
Abstract
Aim
To evaluate the diagnostic accuracy of the SNNOOP10 list in the detection of high-risk headaches.
Methods
Patients that visited the Hospital Clínico San Carlos (Madrid) emergency department due to headache that were allocated to a Manchester Triage System level between critical and urgent were prospectively included but retrospectively analysed. A researcher blind to the patients’ diagnosis administered a standardised questionnaire and afterwards a neurologist blind to the questionnaire results diagnosed the patient according to the International Classification of Headache Disorders. The primary endpoint was to assess the sensitivity of the SNNOOP10 list in the detection of high-risk headaches. Secondary endpoints included the evaluation of the sensitivity, specificity, positive predictive value, negative predictive value and area under the curve of each SNNOOP10 item.
Results
Between April 2015 and October 2021, 100 patients were included. Patients were 44 years old (inter-quartile range: 33.6–64.7) and 57% were female. We identified 37 different diagnoses. Final diagnosis was a primary headache in 33%, secondary headache in 65% and cranial neuralgia in 2%. There were 46 patients that were considered as having high-risk headache. Patients from the primary headache group were younger and more frequently female. Sensitivity of SNNOOP10 list was 100% (95% confidence interval: 90.2%–100%). The items with higher sensitivity were neurologic deficit or disfunction (75.5%), pattern change or recent onset of the headache (64.4%), onset after 50 years (64.4%). The most specific items were posttraumatic onset of headache (94.5%), neoplasm in history (89.1%) and systemic symptoms (89%). The area under the curve of the SNNOOP10 list was 0.66 (95% CI: 0.55–0.76).
Conclusion
The red flags from the SNNOOP10 list showed a 100% sensitivity in the detection of high-risk headache disorders.
Keywords
Introduction
Headache disorders are among the most frequent and prevalent neurological diseases (1). Headache is also one of the most common reasons for seeking care at an emergency department (ED) in the United States (US) (2), being consistently the fourth to fifth reason for consult globally (3,4). The main priority in the ED is detecting those patients that might have a life-threatening cause of headache (5), a proportion that varies between 2% and 18% (6–11) depending on the studies. Mortality due to some of causes of secondary headache, such as subarachnoid haemorrhage, intracerebral haemorrhage or bacterial meningitis varies from 12% to 50% (12–14), and the prognosis might be highly influenced by the accuracy of diagnosis and timely treatment (15).
Diagnosis of secondary headache disorders is based on the presence of red flags, which are intended to reduce wasted and unnecessary referrals, through better stratification of patients (16,17). There are several proposals, most of them based on consensus of experts, with limited prospective validation (18–21). In 2019, the Secondary Headache Special Interest Group of the International Headache Society compiled the main red flags under the acronym “SNNOOP10” (22). To date, these criteria have not been validated. The aim of this study was to evaluate if secondary headache disorders can be correctly identified by using the SNNOOP10 list (22) in a cohort of patients that visited the ED with headache complaints and had high probability of secondary headache.
Methods
This was an observational analytic study with prospective cohort design. The study was done according to the standards for reporting of diagnostic accuracy studies (STARD) guidelines (23). The study population consisted of patients visiting the ED of the Hospital Clínico San Carlos de Madrid, Spain, a third-level, academic, public hospital, partly covering the metropolitan area of Madrid, with a population of 375,000 covered in this area. Recruitment was done between 20 April 2015 and 20 October 2016.
Eligibility criteria
The inclusion criteria were: 1) patients visiting the ED because of headache or if headache was one of the main symptoms at that time; 2) patients not being directly admitted to the critical box of the ED; 3) patients allocated to a Manchester Triage System (MTS) (11) level between 1-“critical” and 3-“urgent”; 4) patients older than 18 years old. Patients were excluded if 1) the primary reasons to consult were skull or cervical trauma; 2) that were unable to precisely describe the characteristics of the headache because of disorders of consciousness, speech disorders or cognitive impairment; 3) that had already participated in the study.
Recruitment and sampling
Sampling method was by probabilistic sampling, all the potential patients that came in during the shifts of the research team were screened. Each researcher worked approximately four shifts per month, for a total of 96 shifts. Based on a prior study conducted in the same hospital, the number of patients with an MTS score between 1–3 in a six-month period was 175, accounting for almost a patient per day (11). Every time that a patient visited the ED because of headache and had an MTS score between 1–3, the ED nurses alerted the research team who recruited the patient.
Index test
The research team was divided in two sections. The first group of researchers included four physicians, that approached the patients during their ED stay. They explained the purpose of the study and invited him/her to participate. If the participant agreed, they administered a standardised questionnaire that included a list of red flags, covering the 15 items from the SNNOOP10 list (22), and clarified the meaning of each specific red flag, if necessary.
The SNNOOP10 list is a proposal from the secondary headache special interest group of the International Headache Society which summarises the 15 main red flags, based on a literature review and expert opinion. The full SNNOOP10 list is available in the online Supplementary Table 1. At the time we analysed the results of our study, it had not yet been validated (22). Since the study was done prior to the publication of the SNNOOP10 list (2019), the original study questionnaire prospectively assessed 28 different red flags, however, for the purpose of the present study, we will just retrospectively analyse the 15 variables that are included in the SNNOOP10 list. The researchers were completely blind to the clinical information and were not allowed to ask anything beyond what was listed in the questionnaire. Furthermore, the outcome of the questionnaire was not shown to the evaluating neurologist and did therefore not alter the clinical evaluation and care of each patient.
Reference test
Afterwards, the second group, formed by two neurologists DGA and NGG with specific interest in headache disorders, reviewed the discharge report and the medical file of the patient. Then all patients were invited to a three-month follow-up either by in-person consultation or by phone. If needed, additional imaging, blood tests or other tests were conducted. The patients were classified by using the ICHD-3 beta (24), and once published, according to ICHD-3 criteria (25). Additionally, patients were classified as having high-risk headaches (HRH) if the cause of the headache: a) could threaten the patient’s life (e.g., central nervous system infections, subarachnoid haemorrhage); b) could cause significant morbidity, either persistent (e.g., vision loss) or paroxysmal (e.g., seizures); or c) could mimic a condition fulfilling criteria for a or b (e.g., first episode of hemiplegic migraine or thunderclap headache). The patients’ classification as having HRH was done by the two neurologists ALG and JPE, based on all the available information, the results of the investigations and the three-month follow-up evaluation, which was in-person when they deemed it necessary. Both neurologists were completely blind to the results of the questionnaire. Figure 1 summarises the study design.

Study design summary. Created with BioRender.com.
Studied variables
Besides the presence of SNNOOP10 items, we analysed demographic and clinical variables. The first were sex, age, country of birthplace; and the clinical variables included headache intensity, presence of photophobia, phonophobia, osmophobia, nausea, vomiting, and aggravation by physical activity.
Ethics
The study was approved by the local ethics committee board (CP14/425-E). All participants were informed about the study, agreed to participate and signed informed consent form. The study was done in accordance with the Declaration of Helsinki principles (26).
Study endpoints
The primary endpoint was to evaluate the sensitivity of the SNNOOP10 list in the detection of high-risk headaches (HRH) in a series of patients that visited the ED because of headache and had high risk of secondary headache (MTS score 1–3).
As secondary endpoints, we analysed the diagnostic accuracy of each SNNOOP10 item, including sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, negative likelihood ratio and area under the curve (AUC) in receiver operating characteristic model (ROC). We also compared the frequency and type of SNNOOP10 items between the main groups of the ICHD, primary headache disorders, secondary headaches and neuralgias, and patients with and without HRH.
Statistics
Qualitative data was presented as frequencies and percentages, with 95% confidence interval (95% CI). In the description of qualitative data, the selected measures of central tendency were mean if the distribution was normal and median if not. Measures of dispersion were range (R) and standard deviation (SD) or inter-quartile range (IQR) depending on the distribution. In the contrast of hypothesis, Chi-squared test was used to compare qualitative variables and if the number of subjects per group was <30, then Fisher exact test was employed. To compare between qualitative and quantitative variables, Student t-test or Mann-Whitney U-test were used, and if qualitative variable had more than two categories, then ANOVA was used. We estimated the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (PLR), and negative likelihood ratio (NLR). We created a logistic regression model with all the variables and a multivariate model that included all the variables with a p-value of 0.3 or less. We calculated area under the curve by receiver operating characteristic curves and represented them graphically. Statistical signification threshold was set in 0.05 and multiple comparisons were managed by exact test and multivariate modelling. Sample size was not estimated in advance. Missing data was managed by complete-case analysis. Statistical analysis was conducted using the Statistical Package for Social Sciences version 26.0 software (SPSS, Inc., Chicago, IL, USA).
Data availability statement
The full datasets are available to other authors upon request to the corresponding author.
Results
During the study period, 100 patients fulfilled eligibility criteria, aged 44 years median (IQR: 33.6–64.7), 57% were women. The final diagnosis was primary headache in 33 cases (33%), secondary headache in 65 (65%) and cranial neuralgia in 2 (2%). Among the secondary headache patients, 46 (46%) had an HRH. Supplementary Figure 1 shows the frequency of diagnosis according to the ICHD-3 group. The total number of diagnosis was 37. There were 45 patients that were classified as high-risk headache. Supplementary Table 2 shows the frequency of specific diagnosis coded by ICHD-3 and the high-risk specific diagnoses.
Patients from the primary headache group were younger and more frequently female (67 vs. 51%) than patients with secondary headache. Hypersensitivity to stimuli was more frequent in primary headache group. Table 1 compares demographic and clinical variables between the primary and secondary headache groups. Patients with HRH were older and had less frequent hypersensitivity to stimuli. Table 1 compares demographic and clinical variables between standard headache and high-risk headaches.
Demographic and clinical variables comparison between the main categories of the ICHD and between non-high risk and high-risk headache patients. The neuralgia group was omitted in the statistical comparison between primary and secondary headache patients.

†Fisher exact test. ‡ANOVA.
Sensitivity of SNNOOP10 list
All the patients included in the study had at least one positive SNNOOP10 item. The sensitivity of the SNNOOP10 list for HRH detection was 100% (95% CI: 90.2–100%). The mean frequency of SNNOOP10 items in the primary headache patients was 3.75 (1.7), being minimum 1 and maximum 7; in the secondary headache group the mean was 4.7 (1.6), range 1–8; and both patients of the neuralgia group had four positive items. The number of positive SNNOOP10 items in the secondary group was significantly higher than in the primary headache group (p = 0.008).
Frequency and type of SNNOOP10 items in the ICHD groups
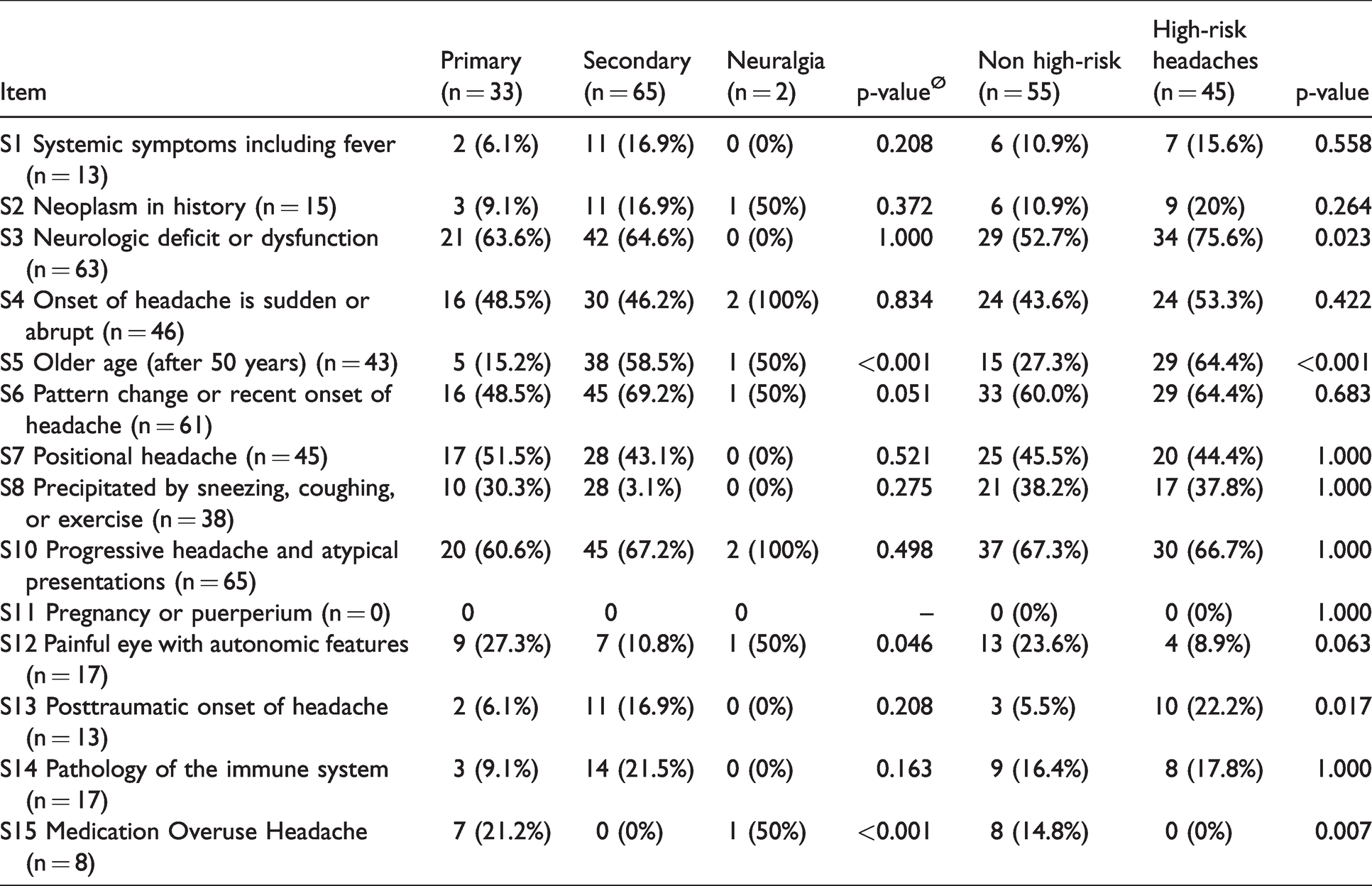
Frequency of SNNOOP10 items 5 (older age) and 6 (pattern change) were more frequent in the secondary headache group. Ocular pain, trigeminal autonomic features and medication overuse headache were more frequent in the primary headache group. Table 2 shows the frequency of SNNOOP10 items in primary headache disorders, secondary headache patients and cranial neuropathies.
Frequency of SNNOOP10 items in the main categories of the ICHD and between patients with and without high-risk headaches. The neuralgia group was omitted in the statistical comparison between primary and secondary groups.
Frequency and type of SNNOOP10 items in the HRH group
All the participants from the HRH group had at least one positive item in the SNNOOP10 list, having a minimum of 2 and maximum of 8 items. On the other hand, in the standard group, all patients had at least one positive item, as well, the minimum being 1 and the maximum 8. The mean number of positive SNNOOP10 items in the standard group was 4.0 (1.8), compared with 4.9 (1.4) in the HRH group (p = 0.009). Frequency of items 3 (neurological deficit), 5 (older age), and 13 (posttraumatic onset) was higher in the HRH group. Supplementary Table 3 shows the frequency of each SNNOOP10 item between the standard group and the high-risk headache group.
Presence of SNNOOP10 items in the ICHD-3 groups
The group with a higher mean number of items was cranial autonomic cephalalgias, and the lower number was tension-type headache group. Supplementary Figure 2 shows the mean number of SNNOOP10 items per ICHD-3 group. Table 2 shows the frequency of each SNNOOP10 item per ICHD-3 group.
Diagnostic accuracy of the SNNOOP10 items
In the detection of HRH, the most sensitive items were neurologic deficit or dysfunction, progressive headache, change in the pattern and older age. The most specific items were posttraumatic onset, immune-compromised state, history of cancer, and systemic symptoms. Table 3 shows the sensitivity (S), specificity (E), positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (PLR), negative likelihood ratio (NLR) of each SNNOOP10 item. The item with the higher AUC was number 5, age of onset >50 years, with AUC: 0.67. Most of the items were close to AUC: 0.5. Figure 2 shows the receiver operating characteristic curves of each of the different SNNOOP10 items. Table 4 depicts the values of the area under the curve in the receiver operating characteristic model. The combination of all the SNNOOP10 variables showed an area under the curve of 0.66 (95% CI: 0.55–0.76), with a standard error of 0.054 (p = 0.006), showed in Figure 3.
Diagnostic accuracy of SNNOOP10 items.

NLR: Negative Likelihood ratio; NPV: Negative Predictive Value; PLR: Positive Likelihood Ratio; PPV: Positive Predictive Value; Se: Sensitivity; Sp: Specificity.

Receiver Operating Characteristics Curve of each SNNOOP10 item.
Area under the curve of each SNNOOP10 item.


Receiver Operator Characteristics Curve of the pooled SNNOOP10 list.
Determinants of high-risk headaches
The items that significantly showed association with HRH were older age, posttraumatic onset, neurologic deficit or disfunction, and neoplasm in history. Painful eye and cranial autonomic symptoms had a lower odd of associating HRH. Supplementary Table 4 shows univariate logistic regression model of SNNOOP10 items in the prediction of high-risk headache. In the multivariate analysis, only older age and neurologic deficit remained statistically significant (Table 5).
Multivariate logistic regression model of SNNOOP10 items in the determination of high-risk headache.

Discussion
In this study, we tested if high-risk headaches were adequately detected by using the SNNOOP10 red and orange flag list in patients with high probability of having a secondary headache disorder. For this purpose, a series of patients were evaluated during their ED stay and prospectively followed-up afterwards by neurologists with expertise on headache medicine. The main findings of this study are that all the patients that visited the ED because of headache and a high-risk headache, were detected by using the SNNOOP10 list. The sensitivity of the combination of all the red and orange SNNOOP10 flags was 100%. However, most of the red flags also showed a low specificity. Still, diagnostic tests owing to detect a potentially life-threatening condition must be more sensitive than specific (27,28), and this study shows the challenges of diagnosing headache patients based on the history of the patients alone. In order to evaluate sensitivity, we selected patients based on the presence of some red flags after being evaluated in the ED triage area. This could represent a selection bias, as the frequency of secondary headache patients was 65%, much higher than the 2–18% described in other studies that evaluated the general epidemiology of headache in the ED (6–10,29). This could influence the positive predictive value and negative predictive value, yet specificity seemed equally low. The potential reasons for the low specificity of the items are diverse. First, the number of secondary headache disorders is profuse. ICHD-3 lists 118 different secondary causes of headache (25). Second, the same red flag might lead to many different causes of headache. A systematic review found 119 different causes of thunderclap headache published in literature up to 2014 (30). Third, a single disorder can present with different phenotypes. In the case of Cerebral Venous Sinus Thrombosis (CVST), headache is not constant, as 12% of the patients do not experience it over the course of the disease (31–33), whereas in 22-45% of the cases, it is the only neurological symptom (34,35).
Not every secondary headache disorder is equally menacing (36,37). In the present study we focused on high-risk headaches, a group which also include some primary headache disorders that might mimic a secondary cause. These patients should be managed as a potential secondary headache sufferers, and only an after appropriate study, these headaches can be classified as primary headache disorders, such as primary thunderclap headache or atypical aura (25). In the present study we tested the sensitivity of the SNNOOP10 list in a selected population with a higher probability of having a secondary headache. The higher the sensitivity, the higher the negative predictive value. However, future studies should also evaluate the specificity of the different red flags, to see its applicability in epidemiological studies and other settings.
In this study we observed that the systematic use of red and orange flags adequately detected all patients with secondary headache and HRH patients. The implementation of red flag lists might be facilitated by the use of abbreviated proposal, as the SNNOOP10 criteria (22). In the case of other standardised triage systems, such as Andorran-Spanish triage system and Manchester Triage System (37), the degree of expertise of the nurse influenced the assigned classification, due to the need of a basic neurological examination, including the assessment of meningeal irritation signs.
Studies analysing the true diagnostic accuracy of diagnostic items, such as the SNNOOP10 list, should anticipate all these factors. In our study, we found 37 different diagnoses among 100 patients. Second, frequency of secondary diagnosis per each different SNNOOP10 criterion might be highly variable. Studies that analysed frequency of subarachnoid hemorrhage (SAH) in all the patients with thunderclap onset of the headache vary between 6.2% and 17% (38–40). Therefore, the sample size estimation must anticipate a high number of different secondary headache disorders, so the needed sample could be remarkable to ensure that the primary endpoint can be completed. Other red flag validation studies have included up to 589 patients (29). Our study was clearly underpowered for many of the secondary endpoints, as comparing the frequency of red flags within the different categories, being many of the analyses not statistically significant. Each study should be designed to answer a single question and in all the exploratory variables, the absence of evidence is not evidence of absence (41).
In our sample, most of the items from SNNOOP10 list seemed to be more frequent in the secondary or HRH groups, however in some cases, such as pattern change, progressive worsening or precipitation by sneezing, frequency seems to be equal. Diagnosis of headache is still based on history and examination (42), and some patients might not fully understand some questions or misinterpret them. The main reasons for visiting the ED because of headache are usually intensity, treatment resistance and fear about having a severe condition (43).
In line with that, many primary headache patients might have atypical characteristics, or even red flags (44,45), in particular in the ED setting (46). Migraine headache might present with transient neurological symptoms (47), sudden onset (48), onset after 50 years (49), change on the pattern (43), worsening by sneezing, coughing or exercising (45), cranial autonomic symptoms (50). However, by definition, primary headache disorder diagnosis can be done only once the headache is not better accounted for by any other headache disorder (25). In the case of primary headaches, the use of red flags may be complemented by the evaluation of green flags, defined as signs or verbal cues pointing towards a primary headache diagnosis. Recently, a list of five green flags was proposed, with some of these may be particularly relevant in the ED setting, as the onset of the headache during childhood, the presence of close family members with the same headache phenotype and the cessation of the headache more than one-week ago (51). Nonetheless, the presence of any red or orange flag, obligates the clinician to rule out a secondary headache. To complete the equation, further studies should evaluate the negative predictive value of the SNNOOP10 list should in non-selected samples.
The present study has several flaws. First, it is a single centre study, so the studied population might not be representative of other settings. Spanish healthcare system is public and subsidised by government, which could affect the profile of patients that seek attention in the ED, however, access to medical attention is free and patients do not need to be referred from primary care. Second, the sample size is limited. We did not calculate sample size in advance and given the vast number of different secondary and high-risk headache disorders, to have a representative number of different entities, the number of included patients should ensure a sufficient proportion of each of the main secondary headache disorders, based on their prevalence in the ED and the desired precision or margin of error, which should be calculated based on the specific study primary endpoint. Third, the study was designed to evaluate the sensitivity of the SNNOOP10 list in the detection of patients with HRH, so most of the secondary endpoints should be interpreted cautiously, including the frequency of red flags in patients with primary headaches and the PPV and NPV, which could be affected by the prevalence of secondary headaches in the sample. Fourth, validation of SNNOOP10 list was not done and items were verbally administered, which may decrease but do not exclude the possibility of misinterpretation, future studies may validate it when administered in paper or digitally. Some causes of secondary headache were underrepresented due to the eligibility criteria, which excluded patients with cranial or cervical trauma and patients with altered level of consciousness, altered mental status or speech disorders. Given our study design, only patients that visited the ED during the shifts of the research team were evaluated for eligibility, however, shifts occurred in a random basis, which could minimise the risk of selection bias.
Based on the present findings, we suggest that future studies should investigate the relative weight of each red flag, if all of them are equally valid or some of them should be re-considered. It should be evaluated if the red flags lists can be self-administered by patients, even at home. Finally, a prospective study with two arms could be done in order to compare if the use of SNNOOP10 list impacts the prognosis of patients and modifies endpoints associated with ED management of patients, in terms of number of imaging studies done, percentage of diagnosed patients, ED stay duration and percentage of neurology consults.
Conclusion
In our sample, the SNNOOP10 list showed a 100% sensitivity in the detection of high-risk headaches in patients seeking for medical attention in the emergency department due to headache. The vast number of causes of secondary headache, and the absence of items with perfect sensitivity and specificity suggests that the SNNOOP10 list should be further validated and implemented in clinical practice by the combination of all its items.
Clinical implications
Headache is a leading reason for presenting to the emergency department. Detection of severe causes is based on red flags, which are insufficiently studied. We evaluated for the first time the SNNOOP10 list, a proposal from the Secondary Headache Special Interest Group of the International Headache Society. All patients with a serious cause of headache had at least one ref flag included in the SNNOOP10 list, suggesting its potential usefulness. Until the development of headache-specific biomarkers, detection of high-risk headaches can be done by the evaluation of red flags, being the SNNOOP10 list a possible approach with high sensitivity.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024221120249 - Supplemental material for Sensitivity of the SNNOOP10 list in the high-risk secondary headache detection
Supplemental material, sj-pdf-1-cep-10.1177_03331024221120249 for Sensitivity of the SNNOOP10 list in the high-risk secondary headache detection by David García-Azorín, Jaime Abelaira-Freire, Nuria González-García, Esther Rodriguez-Adrada, Henrik Winther Schytz, Mads Barloese, Ángel Luis Guerrero, Jesús Porta-Etessam and Francisco Javier Martín-Sánchez in Cephalalgia
Footnotes
Acknowledgements
The authors thank the Emergency Department crew for their great support in the study. The statistical analysis was conducted by DGA.
Data Availability Statement
All data obtained and/or analysed are available from the authors upon reasonable request.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DGA, HWS are members of the Secondary Headache Special Interest Group of the International Headache Society. Authors declare no other conflicts of interest or disclosures relevant to the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.