
Abstract
Background
Restless legs syndrome (RLS) is increasingly being reported as a comorbidity of migraine.
Methods
We conducted a systematic review and meta-analysis of studies investigating RLS in headache/migraine and vice versa. We calculated the prevalence and 95% confidence intervals (CI) of RLS in headache/migraine, of headache/migraine in RLS and controls, and odds ratios (ORs) of the association between the conditions. We then determined pooled effect estimates for the associations.
Results
We identified 24 studies. RLS prevalence in migraine ranged from 8.7% to 39.0% with no apparent differences based on gender and aura status. Prevalence among controls was compatible with the literature. Migraine prevalence in RLS ranged from 15.1% to 62.6%. We did not pool prevalence data because of high unexplained heterogeneity. High heterogeneity with respect to the association between any migraine and RLS could be explained by study design. Pooled analyses showed substantially higher effect estimates in case-control studies (pooled OR = 4.19, 95% CI 3.07–5.71; I 2 = 0.0%) than in cohort studies (pooled OR = 1.22, 95% CI 1.14–1.30; I 2 = 0.0%).
Conclusion
Our results support the concept of RLS as an important comorbidity of migraine. However, the degree of association appears to be strongly determined by study design. Potential effects by gender and aura status and the role of RLS in other headache disorders remain unclear.
Introduction
Migraine is a common, chronic neurological disorder affecting 10%–20% of the general population, predominantly women (1). It presents with recurrent headache attacks, associated vegetative symptoms, and hypersensitivity of various functional systems of the nervous system (1).
The comorbidity burden of migraine is high, and among the disorders most firmly associated with migraine are for example cardiovascular disease (CVD), in particular stroke (2), depression (3), and other pain disorders (4,5).
In addition, there is accumulating evidence that restless legs syndrome (RLS) is another condition frequently reported by migraine patients (6). RLS is a common sleep-related movement disorder that—similar to migraine—predominates in women (7). RLS is characterized by an urge to move the legs, often accompanied by unpleasant leg sensations. Symptoms typically occur at night and during rest and resolve during movement (8). A common origin for migraine and RLS has been proposed (9) and a pathophysiological link involving a disturbance of iron and dopamine metabolism may exist (6,10,11).
Over the past years a number of studies have been published investigating the association between headaches, in particular migraine, and RLS in different populations (12–35). We therefore sought to summarize the current published evidence on RLS prevalence among migraine patients and the association between headaches, in particular migraine, and RLS by systematically reviewing the literature and performing a meta-analysis.
Subjects and methods
For this systematic review we followed the guidelines of the Meta-analysis of Observational Studies in Epidemiology (MOOSE) group for the design, performance, and reporting of meta-analyses of observational studies (36). We did not seek approval from an ethics committee since we used only data publicly available from the medical literature.
Data sources and searches
Two of the investigators (A.W., M.S.) independently searched PubMed, Embase, and Web of Science from their inceptions through January 2014. For their search the investigators combined text words and Medical Subject Headings (MESH) terms, if appropriate, for headache and migraine (“headache” or “headache disorders” or “migraine” or “migraine disorders”) with terms for restless legs syndrome (“restless legs syndrome” or “RLS”). They used the “explode” feature where applicable and restricted their search to humans. No language restrictions were applied. Additionally, the investigators manually searched the reference lists of all primary and review articles.
Study selection
A priori, we defined the following inclusion criteria for studies: First, we considered studies with a case-only (no control group), cross-sectional, case-control, or cohort design. Second, studies were required to investigate patients with migraine or headache or with RLS. Third, we considered only studies published after the publication of International Classification of Headache Disorders (ICHD)-I criteria for headache disorders (37) and the essential diagnostic criteria for RLS (38). Fourth, studies had to either provide prevalence estimates of RLS among migraine or headache patients or prevalence estimates of migraine or headache among RLS patients or relative effect estimates with 95% confidence intervals (CI) for the association of these conditions in the study populations.
For study selection two investigators (M.S., A.W.) jointly screened the titles and abstracts of all publications identified and excluded those not meeting any of the pre-specified criteria. The same investigators then evaluated the full articles of the remaining publications and also excluded any studies not meeting our inclusion criteria. Disagreements were resolved by consensus.
Data extraction
Two investigators (M.S., A.W.) independently extracted data from the studies identified and entered them into a database. Extracted data included the authors' names and title of the study, country of study origin, year of publication, study design, source population, study size, duration of follow-up if applicable, age and gender distribution of participants, criteria for diagnosing migraine/headache and RLS, temporal relationship between migraine/headache and RLS diagnosis, and use of migraine-specific drugs. For studies investigating RLS in migraine/headache patients we further extracted the number of individuals with and without migraine/headache, number of individuals with and without RLS among those with and without migraine/headache, and prevalence of RLS. For studies investigating migraine/headache among RLS patients we extracted the number of individuals with and without RLS, number of individuals with and without migraine/headache among those with and without RLS, and prevalence of migraine/headache. Further, we extracted the effect estimates with 95% CIs for the association between the two conditions. If effect estimates from various models were presented, we selected those derived from the model with the maximum amount of covariate acknowledgment. We did not contact study authors to obtain additional information.
Statistical analysis
To further investigate RLS prevalence, we calculated the percentage of RLS sufferers among migraine/headache patients and people without migraine/headache along with the 95% CIs if published data permitted to do so. For studies without a control group, we calculated only the percentage of RLS sufferers among migraine/headache patients. We then performed the DerSimonian and Laird Q test for heterogeneity among the study groups (migraine/headache patients, controls) and calculated the I 2 statistic (39). Because of high heterogeneity of RLS prevalence among the studies both in migraineurs and people without migraine (see Results section), we did not pool the prevalence data. We proceeded likewise to investigate the prevalence of headache/migraine in patients with RLS.
To further investigate the association between migraine/headache and RLS, we calculated the odds ratios (ORs) and 95% CIs for the association between migraine/headache and RLS in studies not providing relative effect estimates. We performed the DerSimonian and Laird Q test for heterogeneity and calculated the I 2 statistic (39). For meta-analysis we weighted the log of the ORs for each study by the inverse of their variance to obtain pooled estimates. We ran random-effects models, which include assumptions about potential differences between studies. Meta-regression was used to statistically evaluate the extent of heterogeneity due to country of study origin (Western populations vs. Asian populations vs. populations of heterogeneous ethnicities), study design (case-controls vs. cohort studies), gender, and migraine aura status. To visually examine the impact of individual studies on the overall homogeneity of the test statistic, we inspected Galbraith plots (40). Finally, to test for small study effects, e.g. due to publication bias, we used statistical methods described by Begg and Mazumdar (41) and Egger (42). Small study effects denote the tendency for smaller studies in meta-analysis to show larger effects.
A two-tailed p value<0.05 was considered statistically significant. All analyses were carried out using SAS v.9.2 (SAS Institute Inc, Cary, NC, USA) and STATA v.10.1 (Stata, College Station, TX, USA).
Results
Figure 1 summarizes the study selection process. The electronic search identified 752 references. After reviewing the titles and abstracts and excluding records not meeting our inclusion criteria, we were left with 27 records for further evaluation. We identified one additional record from electronic alerts for articles published online ahead of print (35). We evaluated these 28 records as full text references and excluded four that turned out to be conference abstracts not providing prevalence measures or measures of association between migraine/headache and RLS (43–46). This left us with 24 studies for our systematic review (12–35).
Summary of the study selection process.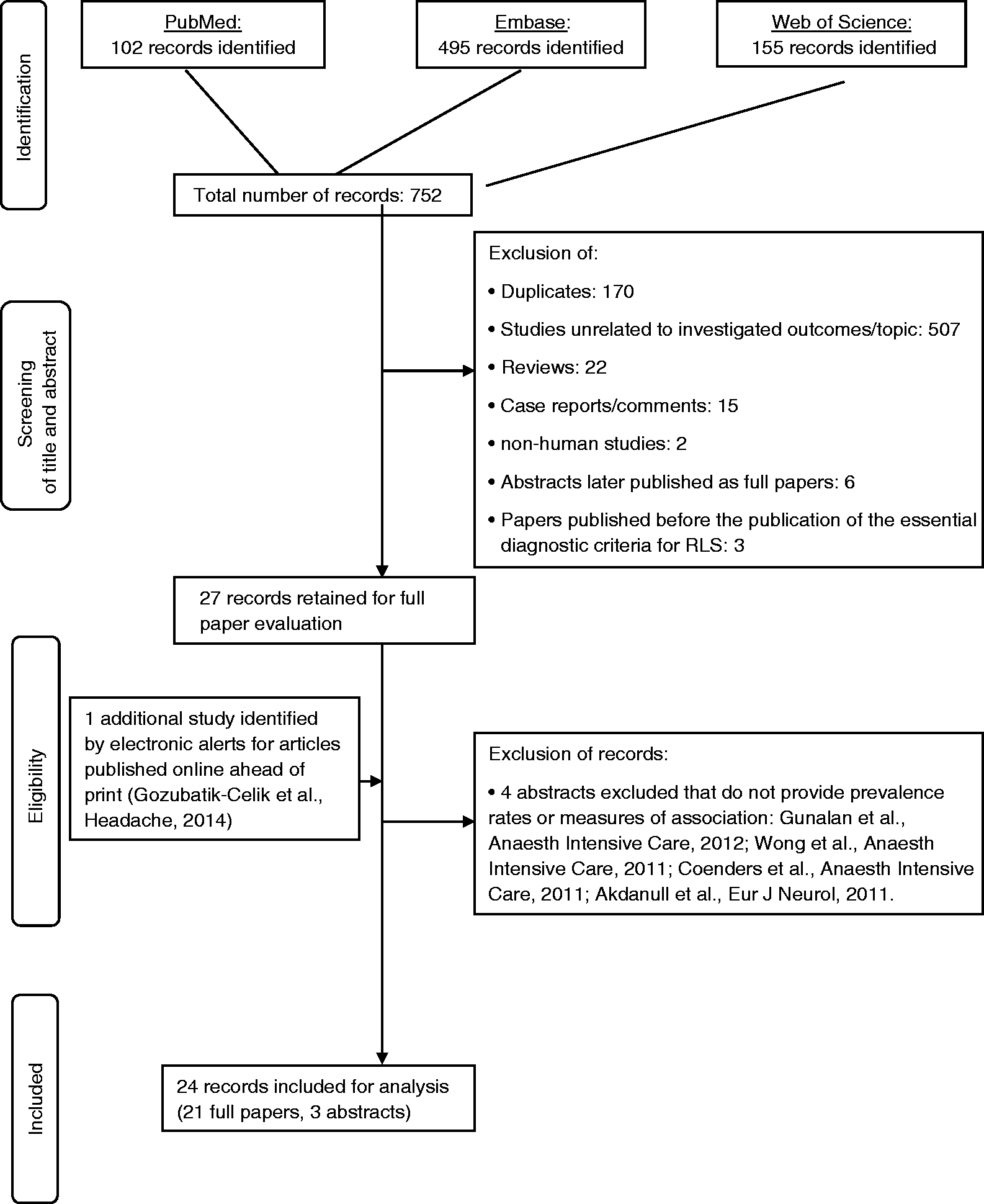
Study characteristics
Characteristics of studies investigating RLS in headache/migraine.

Characteristics of studies investigating headache/migraine in RLS.
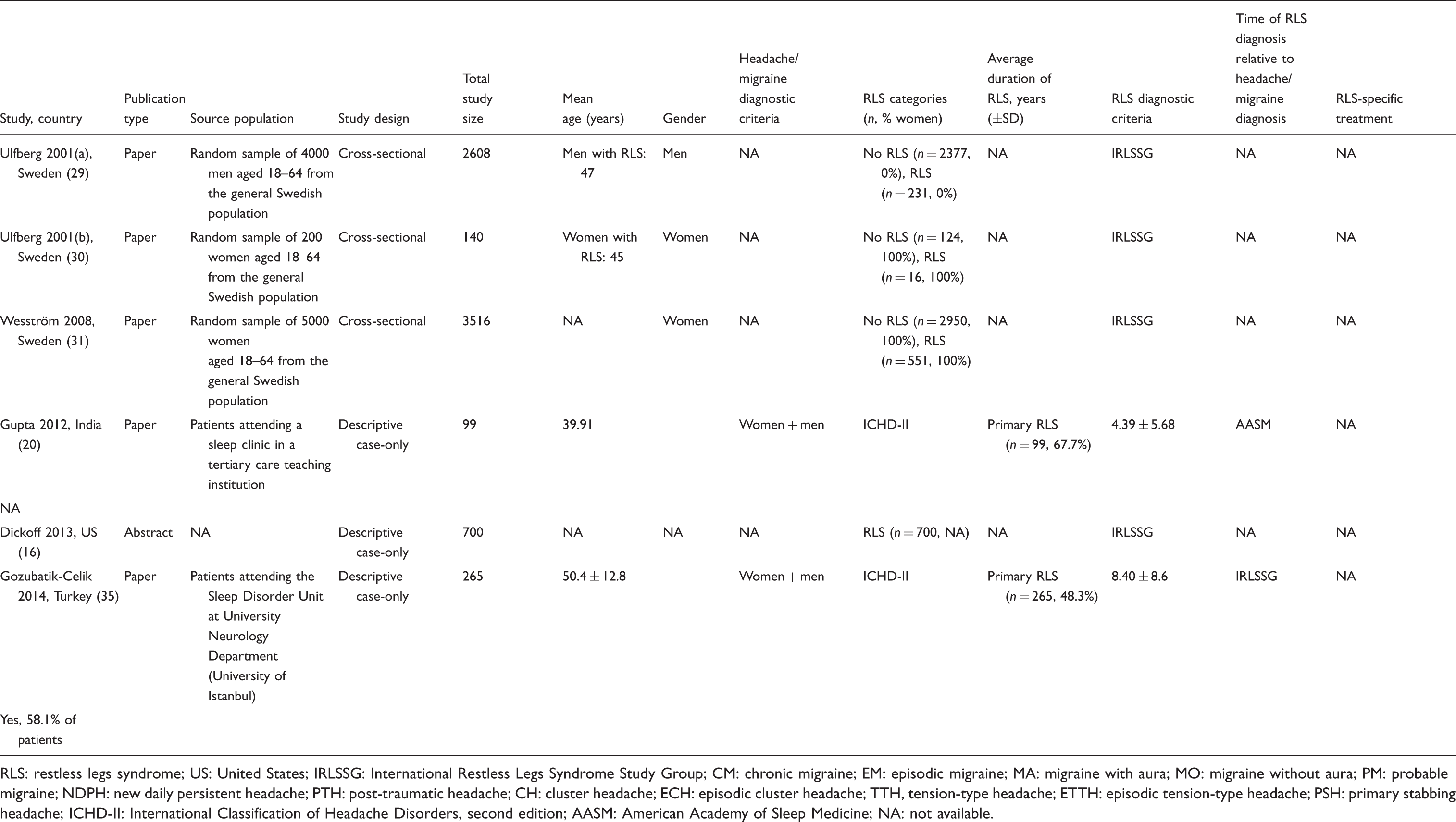
RLS: restless legs syndrome; US: United States; IRLSSG: International Restless Legs Syndrome Study Group; CM: chronic migraine; EM: episodic migraine; MA: migraine with aura; MO: migraine without aura; PM: probable migraine; NDPH: new daily persistent headache; PTH: post-traumatic headache; CH: cluster headache; ECH: episodic cluster headache; TTH, tension-type headache; ETTH: episodic tension-type headache; PSH: primary stabbing headache; ICHD-II: International Classification of Headache Disorders, second edition; AASM: American Academy of Sleep Medicine; NA: not available.
Eighteen studies reported on RLS among migraine/headache patients (12–15,17–19,21–28,32–34), among those 16 are full papers (12–14,17–19,22–28,32–34) and two are abstracts (15,21). One study was in a pediatric and adolescent population (27), while the other studies were in adults. Two studies had a cohort design (26,32) and eight studies each had a case-control (14,17,19,22–24,27,28) or descriptive case-only design (12,13,15,18,21,25,33,34). In 15 studies migraine patients were investigated (12,13,15,17–19,21–24,26–28,32,33), four studies reported on cluster headache (CH) patients (12,14,25,33), and five studies looked at mixed headache forms and other headache disorders (12,17,21,33,34).
Six studies reported on migraine/headache among patients with RLS (16,20,29–31,35); among those five are full papers (20,29–31,35) and one is an abstract (16). Three studies each had a cross-sectional (29–31) or a descriptive case-only design (16,20,35). Further, three studies each reported on migraine (16,20,35) or non-ICHD defined headaches (morning/daytime headaches) (29–31) among RLS patients.
Prevalence of RLS in migraine/headache
Prevalence of RLS among headache/migraine patients and controls and association between both conditions from individual studies.

Prevalence in percentage and 95% confidence intervals (CIs) were calculated based on the numbers of individuals with and without RLS among headache/migraine patients and controls as provided in the publications.
Odds ratios (ORs) and 95% CIs were extracted from the papers or calculated if the publications provided the numbers of individuals with and without RLS among headache/migraine patients and controls. RLS: restless legs syndrome; IRLSSG: International Restless Legs Syndrome Study Group; CM: chronic migraine; EM: episodic migraine; MA: migraine with aura; MO: migraine without aura; PM: probable migraine; NDPH: new daily persistent headache; PTH: post-traumatic headache; CH: cluster headache; ECH: episodic cluster headache; TTH: tension-type headache; ETTH: episodic tension-type headache; PSH: primary stabbing headache; NA: not available.
For any migraine the prevalence ranged from 8.7% (95% CI 7.7–9.7) (32) to 39.0% (95% CI 23.4–54.6) (33). The ranges among men (from 8.7%, 95% CI 7.7–9.7 (32) to 20.6%, 95% CI 6.3–34.9 (13)) and among women (from 11.8%, 95% CI 9.3–14.3 (12) to 26.9%, 95% CI 19.2–34.7 (13)) were largely overlapping. Likewise, the ranges for migraine with aura (from 8.3%, 95% CI 0.2–16.4 (12) to 33.3%, 95% CI 13.0–53.7 (21)) and migraine without aura (from 10.9%, 95% CI 7.1–14.6 (12) to 32.2%, 95% CI 22.4–42.1 (22)) were very similar.
The prevalence of RLS among patients with CH ranged from 0% (14,33) to 11.0% (95% CI 9.2–12.9) (25).
The two studies investigating patients with tension-type headache (TTH) reported a prevalence of 4.6% (95% CI 1.8–7.4) (12) and 5.0% (95% CI –5.5 to 15.5) (34).
Among controls of non-Asian populations 5.6% (95% CI 3.4–7.8) to 12.0% (95% CI 2.7–21.3) had RLS (14,17,19,23,24,26,27,32), compared with 1.8% (95% CI –0.3 to 3.9) to 5.6% (95% CI 0.7–10.4) among controls in Asian populations (22,28).
Heterogeneity was high among studies investigating RLS prevalence in patients with any migraine (I 2 = 92.8%; test for heterogeneity chi-square = 180.53, degree of freedom (df) = 13, p < 0.001), in CH (I 2 = 94.0%; test for heterogeneity chi-square = 16.71, df = 1, p < 0.001; two of the four studies were not included since none of the patients had RLS), and in controls (I 2 = 96.8%; test for heterogeneity chi-square = 284.3, df = 9, p < 0.001). Among studies looking at any migraine meta-regression did not indicate that country of study origin (Western (reference) vs. Asian (p = 0.82) vs. heterogeneous populations (p = 0.65)), study design (case only (reference) vs. case control (p = 0.98) vs. cohort (p = 0.15)), migraine aura status (p = 0.46) or gender (p = 0.26) account for significant heterogeneity across those studies. Likewise among studies reporting on RLS in controls meta-regression did not indicate that country of study origin (Western (reference) vs. Asian (p = 0.06) vs. heterogeneous populations (p = 0.94)) or design (p = 0.14) were significant sources of heterogeneity. Hence, we did not attempt to pool the data for any migraine, CH, and controls for meta-analysis.
Among the two studies investigating RLS prevalence in patients with TTH, there was no indication for heterogeneity (I 2 = 0.0%; test for heterogeneity chi-square = 0.01, df = 1, p = 0.94). Pooling the data indicated a prevalence of 4.6% (95% CI 1.9–7.3).
Prevalence of migraine/headache in RLS
Prevalence of migraine among RLS patients and controls and association between both conditions from individual studies.

Prevalence in percentage and 95% confidence intervals (CIs) were calculated based on the numbers of individuals with and without RLS among headache/migraine patients and controls as provided in the publications.
Odds ratios (ORs) and 95% CIs were extracted from the papers or calculated if the publications provided the numbers of individuals with and without RLS among headache/migraine patients and controls. RLS: restless legs syndrome; NA: not available.
Heterogeneity among the studies investigating migraine prevalence in RLS patients was high (I 2 = 99.3%; test for heterogeneity chi-square = 272.43, df = 2, p < 0.001), hence, we did not pool the data for meta-analysis.
Association between migraine/headache and RLS
A total of 10 studies reported on RLS among migraine/headache patients and controls (14,17,19,22–24,26–28,32). Among those effect estimates for the association between any migraine and RLS were available for eight studies (Table 2) (19,22–24,26–28,32). ORs (95% CIs) ranged from 1.20 (1.04–1.38) (32) to 8.50 (2.57–28.07) (28). One additional study investigated the association between headache and RLS, presenting an OR of 3.10 (95% CI 1.50–6.43) (17). One study among patients with CH did not allow calculating an effect estimate since none of the CH patients had RLS (14).
Heterogeneity was high among studies investigating the association between any migraine and RLS (I 2 = 88.8%; test for heterogeneity chi-square = 62.32, df = 7, p < 0.001). Meta-regression did not indicate that country of study origin (Western (reference) vs. Asian (p = 0.09) vs. heterogeneous populations (p = 0.55)), gender (p = 0.87) or migraine aura status (p = 0.66) account for significant heterogeneity among those studies. However, meta-regression suggested that study design (p < 0.001) was a significant source of heterogeneity among the studies. This agreed with visual inspection of the Galbraith plots, where studies with a case-control design (19,22–24,27,28) were located outside the margin set by two standard deviations of the z score. Hence, we did not attempt to pool the data from all studies for meta-analysis, but performed an analysis stratified by study design.
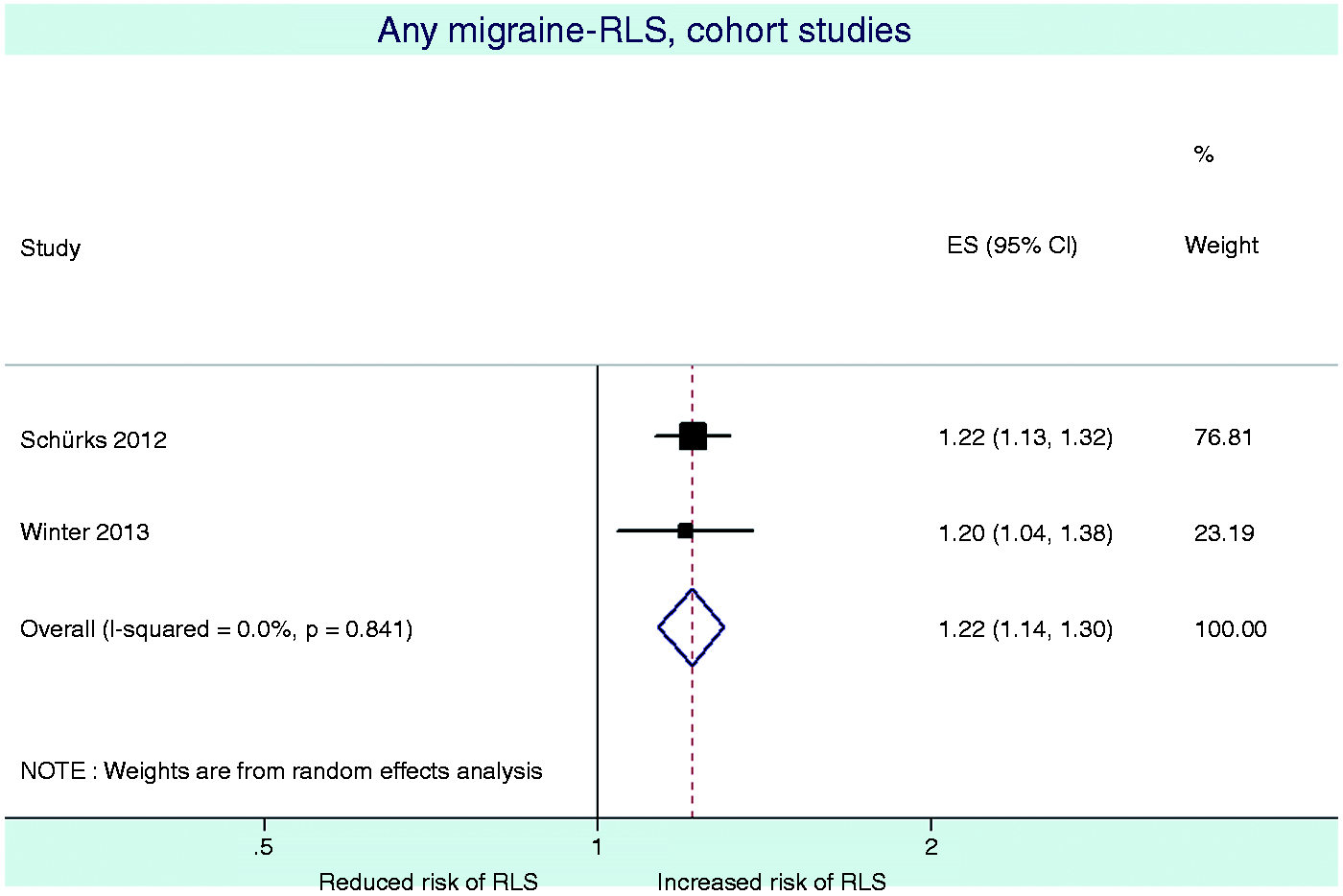
Results from the pooled analysis of case-control studies suggest that any migraine is associated with four-fold increased odds for RLS (pooled OR = 4.19, 95% CI 3.07–5.71), while pooled analysis of cohort studies suggest that the odds for RLS among migraineurs are increased by about 20% (pooled OR = 1.22, 95% CI 1.14–1.30) (Table 4, Figures 2 and 3). There was no remaining heterogeneity within the strata (case-control studies: I
2
= 0.0%, test for heterogeneity chi-square = 3.94, df = 5, p = 0.56; cohort studies: I
2
= 0.0%, test for heterogeneity chi-square = 0.04, df = 1, p = 0.84). There was no evidence for small study effects among case-control or cohort studies in formal investigations with Begg's and Egger's tests (Table 4).
Results from the case-control studies. Results from the cohort studies. Association between any migraine and RLS, heterogeneity, and small study effects. From random-effects model. RLS: restless legs syndrome; OR: odds ratio; df: degree of freedom; CI: confidence interval.

The three studies reporting on migraine in RLS patients did not have a control group, obviating calculating an effect estimate.
Discussion
Analyses from this systematic review suggest that RLS prevalence for any migraine ranges from 8.7% to 39.0%, with similar ranges for women and men as well as for migraine with aura and migraine without aura. Among controls of non-Asian populations 5.6% to 12.0% had RLS, compared with 1.8% to 5.6% among controls in Asian populations. Heterogeneity with respect to prevalence was high both among studies in patients with any migraine and controls. Prevalence of migraine in RLS ranges from 15.1% to 62.6%; heterogeneity was likewise high. Data regarding prevalence of RLS in CH and TTH as well as prevalence of migraine in RLS are limited. All published studies report increased odds for RLS among patients with any migraine. Heterogeneity among those studies was high and is attributable to study design. Among case-control studies pooled analysis indicates that any migraine is associated with four-fold increased odds for RLS, while pooled analysis of cohort studies suggest that the odds for RLS among migraineurs are increased by only about 20%.
There is plausibility for an association between migraine and RLS when considering pathophysiology and clinical findings. In both conditions disturbances of the iron and dopamine metabolism have been indicated. First, brain iron deposition has been reported in migraine patients and increased iron accumulation appears to be associated with repeated attacks (47). On the contrary, iron deficiency has been implicated in at least a subset of patients with RLS (48). Second, dopamine has long been hypothesized to be involved in migraine pathophysiology (10). In particular, premonitory symptoms like yawning, irritability, and mood changes as well as nausea and vomiting occurring both during the premonitory and headache phases may be caused by dopamine. Further, antiemetics with antidopaminergic properties are effective in aborting migraine attacks (49). These findings agree with experimental data from rats that dopamine can modulate neuronal firing in the trigeminocervical complex (50) and hence, modulate pain transmission in the brainstem. With regard to RLS pathophysiology, the most widely supported hypothesis relates to a dysfunction of the dopaminergic system of the A11 neurons descending from the hypothalamus to the spinal cord (11). A “dopaminergic link” between migraine and RLS is further supported by reports that migraineurs with RLS more often have premonitory symptoms than migraineurs without RLS (13).
Available data favor the scenario that RLS is a prevalent comorbidity in migraine and RLS is a condition that may substantially impair quality of life (51). However, for the following reasons, the burden of RLS imposed on migraine patients is still difficult to quantify. First, the reported RLS prevalence varies greatly among studies (Table 2), resulting in high heterogeneity. Our analyses do not indicate that country of study origin, study design, migraine aura status or gender significantly account for this heterogeneity. Second, many of the studies do not have a control group, and among studies with control groups heterogeneity in the control groups was likewise high (Table 2). This could not be explained to a significant degree by design and country of study origin. The observed prevalence range among non-Asian control populations of 5.6% to 12.0% was within the range of 4%–29% reported in a recent systematic review (7). The prevalence range of 1.8%–5.6% among Asian controls was lower than among the non-Asian controls, which agrees with the published literature (52); however, interpretation warrants caution because of the low number of studies. Hence there are remaining uncertainties with respect to RLS prevalence among migraineurs.
The findings among controls argue that the wide range in RLS prevalence among patients with any migraine cannot be ascribed to migraine per se. A potential source of variability is frequency and severity of RLS symptoms used to aid RLS diagnosis. However, only four studies reported some form of International Restless Legs Syndrome Study Group (IRLSSG) scores (Table 1). Hence, too few studies are available that could be sensibly grouped into categories to be used in a meta-regression approach. Additional factors such as genetics and environmental factors also likely account for the variability of RLS prevalence. This is supported by reports that the risk for RLS increases with multimorbidity, i.e. appears to be a function cumulative disease burden (53).
High heterogeneity among the studies with respect to the effect estimates was completely explained by study design. Specifically studies with a case-control design suggested four-fold increased odds of RLS for any migraine, while among cohort studies there were only 20% increased odds, with no remaining heterogeneity. Hence, when interpreting our results, the following aspects need to be considered.
First, despite the established criteria by the International Headache Society (54) migraine is still clinically very heterogeneous. Hence, migraineurs presenting to headache or neurology clinics, where cases for the case-control studies were recruited, are likely more seriously affected by their migraines than migraineurs identified in non-clinic cohort studies. If we further hypothesize that migraine severity is correlated with comorbidity including RLS, it is plausible that the odds for RLS are higher in case-control than cohort studies. This may be supported by data from one cohort study, suggesting that active migraine at the time of the study is associated with RLS, while such an association was no longer statistically significant for prior migraine, i.e. for women no longer reporting active migraine at the time of the study (26). However, data on migraine attack frequency, an important marker for migraine severity, were not available in this study.
Second, patients and controls in case-control studies were asked about their migraines and RLS without taking the temporal association between the two conditions into consideration, while the cohort studies were designed to investigate only RLS among participants who had reported migraine previously. Hence, the effect estimates reported in case-control studies are more likely to reflect the overall risk of having the two conditions together (not necessarily at the same time or in a certain sequence), while the cohort studies estimate the future risk of RLS among migraineurs. In both types of study designs RLS was ascertained at only one point in time obviating analyses of changing time patterns of RLS manifestation.
Third, the impact of potential confounders on the association between migraine and RLS was differentially captured among studies. While some of the case-control studies were matched by age and sex (17,19,22–24,28), which are established risk factors both for migraine and RLS, a number of case-control studies do not report if covariate acknowledgment was taken into account. In contrast the cohort studies additionally accounted for many covariates that may be associated with migraine and/or RLS and as such affect the respective other condition, including for example cardiovascular risk factors, alcohol consumption, depression, and Parkinson's disease (26,32).
Finally, use of migraine-preventive drugs may affect RLS prevalence among migraineurs; however, available data did not permit us to investigate this.
Our analyses support the role of RLS as an important comorbidity in migraine and an association between both conditions. The degree of association may be determined by severity of migraine. In addition, defining the temporal sequence for the occurrence of migraine and RLS as well as taking changing time patterns for both conditions into consideration might impact their association. The available data, although scarce, do not support a potential modifying effect by gender and migraine aura status. Further, a potential association between RLS and other primary headache disorders like CH and TTH needs to be further investigated. Given the high prevalence and burden of both headache disorders and RLS in the general population, future studies addressing these unresolved questions are of great individual and public health importance.
Clinical implications
Migraine and restless legs syndrome (RLS) are common neurological conditions in clinical practice. RLS is an important comorbidity of migraine. The propensity of having RLS appears to be higher among patients in a clinic-based setting compared to migraineurs from the general population. Patients presenting with either migraine or RLS should also be questioned about the respective other conditions, since this may have implications for treatment strategy.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
We present full disclosures for all authors. None of the disclosures for any of the authors represent a conflict of interest with regard to this specific manuscript.
Dr Schürks is a full-time employee of Bayer HealthCare Germany.
Dr Winter is currently supported by funds from Washington University School of Medicine, the Barnes-Jewish Hospital Foundation, and Siteman Cancer Center.
Dr Berger has received research support for the conduction of the DMKG Headache Study; unrestricted grants of equal share from the German Migraine and Headache Society and a consortium formed by Allmiral, Astra-Zeneca, Berlin-Chemie, Boehringer Ingelheim Pharma, Boots Healthcare, GlaxoSmithKline, Janssen Cilag, McNeil Pharmaceuticals, MSD Sharp & Dohme, Pfizer; for the “Course of Restless Legs Syndrome Study”; unrestricted grants from the German Restless Legs Society and a consortium formed by Boehringer Ingelheim Pharma, Mundipharma Research, Neurobiotec, UCB (Schwarz Pharma) and Roche Pharma; from the German Ministry of Research and Education for several research projects within the German Competence Net Stroke and an ongoing cohort study on depression and subclinical arteriosclerosis.
Dr Kurth has received within the last two years investigator-initiated research funding from the French National Research Agency and the US National Institutes of Health. Further, he has received honoraria from BMJ and Cephalalgia for editorial services.