
Abstract
Background
In Pakistan, we have shown that both migraine (one-year prevalence of 22.5%) and tension-type headache (TTH: 44.6%) are more common among the adult population than reported globally. Here, to inform local health policy and add to knowledge of the global burden of headache, we estimate the lost health and other burdens attributable to headache in this populous Eastern Mediterranean Region country.
Methods
In a cross-sectional survey using cluster-randomized sampling, we visited households unannounced in Punjab, Sindh, Khyber Pakhtunkhwa and Baluchistan. We randomly selected and interviewed one adult member (aged 18–65 years) of each household, using a validated Urdu version of the HARDSHIP (i.e. Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation) structured questionnaire. Burden enquiry was in multiple domains.
Results
In total, there were 4223 participants. Those with headache spent on average 6.4% of their time with headache of moderate intensity, with females worse affected than males. Participants with migraine were worse affected than those with TTH. Those with probable medication-overuse headache or other headache on ≥15 days/month spent 39.7% and 30.2% of their total time with headache. Quality of life, productivity and participation in social or leisure activities were impaired. Factoring in prevalence and adjusting for age and gender, we estimated that 4.9–5.9% of all time in this population was spent with headache, and, on average, 3.1 and 3.8 days were lost from paid and household work in the preceding three months. Over half (57.5%) of the population were assessed as needing care, but education promoting effective self-care might reduce this to 28.7% in need of professional care.
Conclusions
The burdens of headache in Pakistan are therefore very substantial in terms of health and productivity losses. These findings are important to national health and economic policies. The benefits in health gain from nationwide implementation of structured headache services, cost-effective in themselves, should be accompanied by enhancements in productivity, offsetting the cost of these services.
Keywords
Introduction
In its latest published iteration, the Global Burden of Disease (GBD) study attributed 5.23% of all years lived with disability (YLDs) to headache disorders, recognizing these as the third highest cause, among groups of related disorders, of global YLDs (1,2). Although there are over 200 headache disorders described in the International Classification of Headache Disorders (ICHD) (3), GBD includes only migraine and tension-type headache (TTH), along with medication-overuse headache (MOH), which arises from these. A few other primary headache disorders are highly burdensome at individual level but contribute little to population ill health because of their relative rarity, while any lost health due to secondary headache disorders is correctly attributed by GBD to their underlying causes (4).
With regard to headache, GBD relies solely on data from population-based studies (1). Over more than two decades, using standard methodology and survey instruments (5,6), the Global Campaign against Headache (7–9) has undertaken or supported a series of such studies in countries around the world, estimating headache prevalence and attributed burdens (lost health, impaired participation in daily activities, lost productivity and financial costs) (9). These have filled many of the large gaps in knowledge of the burden of headache worldwide that existed at the time of GBD2000, the first iteration to include migraine (10,11) (TTH was not included until GBD2010 (12) and MOH not until GBD2013 (13)).
These three headache disorders are expected to place heavy demands on health services and to require allocation of health resources accordingly, in competition with other demands on these resources (14). As well as informing GBD, these studies have been sources of local knowledge offering guidance to country policy makers in setting healthcare priorities. Crucially, this knowledge includes evidence-based estimates not only of headache-attributed population ill health and of need for health care, but also of the associated lost productivity and heavy financial cost of leaving these disorders untreated (14–17).
However, knowledge gaps remain (18,19). In the Eastern Mediterranean Region (EMR), studies completed by the Global Campaign have included Saudi Arabia (20,21) and Morocco (22,23), which are geographically distant and ethnically and culturally very different from each other. In each, headache disorders were found to be very common, and attributed burden very high. For Pakistan, an EMR country with the sixth largest population in the world (24), we have so far published only prevalence data, which were collected from a population-based sample of 4223 in 2010 (25,26). Three-quarters (76.1%) of Pakistan's adult population (aged 18–65 years) were estimated to be affected by any headache and age- and gender-adjusted one-year prevalences of both migraine (22.5%) and TTH (44.6%) (26) substantially exceeded global averages estimated in GBD2010 (14.7% and 20.8%, respectively) (12). We concluded that headache disorders must be on the public-health agenda of Pakistan (26).
Here, expressly to inform national health policy, but also to add to knowledge of the global burden of headache, we analyse headache-attributed lost health and impaired participation in this country, and conduct a healthcare needs-assessment, using data from the same survey. The study continues the series supported by The Global Campaign (7–9), and is the third of its kind (after those in Saudi Arabia (20,21) and Morocco (22,23)) to be published from EMR.
Methods
The methodology has been published in detail previously (25), but is summarized here for convenience.
Ethics
The study was conducted in accordance with the Declaration of Helsinki (27) and with approval from the Ethics Review Board of the Dow University of Health Sciences. All participants gave their written consent prior to interview, and had the option of discontinuing the interview at any time during it.
Data were managed in accordance with data-protection laws.
Study design
We used the standardized methodology and structured questionnaire developed by the Global Campaign (5,6).
We aimed for a nationwide study, but could not sample from almost 45% of the urban population who were slum-dwellers, or, for security reasons, enter the city of Quetta, areas north of Abbottabad or deep rural areas (25). We conducted the survey in six locations in the four provinces of Pakistan: Lahore and Multan (Punjab), Karachi and Sukkur (Sindh), Abbottabad (Khyber Pakhtunkhwa) and Gwadar (Baluchistan). Rural and urban households randomly selected in each location were visited unannounced by 12 trained non-medical interviewers recruited from, and therefore familiar with, the same locations. One randomly selected adult member (aged 18–65 years) of each household was interviewed using a validated Urdu-version of the structured Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation (HARDSHIP) questionnaire (6,25). HARDSHIP included demographic enquiry, headache screening and diagnostic questions and enquiry into various domains of burden: symptom burden, impaired participation and lost productivity (using the Headache-Attributed Lost Time (HALT) index (28), a module within HARDSHIP), as well as quality of life (QoL) (using the World Health Organization Quality of Life 8-item questionnaire (WHOQoL-8) (29), also inserted as a module within HARDSHIP).
Headache diagnoses
The screening question for headache was: “In the last year, have you had headache?” Participants who answered “yes” were asked if all their headaches were of one or more types and, if more than one, to focus in the subsequent questions on the type that was most bothersome for purposes of diagnosis and burden enquiry.
The diagnostic questions based on ICHD-2 (30), the version then current, had been validated earlier in a Pakistani population (25). Headache diagnoses were made algorithmically from the responses to these, in steps (published in detail previously (6)): first identifying headache on ≥15 days/month (H15+) and, among these, probable MOH (pMOH) when acute medication overuse (on ≥15 days/month) was reported, then definite migraine, definite TTH, probable migraine and probable TTH. This procedure followed the hierarchy established in ICHD (30). Any remaining cases were unclassified.
Headache-attributed burden
The timeframes for burden enquiry were the preceding one year, three months, one month and one day, the last in questions addressed to those responding positively to “Did you have a headache yesterday (HY)?”
Symptom burden
Headache frequency (days/month) and usual duration (hours) were recorded as continuous variables. Usual headache intensity was reported as “not bad”, “quite bad” or “very bad”, which we converted into a numerical scale of 1–3. We calculated proportion of time in the ictal state (pTIS) as the product of headache frequency and duration (the latter capped at 24 hours to avoid overestimation) divided by the total number of hours in one month (30 × 24). We computed attributed lost health at individual level for migraine and TTH as proportions (%) by multiplying pTIS for each by the respective disability weights (DWs) from GBD (31).
Duration (hours) and intensity (1–3) of HY were also recorded.
Impaired participation
HALT enquired into impaired participation over the preceding three months as lost days from paid work, household work (the necessary chores of everyday life) and social or leisure activities (28). Lost paid and household work together constituted lost productivity. Missing data were treated as zero because a question was likely to be unanswered when perceived as irrelevant (for example, days of paid work could not be lost by those who were unemployed). In accordance with established methodology, for lost productivity we equated “less than half achieved” on a particular day with “nothing achieved” (one day lost) and, to counterbalance, “more than half achieved” with “everything achieved” (no days lost) (28). In individuals reporting HY, overall impaired participation yesterday (not distinguishing between different domains) was similarly assessed as 0% or 100%.
Quality of life
Enquiry into QoL included all participants, with or without headache. We summed the scores for the eight WHOQoL-8 questions (each 1–5) for an overall score of 8–40, with higher scores indicating better QoL (29). We treated this as a discrete variable.
Healthcare needs assessment
We defined “need” for health care in terms of numbers judged not only to have significant health loss, but also likely to benefit from health care, assuming it was provided effectively. Accordingly, we counted among these everyone with H15+ (whether pMOH or other H15+). Of participants with migraine or TTH, we counted those meeting either or both of two criteria: a) pTIS > 3.3% (i.e. > 24 h/month) and usual intensity ≥2 (i.e. moderate or severe); b) lost productivity over the preceding three months from either paid or household work of ≥3 days. Additionally, but avoiding double counting, we included all participants with migraine reporting headache frequency of ≥3 days/month.
Statistical analysis
Means, standard errors of the mean (SEMs) and medians were used to describe continuous and discrete variables. We applied Mann–Whitney U-tests (when comparing two groups) or Kruskal–Wallis tests (when comparing more than two groups) to group differences in continuous and discrete variables and chi-squared tests to group-differences in categorical variables.
We calculated pTIS at population level by factoring in one-year prevalence and adjusting for age and gender. Similarly, we factored one-day prevalence into proportion of time spent yesterday with HY.
We calculated age- and gender-adjusted impaired participation at population-level over the preceding three months using HALT data, separately for paid work, household work and social or leisure activities. From HY data we estimated overall impaired participation, as a percentage, also at the population level.
Statistical analyses were performed using SPSS, version 28 (SPSS Inc., Armonk, NY, USA). p < 0.05 was considered statistically significant.
Results
The sample (N = 4223; participating proportion 89.5%) was representative of the national population regarding age, gender and habitation (urban/rural) (26). The characteristics were as reported earlier (26). Headache prevalence estimates, also reported earlier, are repeated here because they are used in burden analyses. Adjusted for age and gender, the one-year prevalence of any headache was 76.1%, migraine was 22.5%, TTH was 44.6%, pMOH was 0.8% and other H15+ was 7.4% (26). HY was reported by 17.9% of males and 22.3% of females (26).
Burden at individual level
Symptom burden
Table 1 shows the various measures. Means and medians are sometimes dissimilar, indicating some skewedness of data.
Symptom burden at individual level by headache type and gender.

pMOH = probable medication-overuse headache; H15+ = headache on ≥15 days/month; TTH = tension type headache; p-values indicating significance (<0.05) are shown in bold.
Overall headache frequency was 6.2 days/month, with a mean duration of 5.3 hours, mean intensity of 1.9 (moderate) and mean pTIS of 6.4%. For all of these, females reported significantly higher values than males (all p < 0.001). Although we did not compare them statistically, migraine was more frequent, longer lasting and more intense than TTH in both genders (Table 1). Gender-related differences in migraine and TTH were minor and mostly non-significant.
Inevitably, pMOH and other H15+ were much more frequent (21.0 and 21.9 days/month). Reported durations were also longer (13.6 and 12.4 hours) (Table 1), such that both were associated with very high values of pTIS (39.7% and 30.2%), the former markedly more so among females (44.5%) than males (24.6%; p = 0.009). Both were reported as moderate-to-severe (on a par with migraine) by both genders (Table 1).
Individual-level lost health was 1.8% for migraine and 0.1% (at the lower limit of measurement) for TTH.
Impaired participation
Figure 1 and Table 2 show mean headache-attributed lost days from paid and household work and from social or leisure activities over the preceding three months. Again, there was some skewedness of data.

Impaired participation in paid (red) and household work (green) and in social or leisure activities (blue) by headache type. Error bars are 95% confidence intervals. pMOH = probable medication-overuse headache; H15+ = headache on ≥15 days/month; TTH= tension-type headache.
Impaired participation at individual level in paid and household work and in social or leisure activities by headache type and gender.

HALT = Headache-Attributed Lost Time (index); pMOH = probable medication-overuse headache; H15+ = headache on ≥15 days/month; TTH = tension-type headache; p-values indicating significance (<0.05) are shown in bold.
Overall, for every individual with any headache, 3.9 days per three months were lost on average from paid work, 5.2 days from household work and 0.3 days from social or leisure activities. Males reported significantly higher losses from paid work than females for all headache types (all p < 0.001). In contrast, females reported higher losses from household work than males for all headache types except pMOH (p = 0.17; all others p ≤ 0.002) (Table 2). Migraine was associated with higher losses than TTH in all domains (Figure 1 and Table 2). Differences between migraine, pMOH and other H15+ in lost days from paid work were not significant, while pMOH was associated with the highest losses from household work (Figure 1).
Burden associated with headache yesterday
Table 3 shows symptom burden and impaired participation associated with HY.
Duration, intensity and impaired participation associated with headache yesterday.

*Equating to 1, 2 and 3, and treating as though continuous data; p-values indicating significance (<0.05) are shown in bold.
Mean duration of HY was 6.9 hours, being higher among females (7.9 hours) than males (5.3 hours) (p < 0.001). Mean intensity was 2.1 (moderate) in both genders. Of everyone with HY, 491 (62.9%) reported they could do everything as normal or more than half, but there was a marked gender difference: for males, the proportion was 77.4%, for females 58.3% (p < 0.001) (Table 3).
Quality of life
Figure 2 and Table 4 show WHOQoL-8 scores. For those with no headache, WHOQoL score was 28.6; for those with headache, scores (range 26.1–27.5) showed clear detrimental effect of all types (p ≤ 0.01 vs. no headache) (Figure 2). Migraine had greatest effect; TTH had least, but with only very small and insignificant differences from pMOH and other H15+.

Self-reported quality of life (World Health Organization Quality of Life 8-item questionnaire (WHOQoL-8)) by headache status. Error bars are 95% confidence intervals. pMOH = probable medication-overuse headache; H15+ = headache on ≥15 days/month; TTH = tension-type headache.
Quality of life (WHOQoL-8 score) by headache type.

pMOH = probable medication-overuse headache; H15+ = headache on ≥15 days/month; TTH = tension-type headache; p-values indicating significance (<0.05) are shown in bold.
Burden at population level
Table 5 shows the age- and gender-adjusted estimates of pTIS and impaired participation attributed to headache at population level (including those with and those without headache).
Proportion of time in ictal state and impaired participation at population level, by headache type and by timeframe of enquiry (adjusted for age and gender).
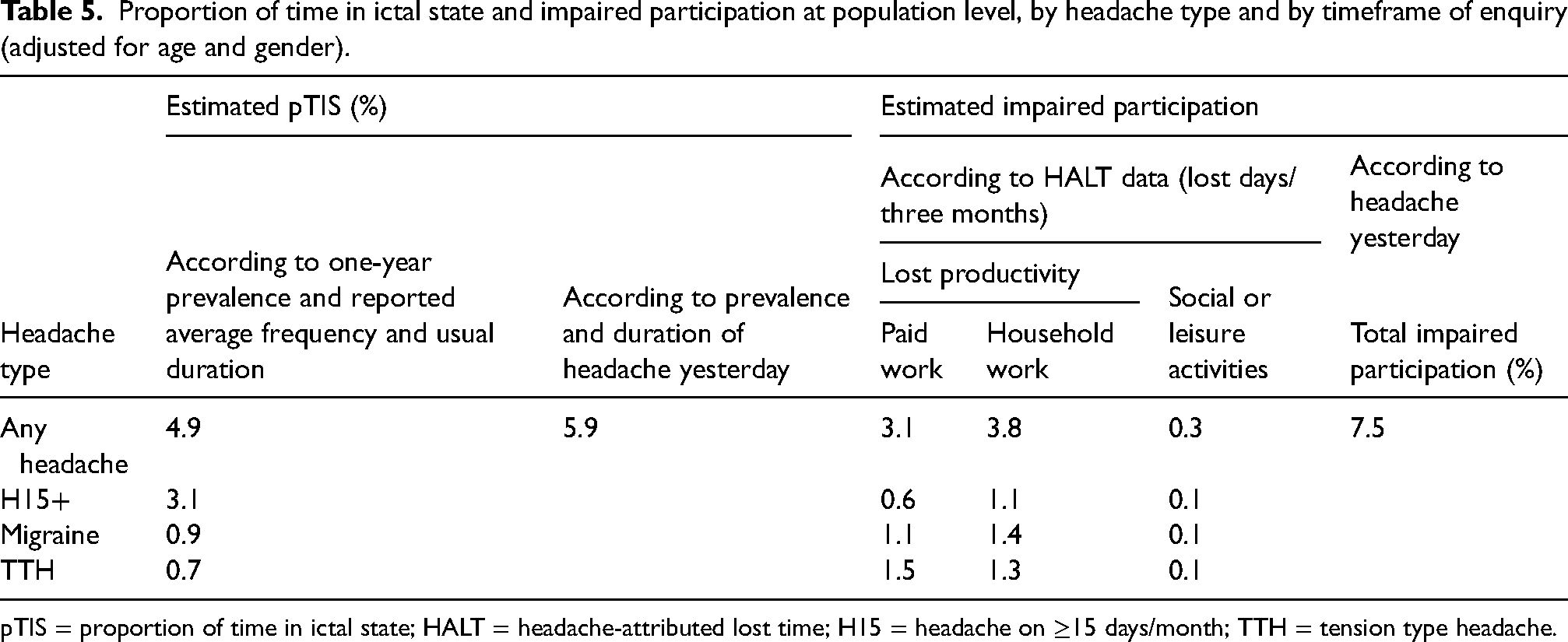
pTIS = proportion of time in ictal state; HALT = headache-attributed lost time; H15 = headache on ≥15 days/month; TTH = tension type headache.
The two methods of estimating population pTIS (from one-year prevalence and average recalled frequency and usual duration, and from prevalence and duration of HY) gave similar estimates of 4.9% and 5.9%. More than half of this time (3.1%, according to the former method) was spent with H15+ (a consequence of its very high prevalence (8.2%)), and much less with migraine (0.9%) or TTH (0.7%) (Table 5).
Headache-attributed impaired participation, according to HALT data, was estimated as 3.1 lost days per person (with or without headache) from paid work, 3.8 days from household work and 0.3 days from social or leisure activities during the preceding three months. The episodic headaches had greater negative impact than H15+ on participation both in paid work (migraine 1.1, TTH 1.5 and H15+ 0.6 lost days) and in household work (migraine 1.4, TTH 1.3 and H15+ 1.1 lost days). Impact on social or leisure activities was much smaller, and similar for all headache types (0.1 lost days). Overall impaired participation estimated from HY was 7.5% (Table 5).
Healthcare needs assessment
Table 6 shows the numbers of participants fulfilling one or more of our criteria for need for headache-related health care, and how, after correction for age and gender, these numbers translate into proportions of the general population.
Healthcare needs assessment.

*Age- and gender-corrected; 1of whom 318 also fulfilled criterion 2; 2of whom 582 also fulfilled criterion 2, 257 also fulfilled criterion 3, and 244 also fulfilled criteria 2 and 3; 3of whom 115 also fulfilled criterion 5. CI = confidence interval; pTIS = proportion of time in ictal state; TTH = tension type headache.
According to the criteria as originally set, well over half (57.5%) of the adult Pakistani population were assessed as having significant health loss and likely to benefit from health care. Migraine contributed 20.5% and H15+ contributed 8.2% to this assessment; however, TTH was by far the biggest contributor (28.9%) partly not only because of its high prevalence (44.6% (26)), but also because of the high levels of lost productivity attributed to it (Table 5). Removing the two criteria relating to TTH halved the number assessed as in need to 28.7% (Table 6).
Discussion
The present study provides additional data on attributed burden, as well as a healthcare needs assessment, to those obtained in our previous study reporting headache prevalence in Pakistan and showing that over three-quarters (76.1%) of adult aged 18–65 years in this populous Eastern Mediterranean country have an active headache disorder (26). In summary, these three-quarters of adults spend, on average, an estimated 6.4% of all their time with headache of, again on average, moderate intensity. Those with migraine are worse affected (more frequent, more severe and longer lasting headache) than those with TTH. Those with pMOH and those with other H15+ spend, respectively, 39.7% and 30.2% of their time with moderate-to-severe headache. These symptom burdens have inevitable consequences, with negative impacts on participation in life activities, on productivity measured in lost days from paid and household work, and on QoL. Measured at population level (including people with and without headache), pTIS according to two methods of estimation is 4.9–5.9%: in other words, 4.9–5.9% of all time in this population is spent with headache. Impaired participation across all domains of activity is 7.5% for all headache, according to estimates based on HY. Productivity losses are 3.1 lost days from paid work and 3.8 days from household work per three months (absolute losses from household work being greater than those from paid work for all headache types except TTH). Assessed need for headache-related health care (discussed below) appears to be very high.
In our sample, females reported higher headache-attributed burden than males, independently of higher prevalence (26). Females had more frequent, longer lasting and more intense headache than males, with much longer pTIS (8.5% vs. 3.8%). These findings were reflected in significantly longer duration of HY, but not greater intensity, while females with HY were more likely than males to achieve less than half or nothing yesterday. Lost productivity findings were influenced by relative participation in the labour force (32,33), of whom, at the time of data collection, only 21% were female (34), so that males, despite lesser headache-attributed burden, reported greater headache-attributed losses from paid work while females reported much greater losses from household work. Females also reported greater losses from social or leisure activities.
The two methods of calculating population-level pTIS, one based on recalled frequency and duration and the other on what happened yesterday with HY, gave reassuringly similar estimates (4.9% and 5.9%, respectively). Because of its high prevalence (8.2% (26)) and the high pTIS (>30%) associated with it at individual level, most of this time (3.1%) was spent with H15+. The contributions of migraine (0.9%) and TTH (0.7%) were considerably smaller, but neither was insubstantial (0.9% equates to 79 hours/year for every adult in the population of Pakistan). These estimates were according to recall because we did not diagnose headache type for HY (ICHD criteria are for headache disorders rather than individual attacks (30)).
Despite H15+ accounting for most population-level pTIS, and for the highest productivity losses at individual level, it was TTH that was associated with the greatest productivity losses at population level (1.5 lost days from paid work and 1.3 days from household work per three months), followed by migraine (1.1 and 1.4 days respectively). H15+ was some way behind (0.6 and 1.1 days, respectively). We can speculate on the reasons for this. First, coping strategies are less easily developed for the disruptive effects of occasional headache than for frequent and predictable headache. Second, with regard to paid work, people with H15+ may, as a direct consequence of high individual burden, choose less demanding work, or not be in employment at all. Third, with regard to both paid and household work, expectations (internal and external) about productivity may be lower among those with H15+ than among those with episodic headache. Our methods for assessing lost productivity do so against what each person had planned, not against objective standards, with possible built-in bias. Here, we note that HALT does not distinguish between absenteeism and presenteeism, although both are recorded when relevant, and given equal weight (28). The distinction is unimportant in the context of population-level burden: it is total productivity losses that inform health and economic policies. Furthermore, the distinction becomes artificial or meaningless in circumstances where work does not require presence during specified times: for those who are self-employed, with freedom to work whenever they wish; for those who are employed, but with flexibility to work from home; and with respect to household chores.
As for migraine and TTH, the latter had the greater impact on population-level productivity. This was surprising. At the individual level, migraine, on average, was more frequent, longer lasting and more intense than TTH (frequency being the principal driver of lost productivity (35)). Migraine was associated with lower self-reported QoL than TTH (or H15+). Nevertheless, lost productivity at individual level showed less than two-fold difference (Table 2), so that the very high prevalence of TTH (44.6% vs. 22.5% for migraine) was the determining factor.
It is clear that, in Pakistan at least, TTH should not be regarded as a non-disabling headache, a factor that had a major impact on our needs assessment. The very high proportion of the population found likely to benefit from health care (57.5%) was perhaps our most striking finding. At issue, therefore, were our criteria for need. We used the same criteria in our study in Saudi Arabia (also in EMR), assessing need in 35.8% of the population aged 18–65 years (21). That everyone with H15+ has need for health care is not open to question, but our other criteria might be considered arbitrary. As observed above, symptom burden and impaired participation data were somewhat skewed. This is always the case. Skewedness does not affect estimates of total population-level burden, which are based on means, but it does have an impact on who is considered to need health care. Among the episodic headaches, with a maximal frequency of 15 days/month, there is an upper limit on individual burden; but, below this, skewing is towards the low end of individual burden, which might be expected to leave only minorities with need for health care. However, a migraine frequency of 3–4 days/month is a recognized threshold for initiating preventative therapy (36), and this clearly requires medical care. The majority of those with migraine, pTIS > 3.3 and moderate-to-severe intensity also met this frequency criterion, such that changing this criterion would have little impact. However, removing TTH would reduce the proportion assessed as in need of care by half to 28.7%. Of interest, doing the same in Saudi Arabia would yield a similar proportion of 27.6% (21). Although our criteria regarding TTH reflected substantial burden (pTIS > 3.3% and moderate-to-severe intensity, and/or ≥3 lost days from paid or household work per three months), it can be argued that they indicate need not for medical care but for education, which might consist of no more than encouraging appropriate use of over-the-counter medications (36). It should be noted here that TTH did not include chronic TTH because any such cases would have been included among those with H15+.
Structured headache services, catering for migraine, TTH and H15+, have been proposed as the solution to headache (14), and shown to be cost-effective (15,16). Health education of the public is a pillar of these services, promoting appropriate usage by those who need them and effective self-care for those who do not (14). If these services were implemented in Pakistan, and supported by educational initiatives, it should be that no more than 30% of the adult population would need professional care. This is still a large proportion, but the expected health gains from effective care should be accompanied by productivity gains that greatly if not wholly offset the cost of efficiently provided professional care (14–16).
The strengths of the present study included the application of standardized and well-tested methodology (5,6), the use of the HARDSHIP questionnaire validated in Urdu in the target population (25), and a large sample (N = 4223) with a participating proportion of almost 90% and good matching of the nation's age, gender and habitation distributions. The last was despite that we could not sample from the urban slums or enter quite large areas of the country for security reasons (25). This was of course a limitation, in that we aimed for a nationwide study. However, it does not by any means invalidate the findings among those we did sample. The study was also limited, as are all retrospective observational studies, in its reliance on participants’ recall. However, we mitigated this by also collecting data on headache yesterday, requiring extremely short recall. In cross-sectional studies with a single encounter, H15+ cannot reliably be further diagnosed beyond recognizing its association (pMOH), or not (other H15+), with acute medication overuse (5,6). We made only one diagnosis per participant. Because migraine was more likely to be diagnosed when both migraine and TTH were present, TTH-attributed burden might have been somewhat underestimated. The original data were collected in 2010, but significant variations in prevalence are unlikely over the subsequent 15 years, and the succeeding iterations of GBD provide no evidence of variations other than those due to population growth and demographic shifts (1,12,13) (in Pakistan, gender distribution has remained very nearly constant between 2010 and 2023 (37,38)). The study applied diagnostic criteria from ICHD-2 (30), rather than the current ICHD-3 (3), but no material differences exist between these two versions of ICHD with respect to migraine, TTH or MOH.
In conclusion, the more than three-quarters of the adult Pakistani population (aged 18–65 years) with a headache disorder spend, on average, 6.4% of their total time with headache. There are associated losses in health, QoL, productivity and participation in social or leisure activities. Over half (57.5%) of this population appear to be in need of care, but health education promoting effective self-care might reduce this to <30% in need of professional care. The benefits in health gained from nationwide implementation of structured headache services, being cost-effective in themselves, should be accompanied by enhancements in productivity that would greatly offset the cost of providing these services.
Clinical implications
An estimated 4.9–5.9% of all time in Pakistan is spent with headache.
Calculated productivity losses attributed to headache per person (regardless of headache status) are 3.1 days lost from paid work and 3.8 days from household work over the course of three months.
Almost one third of the Pakistani population would be expected to benefit from professional headache care.
Footnotes
Acknowledgements
We are grateful to MA Shahab, U Javed and Rafiq Khanani, of Dow University of Health Sciences, Karachi Pakistan, for their assistance with the conduct of the study.
Author contributions
ADH and TJS conceived the study. TJS drafted the protocol and study questionnaire, which were subsequently refined by TJS and ADH in discussion. ADH provided supervision in Pakistan. AAH, AA, ULU, BA, JE and SZUA were responsible for conduct of the study in the field, with ADH acting as principal investigator. AKH carried out the statistical analysis. AKH and TJS drafted the manuscript. All authors reviewed and approved the final version of the manuscript submitted for publication.
Data availability
Data are held at Norwegian University of Science and Technology (NTNU), Trondheim, Norway. When analyses are completed, they will be available on request for academic purposes in accordance with the general policy of the Global Campaign against Headache.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The study was supported by Lifting The Burden, a United Kingdom-based non-governmental organization conducting the Global Campaign against Headache in official relations with the World Health Organization.
Ethical statement
The study was conducted in accordance with the Declaration of Helsinki and with approval from the Ethics Review Board of the Dow University of Health Sciences. All participants gave written consent prior to interview and had the option of discontinuing the interview at any time during it.