
Abstract
Background
While the Global Burden of Disease study reports headache disorders as the third-highest cause of disability worldwide, the headache data in this study largely come from adults. This national study in Iran, the first of its type in the Eastern Mediterranean Region, was part of a global schools-based programme within the Global Campaign against Headache contributing data from children (6–11 years) and adolescents (12–17 years).
Methods
We followed the generic protocol for the global study. In a cross-sectional survey, self-completed structured questionnaires were administered to pupils within their classes in 121 schools selected from across the country to be representative of its diversities. Headache diagnostic questions were based on ICHD-3 criteria but for the inclusion of undifferentiated headache.
Results
Of 3,357 potential participants, 3,244 (children 1,308 [40.3%], adolescents 1,936 [59.7%]; males 1,531 [47.2%], females 1,713 [52.8%]) satisfactorily completed the questionnaire. Children and males were therefore somewhat under-represented, with a participating proportion of 96.6%. Gender- and age-adjusted 1-year prevalence of any headache was 65.4%, of migraine 25.2%, of tension-type headache 12.7%, of undifferentiated headache 22.1%, of all headache on ≥15 days/month 4.1%, and of probable medication-overuse headache 1.1%. All headache types except undifferentiated headache were more prevalent among adolescents than children; probable medication-overuse headache increased five-fold between childhood and adolescence.
Conclusions
Headache disorders are common in children and adolescents in Iran, with undifferentiated headache accounting for over one third of cases. The increasing prevalence of probable medication-overuse headache with age is concerning. These findings are of importance to health and educational policies in Iran.
Keywords
Introduction
While the Global Burden of Disease study reports headache disorders as the third-highest cause of disability worldwide (1,2), the headache data in this study come very largely from adults. The present study is part of the global schools-based programme within the Global Campaign against Headache, directed by Lifting The Burden (LTB) (3 –5), which aims to address this deficiency. The programme uses standardised methodology and instruments to estimate the prevalence and burden of headache disorders among children (aged 6–11 years) and adolescents (aged 12–17 years).
Headache disorders are of especial importance in these age groups, not only because they portend lifelong health loss but also, and more particularly, because their impact on education can cause cumulative lifelong disadvantage (6,7). Migraine, tension-type headache (TTH) and the group of disorders characterised by headache on ≥15 days/month (H15+), including medication-overuse headache (MOH), have all been common in studies so far reported within the global programme (8 –12). A key finding of these studies was the high prevalence of undifferentiated headache (UdH), believed to be expressions of migraine or TTH by the immature brain (8) but meeting International Classification of Headache Disorders (ICHD) diagnostic criteria (13) for neither.
The aims of this study were to estimate the prevalence of these disorders, and their attributed burden, in Iran. It is the first such study from the Eastern Mediterranean Region, adding to those from European (8,9), Western Pacific (10) and African Regions (11,12). While there is published evidence of headache-attributed burden among adults in Iran, the data are not population-based (14 –16). Iran is the second-largest country in the Middle East after Saudi Arabia, although much of it is mountainous and uninhabitable. Within its population of 85 million, about three quarters are urban dwelling and a quarter are aged 15 years or under (17). Although Iran is historically a multinational state, over 95% of its population are either Iranic (about three quarters, mostly Persians, with fewer Kurds and small communities of others) or Turkic (about one quarter, the largest group being Iranian Azerbaijanis). The Iranic and Iranian Azerbaijani peoples are genetically and culturally similar. There are linguistic diversities, but Articles 15 and 16 of the Constitution of the Islamic Republic of Iran identify the Persian (Farsi) language as the lingua franca, and require its use throughout the school system (18). Education is highly centralised and free, except for a small proportion of schools that are private, with tuition fees. Schooling is mandatory from 6–15 years of age, with over 80% of pupils continuing upper-secondary education to age 18 (19). Restrictions on the education of females were lifted in 1989.
The purposes of the study were to inform local health and educational policies, and add to global knowledge of headache burden. This manuscript reports prevalences; headache-attributed burden will be reported later.
Methods
The basic study design, following the generic protocol (20), was a cross-sectional survey conducted by self-completed structured questionnaires administered in schools selected to be representative of Iran’s diversities.
Ethics and approvals
The study was approved by the Ethics Committee of Tehran University of Medical Sciences, Tehran (reference number: IR.TUMS.NI.REC.1397.211).
The survey was explained to school managers and teachers of selected schools, whose agreement to participate was required. Information forms describing the study’s nature and purposes were given to all intended participants, for themselves and their parents. Consents from both pupils and parents were required for entry to the study.
Questionnaires were collected anonymously.
Sampling and recruitment
The study was conducted from 1 December 2018 until 31 March 2019.
We purposefully selected 121 schools from urban and rural areas of 13 of Iran’s 31 provinces (Figure 1), aiming to reflect, in the sample, the country’s geographical, genetic, cultural and socio-economic diversities. All pupils aged 6–17 years, from all classes, were invited to participate in the survey, although numbers per school varied greatly (<20 from some rural schools with limited classes and few pupils). Those absent on the survey day, those declining to participate and those whose questionnaires were insufficiently completed for analysis were excluded and counted as non-participants.
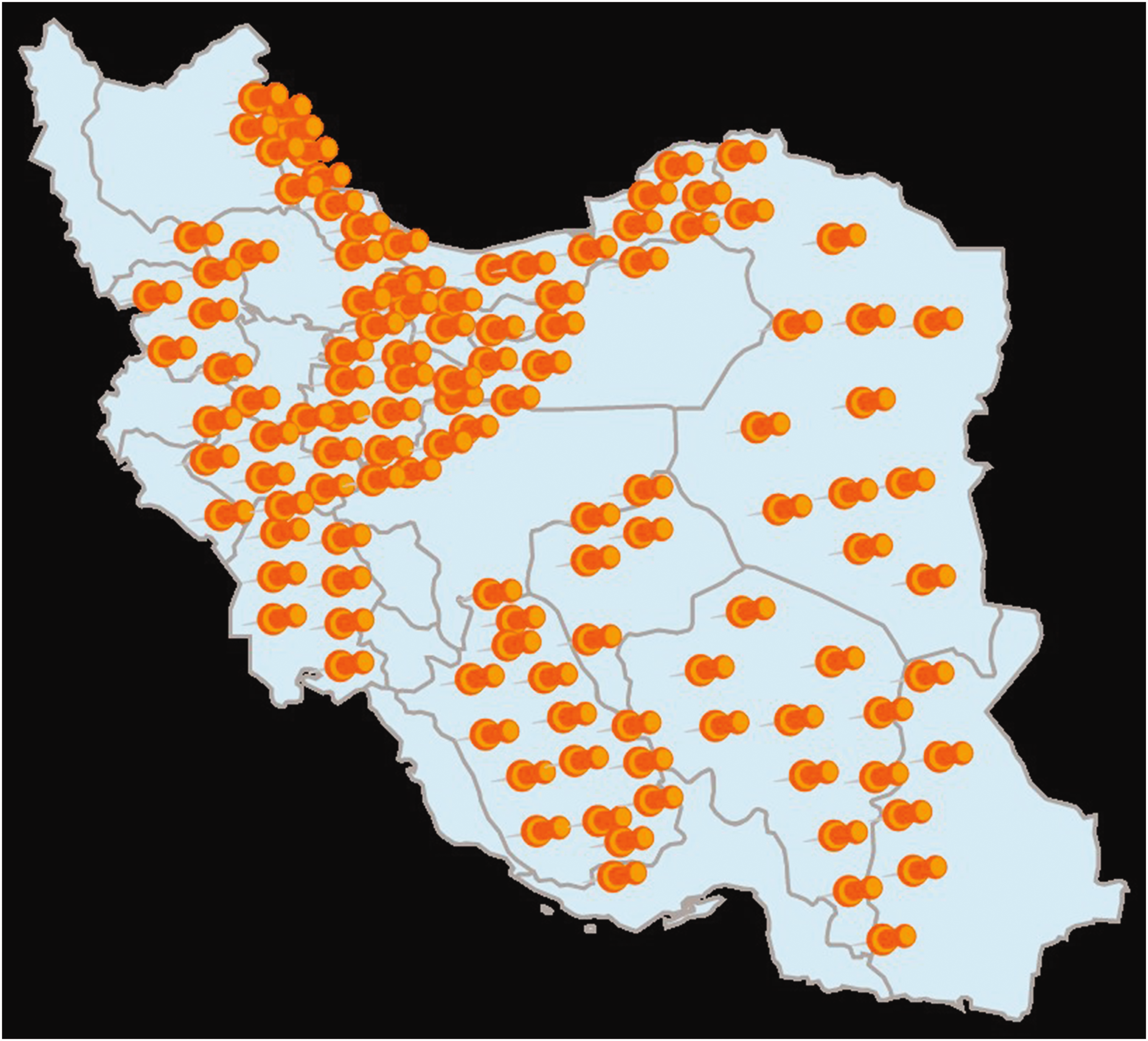
Distribution of the 121 selected schools in 13 provinces of Iran.
We aimed for N > 3,000. A sample size of N = 2,000 is recommended for headache prevalence, but a larger sample size is more informative for burden estimation (21).
Survey instruments
We employed the child and adolescent versions of LTB’s Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation (HARDSHIP) structured questionnaire (20), translated into Persian language according to LTB’s translation protocol for hybrid documents (22). These modular instruments, designed for application by lay interviewers, incorporated demographic enquiry, headache screening and diagnostic questions based on ICHD-3 criteria (13) and enquiries into components of headache-attributed burden. The timeframe of enquiry was the preceding 4 weeks (28 days), except for the module asking specifically about headache yesterday (HY).
Pupils completed their questionnaires in class under the supervision of the teacher or an investigator. These questionnaires did not identify participants, and data collection was anonymous except to the extent that younger children, and those unable to read well, were given necessary assistance in understanding and appropriately answering the questions.
Additional questionnaires enquiring into relevant school variables were completed by the managers of the schools.
Diagnoses
Diagnoses were made algorithmically according to HARDSHIP methodology (6). H15+ (i.e., headache reported on ≥14 days in the preceding 28 days) was first identified and categorised according to reported medication use into probable MOH (pMOH: use on ≥14 days/28 days) or “other H15+” (use on 0–13 days/28 days). To all other reported headaches, the algorithm first applied criteria for UdH (mild intensity and usual duration <1 hour (8)) and then the ICHD-3 criteria for definite migraine, definite TTH, probable migraine and probable TTH in this strict order (13). Remaining cases were recorded as unclassified.
Data management and entry
All questionnaires were removed to the Department of Headache, Iranian Center of Neurological Research at Tehran University of Medical Science, and held securely. Initial data entry into SPSS version 19 was performed by a trained data-entry clerk employed by the local research team. As a quality-assurance measure, a separate member of the team compared the SPSS dataset with the original questionnaires.
Analysis
Analyses were performed at University of Mersin.
We categorised schools by location (urban or rural) and, as a socio-economic indicator, by estimated proportions of pupils coming from low-income homes (<0.25, 0.25-0.5, 0.5-0.75 [categories referred to for simplicity as “high-income”, “middle-income” and “low-income”]). We used descriptive statistics to present means and standard deviations (SDs) of continuous variables and proportions (%) with 95% confidence intervals (CIs) of categorical data. We used chi-squared or one-sample proportion tests to evaluate differences between groups. We estimated prevalences of each headache type as proportions (%), and adjusted the crude values for gender and age using official population statistics for Iran (23). In these analyses, in accordance with published guidelines (21), definite and probable migraine were combined, as were definite and probable TTH. To show associations with demographic variables, we first used bivariate analysis with odds ratios (ORs), then multivariate logistic regression analysis with adjusted ORs (AORs), entering gender, age group, school location and income category into the multivariate model. Mean headache frequencies (days/month) were calculated to support estimates of predicted headache yesterday.
We considered p < 0.05 to be significant.
Results
The sampled population consisted of 3,357 children and adolescents, of whom 14 did not participate (males = 8, females = 6): five were absent on the day and nine declined to participate. In addition, 99 questionnaires, with >50% of responses missing, were considered insufficiently completed for analysis. Participating proportion was therefore 96.6%, with N = 3,244 (children 1,308 (40.3%), adolescents 1,936 (59.7%); males 1,531 (47.2%), females 1,713 (52.8%)). Since we intended to have similar numbers of each age group and gender, children were under-represented, as were males. Mean age of the sample was 12.3 (±3.2) years (median 12.0).
Participants are categorised according to school variables in Table 1. Over three quarters (77.7%) attended urban schools. Only a small minority (5.4%) attended schools where >50% of pupils were from low-income homes.
Participant pupils categorised according to school variables (from teachers’ questionnaires) (N = 3,244).

Headache
Headache ever was reported by 2,570 pupils (crude lifetime prevalence: 79.2%), and headache in the preceding year by 2,301 (crude 1-year prevalence: 70.9%; gender- and age-adjusted: 65.4%). Observed and adjusted prevalences of each headache type are shown in Table 2.
Crude (observed) prevalences of all headache and each headache type, overall and according to demographic variables, and gender- and age-adjusted prevalences (N = 3,244).

Migraine (25.2%) and UdH (22.1%) were the most common headache types after adjustment, followed by TTH (12.7%) (Table 2). H15+ was reported by more than one participant in every 25 (4.1%); mean headache frequency among these was 19.1 days/28 days. These included 1.1% with pMOH, who reported medication use on 18.0 days/28 days. There were 44 headaches cases (1.3%) remaining unclassified.
Demographic associations
The demographic associations are illustrated in Tables 2 –4, but there were few of significance. Overall, headache was more prevalent among females (72.7%) than males (69.0%; Table 2), but among the headache types this was clearly reflected only in other H15+ (AOR = 1.8) (Tables 2 –4). Migraine and TTH trended in opposite directions. Migraine (AOR = 2.3), TTH (AOR = 1.7), pMOH (AOR = 5.0) and other H15+ (AOR = 5.4) were all more common among adolescents. Prevalence of UdH increased from 10.5% at age 6 years to a maximum of 30.0% at age 10, then showed an undulating decline to 17.5% at 17 years. This was against a background of increasing prevalence of all other headache types, so that, as a proportion of all headache, UdH declined from 40.1% among children to 29.0% among adolescents. Income category had no effect on prevalences. Both pMOH (AOR = 5.9) and other H15+ (AOR = 2.4) were more common in urban schools (Tables 2 –4).
Bivariate analyses of headache type versus demographic variables (N = 3,244).

CI: confidence interval; pMOH: probable medication-overuse headache; d/m: days/month; TTH: tension-type headache; UdH: undifferentiated headache. * see text or Table 1 for explanation. Significant values are emboldened: 1p < 0.05; 2p < 0.01; 3p < 0.001.
Multivariate logistic regression analyses of headache type versus demographic variables (N = 3,244).

CI: confidence interval; pMOH: probable medication-overuse headache; d/m: days/month; TTH: tension-type headache; UdH: undifferentiated headache. * see text or Table 1 for explanation. Significant values are emboldened: 1p < 0.05; 2p < 0.01; 3p < 0.001.
Headache yesterday
The questions on HY were answered by 2,279 of the 2,301 pupils with any headache in the last year. HY was reported by 670 (29.4% of those with any headache; 20.7% of the total sample) (Table 5). Females (35.0%) reported HY more than males (22.8%; AOR: 1.9 (1.5–2.3); p < 0.001), and adolescents (33.0%) more than children (21.2%; AOR; 1.5 (1.2–1.9); p < 0.01).
Proportions reporting headache yesterday, and predicted proportions*, overall and by headache type (N=3,244).

*calculated as F/28.
pMOH: probable medication-overuse headache; d/m: days/month; TTH: tension-type headache; UdH: undifferentiated headache.
Mean headache frequency in the 2,279 reporting any headache was 3.9 days/28 days. Probability of HY among these, calculated as proportion of days affected, was 13.9% (3.9/28). Since the observed prevalence of all headache was 70.9% (Table 2), 9.8% (74.2*13.2%) of all participants would be expected to have headache on any day (predicted HY). Pupils with all episodic headache types reported substantially more HY than predicted, notably those with migraine and UdH (by factors of 2.65 and 2.5) (Table 5). H15+, including pMOH, the greatest contributor proportionately to HY, was reported yesterday only slightly more than predicted.
Discussion
This was the sixth national study of child and adolescent headache to be completed within the Global Campaign programme of such studies. Its findings confirmed, again, that headache is very common among these age groups. In summary, in Iran, almost two thirds (65.4%) are affected with a current headache disorder, a quarter (25.2%) with migraine. UdH is also common (22.1%), but TTH less so (12.7%). H15+ affects one pupil in every 25 (4.1%), with pMOH estimated at 1.1%. Among our sample, more than one in five (20.7%) claimed to have had headache yesterday. As often observed in these age groups, associations with gender were weak (only H15+ was clearly more prevalent in females, while migraine and TTH trended in opposite directions). All headache types other than UdH were, as expected, more common among older pupils; UdH declined with age as a proportion of all headache. H15+, and especially pMOH (AOR = 5.9), were more common in urban than in rural schools.
Important among these findings is confirmation once again that UdH (here accounting for over one third of all reported headache) must be included in prevalence (and burden) estimates. As noted when it was first described, UdH probably represents expressions of migraine and TTH by an immature brain, with the characteristic features of these headaches yet to develop (8). Accordingly, UdH declined with age in this study, as a proportion of all headache, from 40.1% among children to 29.0% among adolescents against a background of increasing headache prevalence. Also important was the prevalence of pMOH. Although overall this was only 1.1%, what is of concern is the strong association with age, with AOR = 5.0 in adolescents (prevalence 1.9%) compared with children (prevalence 0.4%) (Table 2). Thus is the pattern set for MOH in adults, a significant and costly cause of disability in Iran (16). MOH is an acquired disorder, attributable to a behaviour that, when it occurs in children, is most probably taught to them by their parents. It should, however, be noted that, behind the increase in pMOH, and probably feeding it, was a similarly increasing prevalence of other H15+.
The other point to be made about pMOH is its much higher prevalence among urban schools compared with rural (AOR = 5.9). This has been noted in adult studies in Ethiopia (24) and Zambia (25), and attributed to easier availability in towns of over-the-counter medication. As a general rule, however, health care is also more accessible in urban settings, and ought to discourage medication overuse. In Iran, health care is highly developed and equitably provided, but apparently it is failing in this regard.
There are no comparable data from these age groups in Iran, and within Eastern Mediterranean Region there are data only from Kuwait (26). Although this study used the same questionnaires (child and adolescent versions of LTB’s HARDSHIP questionnaire (20)), it modified the key screening question, enquiring into “headache that was not part of another illness” rather than use a neutral question as recommended (21). Further, it did not account for UdH. For these reasons, the data from this study are not reliably comparable. In Table 6 we make comparisons with LTB’s five earlier national studies from other regions (8 –12), which are of interest because all used the same methodology and questionnaires. The two African studies, in Ethiopia and Zambia, are outliers with regard to migraine (the possible reasons behind this have been discussed in detail (11,12)). The findings in Iran are otherwise within the ranges of these studies, and very similar to those from Turkey (8), which is geographically and culturally the closest to Iran.
1-year headache prevalences in this and other studies using the same methodology and questionnaire.

TTH: tension-type headache; UdH: undifferentiated headache.
Headache yesterday was reported by one pupil in every five, implying that, on any day (or, at least, on any school day), one fifth of pupils have headache for at least part of the day. This is not highly feasible – much less so than the proportions predicted from prevalence and headache frequency of 13.9% of those with headache or 9.8% (one in ten) of all pupils. The proportion with H15+ (4.1%) account for many cases but, as in the other studies, pupils with episodic headache types reported substantially more HY than expected (here more than two-fold). If the predicted proportions are accepted as closer to reality, despite likely recall error, embellishment seems the most likely cause, induced or encouraged perhaps by the leading nature of the questions. This mode of enquiry is not ideal among children, and better alternatives need to be sought.
We note this as a possible study limitation. Lack of diagnostic confirmation was the more definite limitation, but inherent in this type of cross-sectional enquiry. In adult studies, re-interview of a subsample by a headache expert may be possible, providing a level of validation, but a second exposure to interrogation with no therapeutic purpose is ethically difficult in these age groups. A solution to this was not available.
The strengths of the study were several. It was conducted nationwide using tested and validated methodology (20) and recruited an adequate sample size with a very low non-participating proportion (3.4%). Mandatory schooling ensured the validity of schools-based sampling at least for those aged 6–15 years. Although children and males were relatively under-represented, statistical corrections for these were possible. The sample appropriately represented Iran’s urban/rural divide.
Conclusions
Headache disorders are common in children and adolescents in Iran, with findings similar to those from several other countries, in particular Turkey. UdH accounts for over one third of all headache. The prevalence of pMOH increases five-fold between childhood and adolescence, as does that of other H15+. While these findings are of academic interest, the next step is to supplement the prevalence estimates with estimates of attributable burden. As indicators of the ill-health consequences of headache, these are of greater importance from both public-health and educational perspectives.
Public-health relevance
Headache is very common in children and adolescents in Iran, as in other countries where its prevalence has been estimated. This has implications for educational as well as public-health policies in Iran. Undifferentiated headache must be recognised in these age groups. Unless it is included, accounts of headache prevalence and burden will be incomplete. The prevalence of pMOH, higher in urban than rural settings, increases five-fold between childhood and adolescence. This very probably sets the pattern for adult MOH, and indicates the need for educational intervention.
Footnotes
Data availability
The original data are held on file at the Iranian Center of Neurological Research, Tehran University of Medical Science. Once analysis and publications are completed, they will be freely available for non-commercial purposes to any person requesting access in accordance with the general policy of the Global Campaign against Headache.
Acknowledgements
We thank Dr Seyed Mohammad Hasan Paknejad, Dr Shahram Rafie and Dr Sepideh Amouian for their help in acquisition of data, and are grateful to the pupils and staff of the participating schools for their help and cooperation in this study.
Authors’ contributions
MT conceived the study, developed the protocol and supervised all the steps of the project with support from TJS and DU. PR, ZG and MT were responsible for data collection, with guidance from DU as coordinator of the global programme. TS and DA performed the statistical analysis. TJS drafted the manuscript. All authors contributed to manuscript revision and approved the final version.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TJS and DU are Directors and Trustees of Lifting The Burden. Otherwise, no author declares a conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by International Headache Society and Lifting The Burden.