
Abstract
Background
In this manuscript, we aim to systematically estimate the pooled prevalence and incidence of primary headaches and its subtypes (migraine, tension-type headache, and chronic headaches) in Latin America and the Caribbean, describing its epidemiological profile and associated factors.
Methods
We systematically searched PubMed/MEDLINE, Scopus, and LILACS (From conception to March 2021), for populational studies reporting the epidemiology of primary headaches and their associated factors in Latin America and the Caribbean. The data extraction was conducted independently. We performed random-effect model meta-analysis of prevalence (overall primary headaches and by subtypes) and associated factors, assessed potential sources of heterogeneity, the risk of bias, publication bias, and the evidence certainty (GRADE methodology).
Results
We included 32 populational studies (38 subpopulations, n = 63,813). The prevalence of primary headaches was 41.4% (95% CI 31.1–52.2%; n = 54,357), 15% for migraine (95% CI 12.0–18.3; n = 53,658 individuals), 20.6% for tension-type headache (95% CI 12.4–30.2; n = 25,840), and 6% for chronic headaches (95% CI 3.3–9.6; n = 21,720), with high between-study heterogeneity. No incidence data was found. Female sex, white ethnicity, high BMI, comorbid mental health disorders, and low-back pain were associated with higher prevalence of primary headaches. The prevalence was less in rural areas.
Conclusion
In Latin America and the Caribbean, primary headaches are highly prevalent affecting young females disproportionally. The prevalence of chronic headaches is higher than in other systematic global and regional estimations. The presence of comorbidities as modifiable risk factors should encourage their integration as targets for community-based preventive and therapeutic interventions.
Protocol registration number
CRD42018105116
Introduction
Among patients with headache disorders, primary headaches, including migraine and tension-type headache (TTH), constitute more than 90% of cases (1–3). Between 1990 and 2019, the burden associated with migraines and tension-type headaches increased worldwide by 56.7% in absolute values of disability adjusted life years (DALYs) but with an age-standardized rate increment of 1.1% (2,4). These small increments after age-standardization could be potentially explained due to changes in the age distribution of the disease, however maintaining similar burden rates over decades, it remains a burdensome diagnosis in neurology and primary care.
Despite its high relevance for health policy, only a few studies have investigated headache disorders' global and regional epidemiology. Stovner et al. (5) estimated the global prevalence of primary headaches to be around 46%, while in Central and South America it ranged from 6.8% to 93.5%, suggesting a high regional heterogeneity. In 2017, Woldeamanuel et al. (6) estimated the global prevalence of migraines to be 11.6% and 16.4% for Central and South America. However, those studies did not explore the primary headaches subtypes and their associated factors, moreover, the systematic search is outdated and require additional meta-analytic methods to explore the clinical and methodological potential sources of heterogeneity in the region.
Given the region's economic, political, and social complexity, the countries forming the Latin America and the Caribbean (LAC) region are at different levels of development, and the health resources available vary significantly within and between countries (7). Therefore, estimating a precise epidemiological profile of the attributable burden of primary headaches in the region is required for setting health priorities. Nevertheless, to the best of our knowledge, no previous systematic assessment focused on LAC analyzed the epidemiological profile of primary headaches, including all its subtypes, and potential related factors. The aim of this study is to perform a systematic review and meta-analysis to estimate the pooled prevalence, incidence, and associated factors of primary headaches in LAC, describe their trends over time, and explore sources that could explain the heterogeneity in the region.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) (8) guidelines and the Cochrane Handbook for Systematic Reviews of Interventions (9). Additionally, we used the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) checklist to present our findings (10). The protocol was registered in PROSPERO (CRD42018105116).
Systematic search and inclusion criteria
We searched in PubMed/MEDLINE, Scopus, and LILACS databases until March 10, 2021. The search strategy was formulated by experienced authors (CMM, KPB and CAD) and is presented in online Supplementary Table 1. Additionally, we reviewed the references of a previously published systematic review (6) and the references of the included studies. We did not contact additional authors. The eligibility criteria included: 1) population-based studies reporting the prevalence and/or incidence of global primary headache disorders such as migraines, tension-type headaches (TTH), and other primary headache disorders; or primary headaches reported under the term “chronic,”; 2) study population belonging to a LAC country; 3) full-text accessible. We did not exclude studies based on date or language. Finally, we accepted all definitions of headaches reported in the studies, including ICHD-I, -II, -III (11–13), and ICD-10 (14).
Study selection and data extraction
After removing duplicates, two authors (AHR, and RAM) independently reviewed records by titles and abstracts, and then by full text. Discrepancies were verified with a fourth reviewer (CAD or KPB), achieving consensus by discussion. Data extraction from each selected study was conducted independently. The data was extracted for calculating the prevalence estimates of primary headaches (overall, TTH, migraine or chronic) as sample size, population, number of cases; and the characteristics of the study and the study population: author, publication year, country, age, sampled population, detection method, sampling method, diagnostic criteria (according to the classification ICHD-I or -II; other than ICHD, and unspecified), data by sex. The extracted data was tabulated, coded, and imported into a datasheet for analysis.
Quality evaluation in individual studies
Two reviewers (CMM and CAD) conducted quality assessment using Loney et al. (15) instrument for prevalence/incidence studies. The tool presents three categories: 1) sampling, 2) measurement and 3) population analysis. Scores varied from 0 to 8, with higher scores indicating higher quality (“high quality”: 7 and 8; “moderate quality”: 5 and 6; “low quality”: 3 and 4; and “very low quality”: 2 or less). Discrepancies were solved by a third reviewer (KPB).
Statistical analysis
We conducted random-effects model meta-analysis (DerSimonian and Laird method) (16) of the prevalence rates of primary headaches and its subtypes in percentages with 95% exact method CI (17), calculated in percentage by a binomial model (“metaprop”) with variances previously stabilized by the Freeman-Tukey Double Arcsine transformation (18). Between-study heterogeneity was evaluated with I2 statistics (I2 < 40%, I2 = 30–60%, I2 = 50–90%, and I2 = 75–100% were considered to indicate low, moderate, substantial, and considerable heterogeneity, respectively) (19). We expected high heterogeneity since we included epidemiologic studies from diverse countries with different distributions of health determinants. To overcome this limitation random-effect meta-analyses were planned. Despite this, epidemiologic meta-analysis remains informative for prioritizing decisions in public health. Sources of heterogeneity were explored with the subgroup and sensitivity analyses by sex, diagnostic criteria, type of population, quality assessment, sample size, and representative sample. Temporal trends of prevalence estimates were evaluated using random-effects cumulative meta-analysis. Moreover, in order to test moderators at the study-level we conducted univariate and multivariate random-effect meta-regression analysis (20), following the recommendations of Thompson and Higgins (21), testing each moderator on at least eight primary studies. The best model was chosen after evaluating the residual percentage of heterogeneity, the proportion of between-study variance explained (adjusted R2), and significant moderator (p < 0.05). We included categorical and continuous variables as sample mean age, setting, WHO mortality region (group A: very low child and adult mortality, B: low child and adult mortality, C: low child and high adult mortality, D: high child and adult mortality, and E: high child and very high adult mortality), sample number, quality of the studies, male/female proportions, human development index (HDI), and urban index. To adjust for the high false positive rates usually associated with meta-regressions, we used a Monte Carlo permutation test with 10 000 random permutations. Publication bias was assessed visually by funnel plots and statistically by the Egger’s regression test (22), we adjusted publication bias using the meta-trim method. Finally, we extracted the factors reported by the primary studies including epidemiological, clinical, and demographic characteristics, using the raw data to construct two-by-two tables to calculate individual odds ratios (OR) and corresponding 95% CI. We pooled OR using random-effect model meta-analyses. The statistical analyses were conducted in STATA v.17.
Evidence certainty
The certain of evidence was assessed following the approach as in our previously published articles (23–26). We used the five domains described in the GRADE handbook: study limitations (the risk of bias of the primary studies), imprecision (appropriateness of the sample size and width of the CI), indirectness (generalizability of results), inconsistency (between-study heterogeneity), and publication bias (27). The evidence was classified as of high, moderate, low, or very low certainty (28).
Results
Details of the selection process can be found in online Supplementary Figure 1. After duplicate cleansing, we screened 1326 records, assessing 61 by full text with 22 not meeting the inclusion criteria (29–50). Reasons for exclusion are explained in online Supplementary Table 2. Finally, 38 records were included (one from the manual search [51–89). Some studies presented their results in complementary manuscripts (da Silva et al., n = 3 records [59,67,88]; Lavados and Tenhamm, n = 2 [68,69]; Queiroz et al., n = 3 [78–80]; Quesada-Vázquez et al., n = 2 [81,82]; Rueda-Sánchez et al. n = 2 [84,85]). Other studies included more than one population in their cohorts and were analyzed separately (Morillo et al. [73], n = 6 subpopulations; Silva et al. [87], n = 2). Therefore, 32 studies representing 38 subpopulations were analyzed.
From the 38 cohorts, data from only 11 out of the 33 LAC countries were published. Most of them were from Brazil (n = 18) and were conducted from 1983 to 2019. Three cohorts were from high income countries, while the rest belonged to upper-middle income countries. The most frequent setting was urban (76%) and 29% were conducted exclusively in children.
Regarding methods, 74% used a period or point-type prevalence definition and the preferred detection method was door-to-door screening (58%). Case definitions were based in the ICHD-I criteria (34%), the ICHD-II (32%), or not specified/others. The complete description of the included studies is presented in online Supplementary Table 3.
Quality of the included studies
The 38 subpopulations were assessed independently. Most of them reached a moderate quality (45%, n = 17), 13 had low quality (34%) and eight had high quality scores (21%). Twenty cohorts achieved a response rate of ≥70%. Eighteen cohorts included detailed participant information. Only 15 cohorts reported their results appropriately using 95% confidence intervals. The complete assessment is shown in online Supplementary Table 4.
Pooled estimates
We conducted separated meta-analysis for overall primary headaches, migraine, TTH, and chronic headaches (Figure 1). No incidence data was found. Additionally, a summary of all the estimates from the secondary outcomes are shown in Table 1.

Forest plots of the prevalence of primary headache disorders in LAC.
Summary of prevalence estimates from secondary analysis.

Note: n: number of studies included; %: prevalence estimates in percentages; CI: confidence intervals; I2: Statistic assessment of heterogeneity; ICDH-I and -II: International Classification of Headache Disorders first and second editions; IW: interview; WHO regions: World Health Organization regions based on mortality strata of children younger than five years and male adults between 15 and 49 years of age classified from A to E; Region A: Very low child mortality rate and very low adult mortality rate (Cuba); Region B: low child and adult mortality rates (i.e. Argentina, Brazil, Chile, Colombia, Mexico, Panama, etc.); Region D: High child and adult mortality rates (Bolivia, Ecuador, Guatemala, Haiti, Nicaragua, Peru). Countries from regions C and E are not present in this study.
Overall Primary Headaches
Thirty subpopulations from 29 studies were included for this analysis (51–53,55–58,60–64,66–72,74–81,83–89). The total number of individuals included were 54,357; from them, 20,828 cases of primary headache disorders were diagnosed. The overall prevalence of primary headache disorders was per 41.43% (95% CI: 31.06%–52.20%; I2 = 99.85%). The prevalence was twice as high in females than in males (25.25%, 95% CI: 18.10–33.13 vs 13.45%, 95% CI: 9.76–17.66). It was higher in studies with lower quality and studies with only adult individuals; and it was lower in studies in rural setting and in countries that belong to WHO-region D. No differences were found by sample size, headache diagnostic criteria, local or regional/national study scope, type of case detection method, income categories, or prevalence definition.
Migraine
Thirty-one subpopulations from 26 studies reported data for migraine analysis (51,53–57,61,64–66,68,70–77,79,82–86,89) (53,658 individuals; 5993 cases). The prevalence of migraine was 15.03% (95% CI: 12.04%–18.29%; I2 = 99.01%). It was almost four times higher in females than in males (12.78%, 95% CI: 9.19–16.85 vs 3.50%, 95% CI: 2.47–4.69). Prevalence was higher in studies with a sample size smaller than 500 individuals. It was lower in studies with lower quality, and those that did not use the ICHD criteria for case definitions. Studies from rural settings and from WHO-region A had lower prevalence; however, confidence intervals slightly overlapped with the other categories. No further differences were found.
Tension-type Headache
We included fourteen studies (53–57,61,63,69,71,77,80,81,83,89) (25,840 individuals; 4276 cases). The prevalence of TTH was 20.58% (95% CI: 12.39%–30.20%; I2 = 99.68%). It was almost twenty times lower in rural compared to urban settings (1.77%, 95% CI: 1.39–2.19 vs 22.18%, 95% CI: 11.40–35.30), lower in the studies from regional and national scope and those from countries of the WHO-region A; however, with overlapping confidence intervals. No other differences were found in subgroup analysis.
Chronic Headache
Ten studies (53,57,61,68,69,71,77,78,81,82,84,85,89) (21,720 individuals; 948 cases) were analyzed. The prevalence of chronic headache was 6.05% (95% CI: 3.26%–9.62%; I2 = 98.51%). It was lower in studies with greater sample sizes, from rural settings, those that included only participants younger than 20 years old, studies that interviewed the participants face-to-face, and those from countries of WHO-region B. It was higher in women and in studies from countries of high income; however, confidence intervals overlapped.
Geographical assessment
The countries with the highest prevalence of primary headaches were Brazil, Cuba, and Argentina. Colombia had the highest prevalence of migraine and TTH, while Cuba had the highest prevalence of chronic headaches (Figure 2).

Prevalence of primary headache disorders in LAC by country.
Associated factors
For primary headaches, we found that being female (OR: 1.9, 95% CI:1.5 to 2.4), being of white ethnicity (OR:1.3, 95% CI: 1.1 to 1.6), having comorbid mental disorders, mainly depression and anxiety, (OR: 4.6, 95% CI: 3.9 to 5.3), being overweight/obese (OR: 1.6, 95% CI: 1.2 to 2.2), and having low back pain were positive associated factors. In the case of migraine, being female was associated with higher odds of having the diagnosis (OR:2.6, 95% CI:2.0 to 3.3) while having the diagnosis of hypertension was associated with lower odds (OR:0.4, 95%CI: 0.3 to 0.6). Additionally, being a female was associated with higher odds of having chronic headache (OR:2.2, 95% CI:1.6 to 2.9). The ORs summary is presented in Table 2.
Primary headache disorders associated factors.
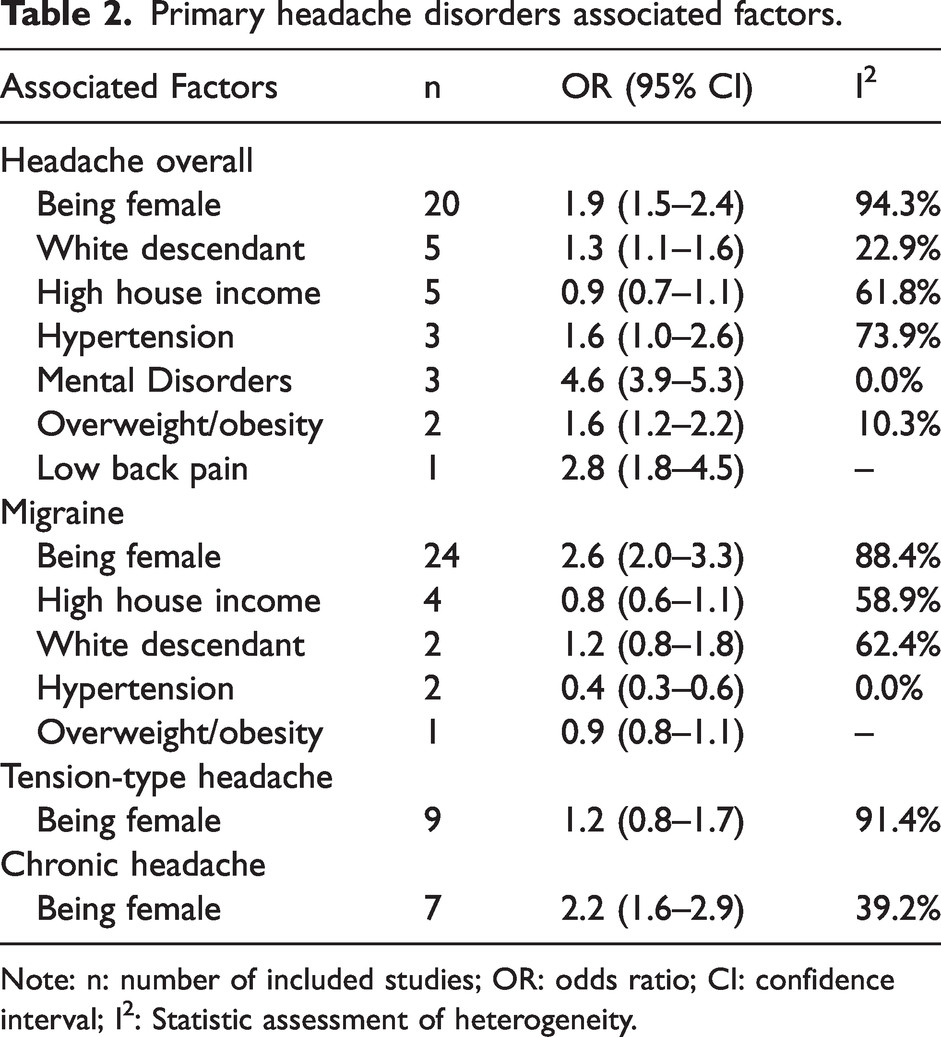
Note: n: number of included studies; OR: odds ratio; CI: confidence interval; I2: Statistic assessment of heterogeneity.
Cumulative meta-analysis
Primary headaches increased from 8.18% to 48.85% since 1985 until 2009, and then diminished progressively to the current value. Migraine prevalence increased from 3.68% to 17.10% since 1985 until 2006 and then remained still to date. On the other hand, the prevalence of TTH showed a negative trend from 72.30% to 23.15% in the last decades. Finally, the prevalence of chronic headaches had remained still since 2002 (online Supplementary Figures 2 to 5).
Heterogeneity assessment
The magnitude of the heterogeneity (I2) found in these analyses varied from 91.09 to 99.85%. The estimates from the secondary outcomes, the subgroup and sensitivity analysis are summarized in Table 1. Female sex was the most important modifier for the prevalence estimates (25.2% overall prevalence in females vs. 13.5% in males). Other modifiers were rural setting (12% overall prevalence in rural areas vs 48% in urban and 36.1% mixed settings), belonging to different WHO-epidemiological regions (22.5% overall prevalence in region D vs. 43.3% in region B and 44.7% in region A), and the participants’ age group (22.7% overall prevalence in studies including all ages vs. 56% in those including only adults and 36.0% in those including only youth). The most important methodological variables were the studies’ quality (42.4% and 47.2% overall prevalence in studies with high and moderate quality respectively vs. 22.2% in low quality studies), the sample size (11.6% migraine prevalence in studies including more than 500 individuals vs 27.1% in those including less individuals), and the diagnostic method (0.8% prevalence of chronic headaches in patients recruited by in-person interviews vs 7.7% in those recruited in door-to-door studies). According to the univariate meta-regression analysis, there was a positive association between the sample mean age and a negative association with rural setting for the prevalence of primary headaches. For migraine, we found a positive association with the quality of the studies (β-coefficient: 7.2; p-value:0.001), the sample size (β-coefficient: 15.1; p-value:0.001), and the proportion of females in the sample (β-coefficient: 78.6; p-value <0.001). Countries with higher HDI had a lower prevalence of TTH (β-coefficient: −376.7; p-value:0.016). Finally, for the prevalence of chronic headache, we found a positive association with the proportion of females in the sample (β-coefficient: 39.9, p-value: 0.005), and a negative association with studies from rural setting (β-coefficient: −5.2; p-value:0.024), and the countries’ index of urbanization (β-coefficient: −0.81; p-value:0.011). In the multivariate analysis, there was a positive association between the mean age of the participants (β-coefficient: 0.9; p-value:0.001) and belonging to WHO region-B (β-coefficient: 35.9; p-value:0.019) with a higher prevalence of primary headaches. Additionally, the prevalence of migraine was associated with the proportion of females in the sample (β-coefficient: 55.1; p-value:0.006). The summary of the meta-regression results could be found in online Supplementary Table 5.
Publication bias
We found no publication bias in the analysis of the prevalence of primary headaches and chronic headache. By visual inspection, we found publication bias in the analysis of migraine and TTH (online Supplementary Text 1 and online Supplementary Figures 58 to 63). After publication bias adjustment (meta-trim), the new estimates were 9.55% (95% CI 6.52−12.60) and 11.17% (95% CI 1.50–20.85) for migraine and TTH, respectively.
Evidence certainty
The evidence certainty was low for the analyses of primary headaches, migraine and TTH. For chronic primary headaches the level of certainty was moderate. All the assessments started from high certainty because only population-based studies were included, and we did not downgrade the evidence due to inconsistency (since high heterogeneity was expected for this epidemiological data). Details are presented in Table 3.
Summary of findings of GRADE evaluation.

Discussion
To the best of our knowledge, this is the first systematic review assessing the epidemiologic profile of primary headaches in LAC. We found a pooled prevalence of primary headaches of 41.4%; similar to the reported worldwide in 2007 (47%) and for Central/South American countries (40%) (despite using different methodology a decade ago) (90), but lower that the value reported for Europe (53%) (91). The prevalence of tension-type headache was 20.6%. This estimate was lower than value reported in the Global Burden of Disease study (GBD) 2016 report, where the global age-standardized prevalence rate of TTH was 26.1% (95% UI, 23.6–29.0) with 10.4% of the cases being from LAC countries (92). Hence, we found lower estimates of TTH. Despite being a potentially under-reported condition (93), the included studies actively search for TTH, making our estimates closer to the reality.
The prevalence of migraine was 15.0%. The global prevalence of migraine is 11.6% (95%, CI 10.7-12.6%), with Central and South American countries having a higher estimate (16.4%) (6). Our results are closer to the latter value. The pathophysiology of migraine suggests a strong organic (94) and genetic component (95). In LAC, some environmental factors related to migraine could influence this estimate, such as the increasing prevalence of obesity in the general population (96–98), air pollution (99,100), and the geographic aspect of the region, since living at a high altitudes could increase the prevalence and severity of migraine (101). Moving to high altitudes also increases the risk of having a migraine episode, which increases the risk of any type of headache (102). One last factor that requires further exploration is the consumption of caffeine (103), which is high in the region and especially in Brazil (104), where most of the included studies were conducted.
We found high prevalence of chronic headache (6.1%). The global prevalence of chronic migraine ranged from 0 to 5.1% (105), this last result being from a Brazilian study (77). Similarly, a systematic review of the Asia Pacific region found a median prevalence of chronic daily headache of 2.9% in general population and a prevalence of 1 to 1.7% for chronic migraine (106). Up to 70% of the patients with chronic headaches disorders had medication overuse headache (MOH) (107). Access to triptans and migraine preventive treatments, the gold standard medications, are limited in LAC countries due to their cost and poor insurance coverage (108), and self-medication is poorly regulated, hence other drugs such as analgesics and ergotamines (in LAC, MOH is of ergotamine predominance) (108) are frequently purchased (109).
Finally, after cumulative meta-analysis we found that the prevalence of primary headaches had increased over time. Our results showed an increment in the prevalence of migraine and a decrease in the prevalence of tension-type headache, since those two disorders shared common triggers these trends may be explained by more accurate diagnosis of migraine over time.
We found that biological sex was the most important factor explaining the heterogeneity with a double fold prevalence of primary headaches for females and fourfold for migraine and chronic headaches. The results were robust not only for the association analysis with significant ORs, but also after the meta-regression with significant coefficients. Overall, females have a higher risk for developing pain disorders (110). A previous systematic review of worldwide migraine prevalence reported a higher proportion of migraine in females than in men (13.8% vs 6.9%) (6). Additionally, the GBD study 2016 reported that headache disorders in females between 15 and 49 years old, represented 11.2% of all Years Lived with Disability (YLD) (92). The classic hormonal theory suggests that since menarche, female prevalence of migraine begins to rise, presumably by the increment of female hormones like estrogen, and progesterone which is more pronounced during the late luteal phase (111).
For chronic headaches, this could be explained as migraine is the type of primary headache with the highest risk of chronification (112) with female sex as one non-modifiable determinant in this process (113). On the other hand, we did not find a gender predominance for tension-type headache (TTH), which is similar to the GBD study 2016 (92).
Besides the biological role of sex-associated features, the concept of female gender generates a set of cross-sectional inequities that are translated in disadvantages in social, political, and health access (114). The Gender Inequality Index, which is a comparation of measures of achievements in reproductive health, empowerment, and position in the work market between women and men, remain as five times higher in LAC countries such Guatemala, Nicaragua and Bolivia (115). As a consequence, females have less access to healthcare provision. All of these disparities could contribute to explain the high prevalence of headache disorders in Latin American females.
The prevalence of primary headaches was higher in studies including only adults with menstruating females as the most affected group. As mentioned, migraine intensity and recurrence are associated with hormonal changes in the menstrual cycle (116). Overall, primary headaches impact the individual’s productivity and commonly produce both absenteeism (not going to work) and presenteeism (going to work while unhealthy) (117). Consequently, headache disorders are responsible for the high costs involved with this, in Europe this is estimated to be around 173 billion euros annually (118).
We found a higher prevalence of primary headaches in urban settings, with the association confirmed by the meta-regression. A previous systemic review of global studies found a higher prevalence of migraine in urban settings (6). From a social viewpoint, living in an urban area is associated with increased risk for chronic stress (119). It is suggested that functional neural changes occur when living in a city that increase the activity of brain regions related to stress processing, explaining a higher vulnerability of city dwellers for primary headaches (120), as stress is the most frequent trigger of all primary headaches (121). Consumption of ultra-processed food is higher in urban areas (122), while consumption of a healthy diet including omega-3, probiotics or fiber could modulate the gut microbiota and gut brain axis with potential benefits for migraine (123).
We found that mental health disorders such as depression, anxiety, and stress were associated with primary headaches. Stress is the most frequent trigger of primary headaches (121), with other triggers being sleep alterations and emotionally adverse situations (121). According to a study across the European Union, both depression and anxiety were associated with MOH, while anxiety by itself was associated with TTH (124). Also, the diagnosis of depression is a predictor for migraine progression from episodic to a chronic condition (125). There is also overlap between headaches and psychiatric conditions like depression and anxiety, since headache could be one symptom, a trigger or a consequence (126). As expected, the prevalence of suicidal ideation and suicidal attempt is high in patients with migraine (127), contributing to mortality in an indirect manner. Additionally, we found that a higher-than-normal body-mass index (overweight and obesity) was associated with headaches. This was aligned to previous studies showing that high BMI increases the disability of headaches in adults and in children (128). Thus, suggesting an opportunity for primary headache disorders (PHD) prevention reducing the risk of obesity.
Limitations
First, the studies included in this analysis were published from a limited number of LAC countries, hence reducing the representativeness. Additionally, this study was limited by the high heterogeneity and low to moderate evidence quality. Publication bias was present for the meta-analysis of migraine and TTH.
Conclusion and research recommendations
Primary headaches are highly prevalent in LAC countries, similar to other world regions. However, chronic headaches may have an even higher prevalence in LAC countries than in other areas, which could be explained by different LAC specific factors, such as deficits in acute pain management and limited access to preventive therapy. These conditions disproportionally affect young females. Several LAC countries still need to report their epidemiological data on headaches, including descriptions of important known and potentially associated factors (age, sex, BMI, comorbidities, medication received, etc.). That will allow us to understand the true impact of primary headaches in the region. These epidemiological studies at a national level are of utmost importance in improving public healthcare planning and resource allocation for each country within the LAC region. In this study we used the definition of chronic daily headaches for the inclusion of chronic headache studies. Nevertheless, the operational definitions of chronic headaches in epidemiologic investigations requires further exploration and dedicated analysis. Additional research in this topic is required. Obesity, mental health disorders, and other chronic pain conditions are modifiable factors in the region that should be further explored and managed. Community-based interventions targeting control of associated factors and improvement of the acute episodes management and preventive interventions are needed in the region.
Public health relevance
Primary headaches disorders are highly prevalent in Latin America (41%). The burden of primary headaches is disproportionally higher in females. Many risk factors for primary headaches are controllable or modifiable, such as comorbid mental health disorders, high BMI and low-back pain. Chronic headache disorders are more prevalent in the region as compared to the worldwide systematic estimates, presumably reflecting deficits in the management of the acute episode and inadequate use of preventive medication.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.