
Abstract
Objective
There is a lack of data on the burden of primary headache disorders such as migraine on emergency services. Existing data relies on a coding of “headache”, which encompasses both primary and secondary headache of all causes; for example, subarachnoid haemorrhage. Guy’s and St Thomas’ NHS Trust in London is one of the UK’s busiest emergency departments with 150,000 attendances per year. Our aim was to assess the healthcare resource utilisation of primary headaches, in particular migraine, in acute medical services.
Methods
We conducted an audit of all adult presentations to the emergency department of Guy’s and St Thomas’ Hospitals which were coded as “headache” over the first 6 months of 2018. We reviewed the initial diagnosis at presentation and also at discharge, investigations and outcome.
Results
Of 78,273 attendances to the emergency department, there were 976 presentations to the emergency department with “headache” as their primary complaint. “Migraine” was the most frequent of all diagnoses, accounting for 30% of all headache presentations and 25% of headache admissions. We calculated the cost of admitting and investigating migraine as £131,250 over the 6-month period.
Conclusion
Emergency admissions for migraine represent an avoidable cost and burden for both the hospital and the migraineur. This data informs us about the need to develop better care pathways for migraine in the community and to improve headache education for physicians and patients.
Introduction
Headache accounts for 1–4% (1) of presentations to the emergency room, with one American study showing one third of these are due to migraine (2). Although the primary aim of the emergency physician assessing the headache patient is to diagnose or exclude secondary headaches such as subarachnoid haemorrhage or meningitis, they are increasingly required to provide symptomatic relief for patients with primary headaches syndromes, mainly migraine, who attend emergency departments for acute treatment.
Digital data from the national health service (NHS) of England shows the number of admissions to hospitals in England for “headache” (including migraine) has increased by 14% over the last five years, to 108,711 emergency admissions in 2018/19 (3). Emergency admissions to hospital for headache in adults account for a third of all neurological admissions (3). However, since the coding of “headache” covers all causes and does not distinguish between primary and secondary causes, it is not currently known what proportion of these are due to primary headache disorders such as migraine.
Guy’s and St Thomas’ NHS Trust (GSTT) in London is one of the UK’s busiest accident and emergency services with 150,000 attendances per year. It is a teaching hospital with a headache service. We aim to assess the burden of primary headaches, in particular migraine, looking specifically at the number of patients attending the emergency department, the number admitted, and the investigations performed to determine the financial and resource cost to the acute and emergency medical services of our hospital during a 6-month period. We aim to use this information to enable us to redirect resources to more appropriate pathways and avoid unnecessary, often invasive investigations. We hope these findings will enable us to improve the management for patients with primary headache disorders.
Methods
Study design
This was an observational analytic study with a retrospective audit of all consecutive adult patients attending the emergency department (ED) at St Thomas’s Hospital (Guy’s and St Thomas’ NHS Trust) during a 6-month period in 2018. The audit was approved by Guy’s and St Thomas’ NHS Trust.
Eligibility criteria
All consecutive patients aged 16 years and over attending the emergency department (both those presenting themselves and those arriving by ambulance), who were coded as having a presenting complaint of “headache” during the period 1 January 2018 to 30 June 2018, were taken into account including patients with cranial neuralgias. We excluded patients with insufficient data.
Patients presenting with traumatic head injury were only included if their primary presenting complaint was of “headache” rather than “head injury”, thereby excluding many of the head injury presentations to the emergency department.
Outcomes
At Guy’s and St Thomas’s NHS Trust, there are a number of different electronic noting systems used for patient care. We worked with the systems relevant to patients presenting to the ED, working primarily with ‘E-Noting’, which is the admission record, and also with Electronic Patient Record, which documents outpatient attendances and results from investigations, and Symphony Egton medical information system (EMIS client). We retrospectively collected information on investigations, outcome, date and time of presentation and departure, basic patient demographics, referral type, and final location. We also looked at data from subsequent visits to secondary care within the trust, particularly any neurology/headache outpatient appointments, to ascertain whether a final headache diagnosis was made. We noted any neurosurgical transfers to our partner neurosurgical centre, King’s College Hospital, London. Changes in final diagnosis at discharge compared to preliminary diagnosis on admission were also recorded.
For each presentation, we recorded whether the patient received a CT brain scan, an MRI brain scan, an MRA scan, or had a lumbar puncture performed during their admission. Multiple scans in the same visit were recorded as a patient receiving that scan at least once. We therefore present results for this section as the number of patients scanned rather than the number of scans per patient. We noted length of stay data as number of days (including half days) starting from admission to hospital services, not from presentation to the ED.
The data was organised according to initial diagnosis made at presentation to the department. This was a provisional diagnosis prior to any investigations. We noted diagnosis on discharge, which was what we termed the “final diagnosis” and this was what we used to calculate the cost of attendance and admission. This diagnosis was either made by the ED physician, general medical physician or neurologist (if there was a neurology consultation during this period). Since many of the final diagnoses were made by ED specialists or general physicians, the International Classification of Headache Disorders (ICHD) (4) was not necessarily used. We categorised the headaches as primary headache, cranial neuralgia or secondary headache. Where no definitive diagnosis was made upon leaving GSTT care, the diagnosis on discharge was coded as “inconclusive”.
Analysis
The headaches were characterised with descriptive statistics for patient demographic data, investigations and ED diagnosis. The mean age and standard deviation was calculated for the primary and secondary headache groups. Missing data were managed by complete-case analysis. Sample size was not estimated in advance and all the calculations were based on the available data. Healthcare costs were analysed for categories of attendance, investigations and admissions and were calculated over the 6-month period. The tariffs were different for patients attending the ED with a CT head scan (£317) compared to those who were admitted to the acute admissions unit for short stay for investigations such as MRI and lumbar puncture (£1047). Those who were admitted to the general wards had an individualised cost of admission applied by the coding department. The mean length of stay was also calculated using 0.5 days as a minimum length of stay to encompass any stay that was shorter than 12 hours. Any subsequent day was calculated as a whole day.
Results
There were 78,273 total attendances to the adult ED at St Thomas’s Hospital and Guy’s urgent care centre between 1 January 2018 to 30 June 2018, 976 (1.2%) with the primary presenting complaint of ‘headache’. Thirty six patients were excluded because the available data was insufficient. Figure 1 shows the breakdown of diagnostic categories. Two hundred and four (21%) patients were admitted to hospital, including the 12 neurosurgical transfers who were admitted to King’s College Hospital. Two hundred and thirty-eight patients underwent cranial imaging and 52 had a lumbar puncture.

Final diagnostic category of headache. Primary and secondary headache disorders and cranial neuralgias as defined by ICHD. Unspecified diagnosis group includes 70 patients labelled as having “benign” headache.
Primary headaches
Of the 510 patients in the primary or “benign” headache category, 436 had a primary headache disorder as defined by ICHD (4) (Table 1), 297 had a final diagnosis of migraine (68% of the primary headache group), 121 were diagnosed with tension-type headache (TTH) (27.8% of the primary headaches) and five were diagnosed with cluster headache (1%). A further 13 were diagnosed with other primary headache types, including eight with primary headache associated with sexual activity, two SUNCT, primary exercise headache, one primary stabbing headache and one hemicrania continua (Table 2). Another group of patients consisted of 70 (7% of all headache) patients who were given a broad diagnosis such as “benign headache” or “primary headache” and had no atypical features/red flags or they had the necessary investigations to exclude a secondary headache. This differed from the group of 103 patients with “diagnosis unspecified”, where there was no headache diagnosis made or they had not undergone complete investigation (see the Supplemental material).
Demographic data.

Primary headache on final diagnosis – includes only diagnoses which are “primary” according to ICHD (4).

LP: lumbar puncture; SUNCT: short-lasting unilateral neuralgiform headache with conjunctival injection and tearing. Total numbers are shown in bold.
There were four patients with trigeminal neuralgia. None were admitted. Seventeen patients in the migraine group and three in the TTH group were repeat attenders to the ED within the 6-month period. One hundred and fifteen out of 510 patients (23%) had imaging, mostly CT head.
Migraine
There were 297 migraine attendances (30% of attenders), of which 50 were admitted to hospital, representing 25% of total admissions for patients presenting with any type of headache. The male to female ratio was 1: 3. The mean age was 35 years (SD 12).
With regards to investigations, 21% of patients with migraine had CT scans, while 4.4% had MRI or MRA scans, and 5% had lumbar punctures. Eight percent of these patients had new neurology referrals made. Only 24 patients were referred to neurology/headache clinic on discharge.
Tension-type headache
It was noted that 15.8% of patients with a final diagnosis of tension-type headache had CT scans, 2.5% had lumbar punctures, and there was one new neurology referral made. Eight patients were admitted.
Table 3 shows the imaging findings in all patients who were coded as having a primary headache disorder at presentation to the ED, although this diagnosis may have changed on discharge. The abnormal finding on CT and MRI was in the same patient with subdural haemorrhages on CT and features of low CSF volume on MRI. Incidental findings included a small aneurysm, meningioma, arachnoid cyst, old infarcts, and white matter lesions.
Investigations on all patients presenting with a preliminary diagnosis of a primary headache disorder.

Cost of investigations and admissions for migraine
The mean length of stay in hospital for the 88 patients finally diagnosed with a primary headache who had been admitted was 1.38 days (SD 1.1). Length of stay ranged from 0.5 days to 5 days. The total number of days of admission on a medical ward was 41 and 80 days on the acute admissions unit.
Looking at those with a definitive diagnosis of migraine, the cost of admission including investigations was £52,634.
Taking into account the cost of attendance and investigation of the remaining 248 migraine patients, £78,616 the total cost of admissions, attendance and investigation for migraine overall was £131,250 during the 6-month period.
Secondary headaches
Of the 976 patients presenting with headache, 363 (37%) were diagnosed with a secondary headache disorder (Table 4). In all, 1.8% of patients presenting with headache were diagnosed with intracranial vascular causes of secondary headaches including subarachnoid haemorrhage, intracerebral haemorrhage, transient ischaemic attack, and stroke. A total of 77.7% of these patients were admitted and had CT scans, and 66.6% were transferred to the neurosurgical unit at King’s College Hospital.
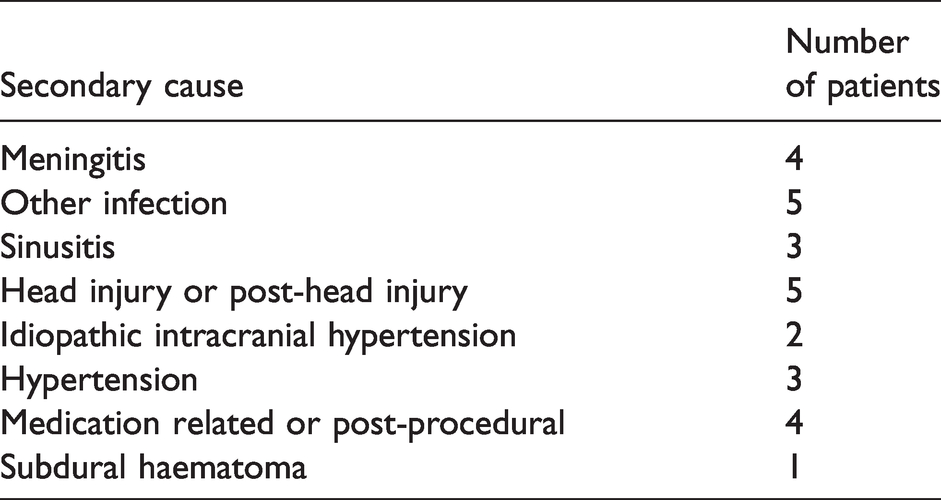
Secondary headaches.

LP: lumbar puncture; SAH: subarachnoid haemorrhage. Total numbers are shown in bold.
We noted that 1.6% of all headache patients were diagnosed with meningitis or encephalitis. In most cases the diagnosis was suspected at admission but three patients had a provisional diagnosis of migraine, with a further patient having an admission diagnosis of tension headache type.
Nine patients (0.9%) were diagnosed with idiopathic intracranial hypertension. This group had initial diagnoses on admission of tension headache, subarachnoid haemorrhage, muscle injury or belonged to vague categories such as “other nervous system disorders” and “no abnormality detected”.
Six patients, 0.6% of all patients presenting with headache to the emergency department, had a neoplastic cause for their headache. Half of these patients were admitted to hospital. These included a pontine glioblastoma, pituitary macroadenoma, nasopharyngeal carcinoma and a meningioma. There was also a facial and vestibular schwannoma case. It is important to note that all of the patients within this group had known malignancies upon presentation to the ED. One of these was admitted from clinic when the diagnosis was made on imaging.
Change in diagnosis
Sixty-seven patients thought to have a secondary headache on presentation to the ED were subsequently diagnosed with a primary headache on discharge. This represented 6.9% of all patients presenting with headache. Fifty percent of these patients were admitted to hospital, 53.0% had CT scans, 22.7% had lumbar punctures, 12.1% had new neurology referrals, and 7.5% had MRI or MRA scans. The majority of these (68.2%) had migraine. Subarachnoid haemorrhage was queried in 39% cases.
Conversely, 27 patients provisionally diagnosed with a primary headache on presentation were diagnosed with a secondary headache after appropriate investigations. This represented 2.8% of all patients presenting to the ED with headache. The final diagnoses are listed in Table 5.
Diagnoses in patients initially thought to have a primary headache syndrome.
In 173 (18%) patients, a final diagnosis was not specified with 70 of these labelled as benign or primary headache when secondary causes were excluded by investigation. There was no follow-up or investigation in the remaining 103 patients.
Discussion
In all, 45% of patients attending with “headache” had a final diagnosis of a primary headache disorder, of which 68% were diagnosed with migraine and 28% TTH. This figure is likely to underestimate the actual number of migraine patients since it is very likely that many of those diagnosed with TTH or in the “benign headache” group may actually have migraine since physicians unfamiliar with headache may not take a detailed headache history and can often misdiagnose TTH due to lack of positive migrainous symptoms (e.g photophobia, phonophobia) if these are not specifically asked about (5–7). Also, if the headache is severe enough to warrant attendance to the ED, it is less likely to be TTH. In fact, of the eight patients diagnosed with TTH who were admitted, two had clear migrainous features documented, three had sudden onset, severe headache with dizziness or blurred vision and were investigated for subarachnoid haemorrhage with a lumbar puncture, clearly not in keeping with a diagnosis of TTH (4). Some of the secondary headache diagnoses are also diagnoses of exclusion. For example, headache attributed to sinus problems was often diagnosed when other investigations did not reveal a cause. In some cases, the patient may have had a facial pain element or coryzal symptoms. Facial pain of migraine may be misdiagnosed as sinus-related headache (8).
There were 17 repeat attenders (5.7%) in the migraine group, which is relatively low.
A significant abnormal finding was only noted for only one of the 65 patients scanned in the primary headache disorder group. Twenty three percent of those attending ED underwent imaging. The very low pick-up rate of significant abnormality suggests perhaps this rate should be much lower. Also, the fact that no de novo neoplastic malignancies were detected should be noted as this is often a concern of the patient and sometimes the physician.
A study in 2006 in Sheffield, UK, looked at 558 patients with headache (excluding traumatic headache or those with altered levels of consciousness) and noted that 30% were admitted although they did not distinguish the different diagnoses of those admitted (9). In this study, 54% of all patients were diagnosed with a primary headache, a figure similar to our study, and 27% had CT scans. In an Australian study, migraine was diagnosed in 23% and 38% of all patients had a CT scan (10). Similarly high figures have been reported in Europe and the USA. A recent joint Italian and Austrian study surveyed 415 non-traumatic ED headache patients and found that 45% had a primary headache, 26.5% had migraine (11). In a US study, it was noted that headache accounted for 2.4% of visits to the ED with migraine being diagnosed in 34.6% (2). A common finding in many of these studies is the significant number of patients without a specific headache diagnosis. This accounted for 18% in our study compared with 21% in the other UK study (9) and 32–44% of patients in studies from Europe (11), the US (12) and Australia (10).
Economic burden
Nearly one third (30%) of patients admitted for headache in our study had a final diagnosis of migraine. Approximately 10 million people live with migraine in the UK (3). It is estimated that the NHS spends around £150 million per year on treating migraine and £250 million on care for headache sufferers (13).The cost to the wider economy is even higher, with around £4.4 billion a year lost to three million migraine-related sick days.
A study comparing the cost of healthcare for patients with migraine in Europe found that the percentage of chronic migraineurs hospitalised was higher in the UK compared with France, Germany, Italy or Spain, although this study used a voluntary online survey for data collection (14). The study also noted that the unit cost estimate for a primary care physician visit and neurologist visit was higher in the UK compared to the other four countries.
The cost of admission and investigations for our group was £131,250. This works out as £439 per migraine patient, with the caveat that length of stay and level of investigation affects the cost. Apart from the financial burden, there is also a risk to the migraine patient. Five percent of those diagnosed with migraine underwent an invasive procedure (lumbar puncture) and 21% had CT head scans, which may be exposing migraineurs to potential harm. Those admitted would be at potential risk of exposure to hospital-acquired infections. Migraineurs should not have to resort to attending their ED to provide them with a diagnosis or for treatment of acute exacerbations.
The NHS in England is free for all patients at all levels of care, so unlike other countries there are no financial reasons why a patient is more or less likely to attend the ED rather than their primary care practice. Primary care physicians or general practitioners (GPs) are meant to be the first port of call for patients with chronic conditions such as migraine, yet patients are finding it increasingly difficult to get appointments with their GP in a timely manner due to strains on the system (13). Other possibilities include low levels of satisfaction with their GP due to a lack of knowledge about migraine (15). These factors may partly explain the 14% increase in headache patients attending ED with headache over the last 5 years (3) in England. The catchment covered by Guy’s and St Thomas is an urban area, much of which is socioeconomically deprived, and with a larger proportion of GPs being temporary or in locum positions than in more affluent or rural locations. This makes it harder to educate the local GPs in headache diagnosis and management and also means educating patients is more challenging.
Despite having a specialist headache service, there was a low rate of referrals to neurology/headache services (8%) for migraine and for the other primary headache groups. This may be because the onus is placed on general practitioners to refer and may partly be due to financial implications of initiating a referral. It may also reflect a lack of awareness of the service amongst junior ED staff, who tend to be on 6 month rotations, and this is one of the issues we plan to address.
Limitations
One of the advantages of performing a retrospective study is that there was a 1-year follow up period during which we could capture any later admissions resulting in a change in diagnosis. There are also disadvantages using retrospective data, however, one of which is that we are reliant upon the diagnosis made by the physician at the time. This may be an ED physician, general medical physician or neurologist (if there was a neurology consultation during this period), so there may be some diagnostic inaccuracy. Since the purpose of our study was to audit current clinical practice, we relied on the diagnoses made although we suspect the actual numbers of patients admitted with migraine to be higher. Our trust has one of the UK’s busiest accident and emergency services and is therefore representative of a large urban population. However, this a single-centre study and in order to reflect the extent of admissions/attendances of migraine nationally one would have to extend the study to include centres in rural locations and centres without dedicated neurology/headache services. Another limitation is that if a patient had more than one scan (e.g repeated MRI) this was only counted as one per patient. This may have resulted in an underestimated cost of imaging in patients with repeated scans.
Following on from this audit, we plan to initiate a regular educational programme for ED junior doctors during their induction and to create a trust-specific headache protocol. Currently the NICE guidelines for headache are used (16). We aim to set up a “hot headache” clinic to divert patients from the ED and to reinforce our local headache pathway. We have already run education sessions for our local GPs but we now plan to initiate community-based headache clinics within the local primary care practices to improve GP education (17) and, equally importantly, patient education to enable better self-care and encourage them to utilise their GP more (15). From a national perspective, there is much to be done to improve headache education. Headache teaching is not on the curriculum for many undergraduate medical schools in England and also not a compulsory part of GP training. A national initiative has been launched to improve healthcare for people with headache disorders and aims to engage commissioners as well as health care providers (13).
Conclusion
At least a third of patients presenting to the emergency services with headache had migraine. Migraine accounted for a quarter of admissions to hospital. The total cost of admissions, attendance and investigation for migraine was £131,250 during the 6-month period. This demonstrates the impact of migraine on acute and emergency medical resources as well as the physical and mental burden on the migraineur. The data suggests that resources should be directed towards education for physicians and patients and developing better ambulatory care pathways for migraineurs.
Public health relevance
Migraine accounts for 30% of emergency ‘headache’ attendances and 25% of admissions in a busy London teaching hospital. The cost of migraine admissions to hospital is significant and avoidable. Resources need to be allocated to the community and towards educating clinicians and patients about migraine.
Supplemental Material
sj-pdf-1-cep-10.1177_0333102420981734 - Supplemental material for The burden of migraine on acute and emergency services in a London teaching hospital
Supplemental material, sj-pdf-1-cep-10.1177_0333102420981734 for The burden of migraine on acute and emergency services in a London teaching hospital by Jessica Southwell and Shazia K Afridi in Cephalalgia
Footnotes
Acknowledgements
The authors thank Matt May and James Couzens for their contribution.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.