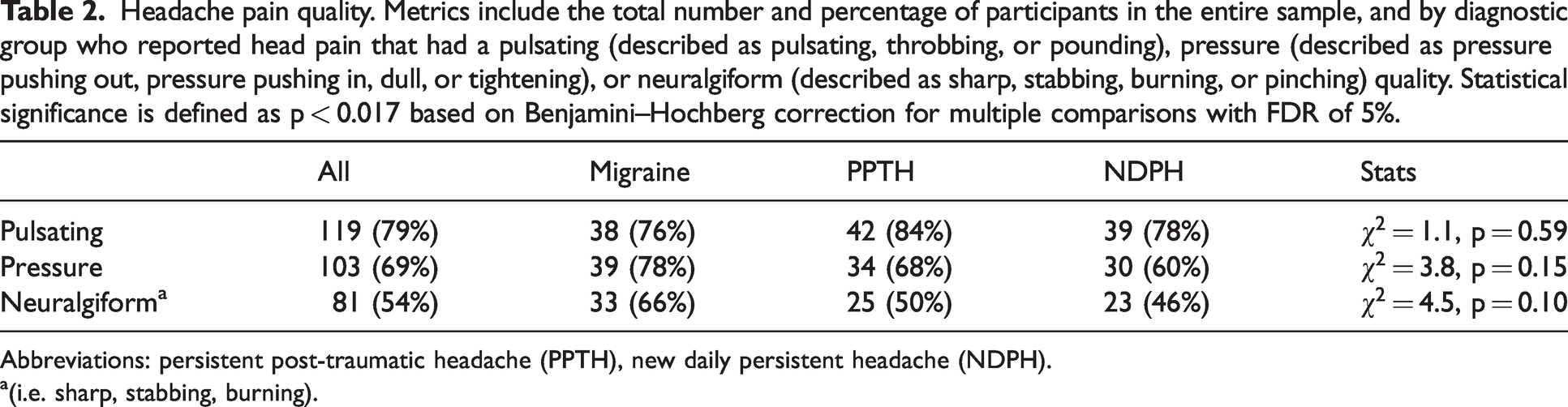
Abbreviations: persistent post-traumatic headache (PPTH), new daily persistent headache (NDPH).a(i.e. sharp, stabbing, burning).
Symptoms associated with headache
The presence or absence of 15 associated symptoms including nausea, vomiting, light sensitivity, and sound sensitivity (the cardinal associated symptoms of migraine), as well as other commonly reported symptoms associated with headache are reported (Table 3). Light sensitivity (69%), sound sensitivity (61%), nausea (60%), difficulty thinking (55%), and light headedness (54%) were the most reported symptoms, present in more than half of participants. Unsurprisingly, the migraine group reported the highest rates of light sensitivity, sound sensitivity, and nausea, which are needed to meet clinical criteria, but these differences did not meet statistical significance.
Symptoms associated with headache. Total number and percentages of participants who endorsed each symptom are shown. Statistical significance is p < 0.0033 based on Benjamini–Hochberg correction for multiple comparisons with FDR of 5%.
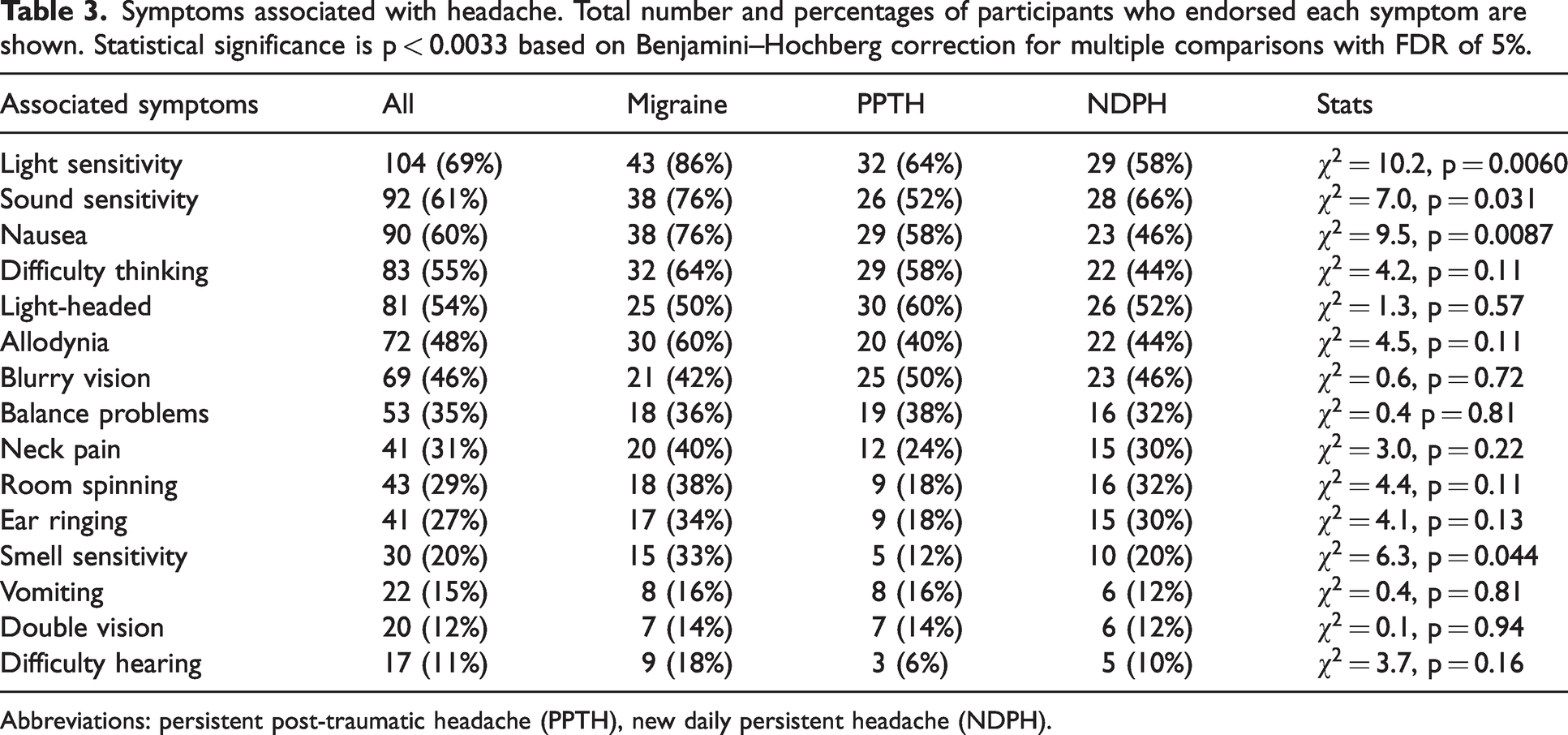
Abbreviations: persistent post-traumatic headache (PPTH), new daily persistent headache (NDPH).
Aura-like symptoms: Information was also collected on visual symptoms, unilateral sensory symptoms, unilateral weakness, and speech/language changes characteristic of migraine aura (Table 4). Visual symptoms were reported most frequently (47%), followed by difficulty with speaking (15%), and unilateral sensory symptoms (11%). Notably, difficulty speaking may have been related to aura or a result of brain fog so this question may overestimate the percentage of participants who had an aura with difficulty speaking. There were no differences across headache diagnosis. We were not able to make a definitive diagnosis of migraine aura based on ICHD-3 criteria because the duration of the symptoms and whether they preceded the headache were not captured in the headache questionnaire. This likely explains why we observed higher rates of these symptoms than the migraine with aura (17). Consistent with prior reports, most participants who reported speaking difficulties or unilateral sensory changes also reported visual aura symptoms (77% and 94%, respectively) with five participants reporting all three aura-like symptoms.
Aura-like symptoms. Total number and percentages of participants who endorsed each symptom are shown. Statistical significance is defined as p < 0.013 based on Benjamini-Hochberg correction for multiple comparisons with FDR of 5%. Unilateral weakness was too infrequent (5%) to be included in statistical analysis.

Abbreviations: persistent post-traumatic headache (PPTH), new daily persistent headache (NDPH).
Features associated with trigeminal autonomic cephalalgias: Unilateral side-locked headache was present in 11% of the entire sample, unilateral autonomic features were present in 5% of the entire sample. Only two participants (one in the PPTH group, and one in the NDPH group) reported both. Overall, rates were low and similar across diagnostic category.
Comparison of symptoms associated across the three groups did not change when only charts that had concordant answers between patient survey and provider note were compared.
Headache triggers
Across the entire sample, the most frequently reported headache triggers were lights (63%), standing up (56%), noises (53%), and stress (51%). Of the 17 headache triggers included in statistical analysis, only two showed significant difference between diagnostic groups based on both Benjamini-Hochberg and Bonferroni correction criteria (Table 5). Reading was more likely to be reported in the PPTH group (
Headache triggers. The number and percentage of 25 headache triggers (including three related to pressure/position changes) across the entire sample, and by headache category are reported. Statistical significance is defined as p < 0.0059 based on Benjamini-Hochberg correction for multiple comparisons with FDR of 5%, and p < 0.0029 based on Bonferroni correction of 17 frequently reported triggers. Lying down (9%), Smoke (7%), chewing (7%), too much sleep (5%), stress let down (4%), high altitude (3%), specific foods (3%), and specific medications (3%) were too infrequently reported to be included in statistical analysis.

Abbreviations: persistent post-traumatic headache (PPTH), new daily persistent headache (NDPH).
Migraine features in PPTH and NDPH
We used ICHD-3 criteria for migraine B – D to determine the percentage of participants in the PPTH group and NDPH group with migraine-type headache (Table 6). Since youth are more likely to have bilateral headache, but focal headache is predictive of migraine in the pediatric population (18), we used focal (i.e. not holocephalic) for criteria C.1. Criteria A was not assessed because it requires that participants had at least four migraines at the onset of continuous headache. Most PPTH (72%) and NDPH (64%) participants met all four diagnostic criteria B–D for migraine, and nearly all participants (98% of each group) met at least two of three criteria B–D.
Percentage of participants meeting criteria for primary ICHD3 headache diagnoses.
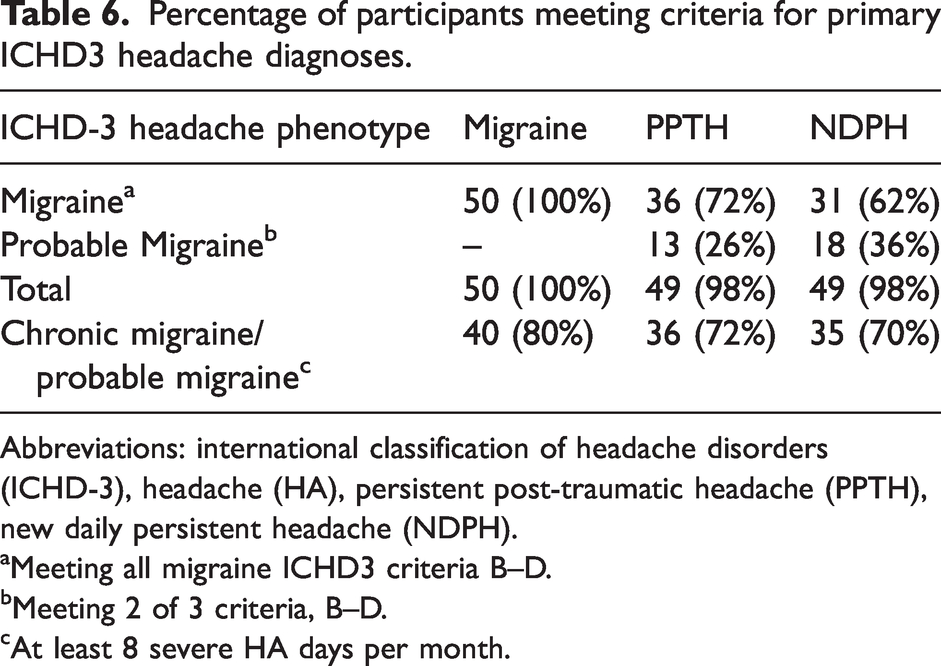
Abbreviations: international classification of headache disorders (ICHD-3), headache (HA), persistent post-traumatic headache (PPTH), new daily persistent headache (NDPH).
Meeting all migraine ICHD3 criteria B–D.
Meeting 2 of 3 criteria, B–D.
At least 8 severe HA days per month.
Post-hoc sub-analysis of bimodal NDPH usual pain severity
The NDPH group showed a bimodal distribution of headache pain severity, which was different from the other two diagnostic categories, despite having a similar median and distribution to the other two groups. This suggests that headache features in NDPH may be more nuanced. To determine if other headache characteristics differed between those with NDPH with low usual headache pain severity (pain score of 1–5) and high usual headache severity (pain score of 6–10), we did a sub-analysis comparing these two groups (6–10; Table S1). Those in the NDPH group with high usual severity reported significantly greater headache-related disability, more frequent severe headache exacerbations, and were more likely to report neuralgiform pain. However, they did not significantly differ in the rate of migraine headache reported, the prevalence of pulsating pain or pressure, any associated headache features, or headache triggers.
Discussion
Although continuous headaches have been studied in this age group (1,4), this is the first age- and sex-matched study to demonstrate that youth with continuous headache consistent with migraine, PPTH, or NDPH are strikingly similar across an extensive evaluation of headache features. This is particularly remarkable because a diagnosis of migraine requires that specific headache features are present, while PPTH and NDPH are defined solely by the circumstances of their onset. Our study design has an advantage over prior work because it carefully controls for critical confounding variables including sex and age, treatment, and duration of continuous headache.
Continuous headache is a scarcely studied and poorly defined condition. Chronic migraine with continuous headache is currently included in the appendix of the ICHD-3 (2), indicating that this is an area requiring further exploration and clarification. Under ICHD-3, continuous headache can also be classified as PPTH or NDPH. Our study provides a full characterization of youth with continuous headache across these three diagnoses, which adds to mounting evidence that headache features of NDPH and PPTH are not distinct from migraine. Indeed, most participants in the PPTH and NDPH groups had headaches consistent with migraine, and nearly all reported headache features consistent with migraine or probable migraine. While other headache types have been reported, our data suggest that they make up a small proportion of all affected individuals. Prior work has suggested that there is a higher prevalence of vestibular symptoms and brainstem aura in adults with NDPH (10). While our questionnaire was not able to specifically address brainstem aura, we did not find audio-vestibular symptoms (i.e. room spinning, ear ringing, double vision) to be more prevalent in NDPH than migraine or PPTH.
These findings indicate that the majority of PPTH and NDPH represent circumstances or precipitants that lead to the abrupt onset of migraine pathophysiology (1,4–9). In the case of PPTH, the precipitant is head trauma. The precipitant is less clear for NDPH, though a viral prodrome, stressful life events, and start of school have been associated with the onset of NDPH (19,20). Consistent with this assertion, multiple studies implicate sensitization of the trigeminal nociceptive system, the cornerstone of migraine pathogenesis, in PPTH (21). Relatively little work has examined the pathophysiology of NDPH (19), though cerebral spinal fluid tumor necrosis factor alpha levels were found to be similarly elevated in individuals with NDPH, chronic migraine, and PTH (22). Instead of considering migraine specifically as a paroxysmal condition that can become chronic over time, it may be better reframed as a predisposition to trigeminal nociceptive sensitization that can start abruptly under certain circumstances. Essentially, this work suggests reframing the ICHD criteria to consider phenotype (migraine, tension-type, etc) versus etiology (trauma-triggered, idiopathic once secondary causes have been excluded, etc). This suggestion should be tested with studies of pathophysiology, but such a change would impact not only diagnosis, but also clinical trial design. As continuous headache is a rare but disabling condition, increased enrollment of these patients in clinical trials is desirable. Indeed, treatment guidance is significantly limited across all three diagnoses in children and adolescents. More treatment options are available for migraine (23) than NDPH and PPTH in youth. Our findings indicate that the majority of individuals with NDPH and PPTH cannot be distinguished from those with migraine based on clinical features, and expert opinion suggests that headache management in NDPH and PPTH should be based on the headache disorder clinical features most resemble (19,24,25).
While very few differences were noted across headache diagnoses, youth with PPTH were more likely to report reading as a headache trigger. This finding should be interpreted cautiously because our sample was not specifically powered to identify differences in associated headache symptoms or headache triggers, though it remained significant even when adjusting for multiple comparisons with multiple methods. It also fits our clinical experience. It may be that these youth were more likely to have seen concussion specialists and were primed to recognize reading as a trigger. However, the PPTH diagnostic group was no more likely to report exercise as a trigger, which is also discussed frequently after concussion, making this explanation less likely. This instead may reflect challenges with eye tracking (26) or cognition (27), which are commonly reported in concussion.
The NDPH group did show a bimodal distribution of usual headache severity, which could have indicated different headache types. However, we found that those with high and low headache severity differed across all headache burden metrics but did not significantly differ in the rate of migraine-type headache, or other headache characteristics except for a greater prevalence of neuralgiform pain in the higher headache severity group. This suggests that the bimodal distribution is associated with differences in headache burden rather than headache “phenotype” (i.e. migraine, tension-type headache, trigeminal autonomic cephalalgia, etc.).
A few limitations of our study should be noted. First, there is a referral bias since only participants who had severe enough headaches to be seen in a general neurology or headache clinic were included. It should be noted, however, that because our study focuses on continuous headache, it is conceivable that individuals with a continuous headache regardless of severity or other symptoms would be more likely to seek neurologic care. Second, diagnosis was based on ICHD-3 criteria for patient and parent reported data. As a result, our dataset is vulnerable to patient or parent misinterpretation of the questions, and therefore it is possible an entry could have been mis-categorized by the diagnostic algorithm. The advantage of using a diagnostic algorithm for diagnosis based on patient and parent responses is that it is unbiased by clinical decision making, and awareness of the current diagnostic categories. Post-hoc chart review indicated that there was discrepancy between patient answers and provider documentation for 34% of participants. Importantly, headache features of discrepant charts did not differ from charts where patient responses and provider documentation were concordant, and only comparing the concordant charts did not substantially change the outcomes. Finally, our cohort was predominantly female beyond what would be expected even given the female predominance in chronic headache disorders (28).
Our dataset specifically focuses on the clinical presentation of youth with continuous headache for at least three months who met strict criteria for PPTH, NDPH, or migraine. Three months is a somewhat arbitrary cut-off, chosen to mirror ICHD-3 duration requirements diagnosis of chronic migraine, PPTH, and NDPH (2). Further work is needed to determine if these findings apply to youth with continuous headache for less than three months, youth without continuous headache, and in diagnostic gray areas between migraine, NDPH, and PPTH. It is unclear if our findings are generalizable to adults. Children and adolescents are less likely to have declared themselves as having migraine than adults because the peak incidence of migraine occurs in the 3rd decade of life (29). It may be that head trauma, viral illness, or stressful life events are more likely to uncover a predisposition to migraine in children compared to adults, though further work is needed to address this.
In summary, our data indicate that headache features do not differ in youth with continuous headache who have headache onset consistent with migraine, PPTH, and NDPH, which calls their diagnostic distinction into question. Similar phenotypes suggest, but do not confirm, shared pathophysiology. Objective biomarkers would still be ideal to classify headache disorders, but in absence of this, different ways of clinically reframing headache to aid in management should also be considered.
Clinical implications
Continuous headache is a poorly characterized condition that can be classified by the ICHD-3 under different diagnoses. Youth with continuous headache report remarkably similar clinical features whether their headache onset is consistent with migraine, persistent post-traumatic headache, or new daily persistent headache. Our findings are consistent with the proposal that most persistent post-traumatic headache and new daily persistent headache can be characterized as abrupt onset of migraine.
Contributions
CPG was involved in the study design, wrote the pre-registration document, confirmed the diagnostic algorithm, performed the data analysis, generated the figures, and wrote the manuscript. GKA provided feedback on data analysis and on the manuscript. ADH was involved in design of the intake questionnaire, the study design, and provided feedback on data analysis and the manuscript. C.S generated the headache questionnaire and manages the database, designed, and implemented the diagnostic algorithm, was involved in the study design, and edited the manuscript.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024221131331 - Supplemental material for Comparison of continuous headache features in youth with migraine, new daily persistent headache, and persistent post-traumatic headache
Supplemental material, sj-pdf-1-cep-10.1177_03331024221131331 for Comparison of continuous headache features in youth with migraine, new daily persistent headache, and persistent post-traumatic headache by Carlyn Patterson Gentile, Geoffrey K Aguirre, Andrew D Hershey and Christina L Szperka in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Neurological Disorders and Stroke of the National Institutes of Health NIH NINDS K23NS124986 (to C.P.G) and K23NS102521 (to C.L.S.), the American Academy of Neurology Clinical Research Scholarship (to C.P.G.), the International Headache Academy Research Fellowship (to C.P.G.), the Minds Matter Frontier Program grant from the Children’s Hospital of Philadelphia (to C.P.G.), and Department of Defense Grant W81XWH-151-0447 (to G.K.A.). Pfizer Grant for Learning and Change supported the development of the patient questionnaire and registry (C.L.S.).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.