
Abstract
Abstract
Objective
This meta-analysis compared pressure pain sensitivity in trigeminal, cervical spine and remote pain-free areas between migraine patients and headache-free controls considering diagnosis (episodic versus chronic) and sex.
Results
Eighteen studies were included. Patients with migraine showed lower pressure pain thresholds than headache-free controls: trigeminal (MD −71.33 kPa, 95%CI −92.14 to −50.53), cervical spine (MD −68.50 kPa, 95%CI −84.67 to −52.33), and remote pain-free (MD −62.49 kPa, 95%CI −99.52 to −25.45) areas. Differences were consistently significant for episodic migraine in all locations, but only significant in the trigeminal area for chronic migraine (MD −67.36 kOPa, 95%CI −101.31 to −33.42). Overall, women had lower pressure pain thresholds than men. The methodological quality of most studies (66.7%) was good. The results showed a high heterogeneity.
Conclusion
This meta-analysis found low to high quality evidence showing lower pressure pain thresholds in trigeminal, extra-trigeminal, and remote pain-free areas in migraine sufferers when compared with headache-free controls. Hypersensitivity to pressure pain locally and widespread was consistently observed in episodic migraine, but locally in chronic migraine as compared to headache-free controls. Women with migraine were more sensitive than men.
Registration number: https://doi.org/10.17605/OSF.IO/YJTAK
Introduction
Headache is the most common painful condition attended by neurologists in clinical practice and it is associated with substantial cost (1). In fact, headache, particularly migraine, is the fourth/fifth most common reason for attending an emergency department annually (2). In the Global Burden Neurological Diseases Study, migraine was the third burdensome neurological disorder in the United States of America (USA) in terms of absolute number of years-lived with disability (3). The worldwide prevalence of migraine is estimated to be up to 11.6% (4).
Current hypotheses support the presence of different and complex mechanisms underlying pathogenesis of migraine (5). Sensitization and vascular/neural are the most accepted theories (5). The vascular/neural theory states that migraine is associated to a primary brain dysfunction with an impaired excitatory-inhibitory balance during cortical activity leading to sensitization of trigemino-vascular pain pathways (5). The sensitization theory proposes that the presence of long-lasting peripheral inputs could lead to activation of trigemino-cervical and central sensitization (6). A clinical manifestation of sensitization is the presence of hyperalgesia to pressure pain (7). Pressure pain thresholds (PPT), assessed with a pressure algometer, are commonly used to determine mechanical pain sensitivity of deep tissues (8). Hypersensitivity to pressure pain, i.e., lower PPTs, in individuals with migraine has been previously investigated in systematic reviews and meta-analyses. Two reviews concluded that PPTs were consistently lower within the trigeminal (9) and cervical (10) areas in migraine sufferers compared to headache-free subjects. The presence of pressure pain hyperalgesia in trigeminocervical areas is mainly related to peripheral mechanisms. To confirm the presence of central mechanisms, pressure pain hyperalgesia in remote pain-free areas is required. A posterior meta-analysis confirmed the presence of lower PPTs in local symptomatic areas but not in asymptomatic areas in migraine sufferers (11). Further, Nahman-Averbuch et al. (11) categorized the trigeminal and cervical areas as local, which did not permit differentiation between trigeminal or extra-trigeminal (but not remote area) sensitization. Additionally, neither review nor meta-analysis specifically differentiated between episodic and chronic migraine. This distinction seems to be highly relevant when considering sensitivity to pressure pain, since it has been observed lower PPTs in remote pain-free areas in individuals with chronic, but not episodic, tension-type headache (12). Therefore, the main objective of the current systematic review meta-analysis was to identify differences in PPT between individuals with migraine and headache-free controls differentiating between trigeminal, extra-trigeminal (cervical spine) and remote pain-free areas. As a secondary objective and as an expansion of the registration protocol, we also compared PPT considering the diagnosis (episodic vs. chronic) and sex (men vs. women).
Methods
This systematic review and metanalysis adheres to the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (13). The review was prospectively registered with the following international OPS Registry registration link: https://doi.org/10.17605/OSF.IO/YJTAK
Systematic literature search
Electronic literature searches were conducted on the following databases from their inception to 10 December 2021: MEDLINE, CINAHL, PubMed, SCOPUS and Web of Science databases. The reference lists of the papers identified in database searches were also screened and, authors were contacted for requesting missing info, if necessary. All database search strategies were conducted with the assistance of an experienced health science librarian.
Selection criteria
Cross-sectional or prospective case-control studies where at least one group included adults with any form of migraine and one headache-free control group were potentially included. The inclusion criteria were: 1, adults with a diagnosis of migraine according to IHS criteria (any edition); 2, full text report (not abstract, letter, or editorial) in an English language journal; 3, a control group including headache-free individuals; and 4, assessment of PPTs calculated with a pressure algometer. If a study evaluated different quantitative sensory tests, e.g., thermal or electrical pain thresholds, just PPTs measured with an algometer were extracted. The exclusion criteria included those studies: 1, not published as a full-text journal article; 2; assessing sensitivity to pressure pain with other modalities rather than pressure algometry (e.g., Von-Frey monofilament); or, 3, experimental pain models of migraine.
Screening, selection process and data extraction
Potential articles identified were independently reviewed by two authors (CFdlP, FCM). First, duplicates were removed. Second, title and abstract of the articles were screened. Third, a full-text read of eligible studies was conducted. A consensus on the included studies was required. If discrepancy existed, a third author (FAS) participated in the process to reach the consensus for inclusion/exclusion of the study.
Population, diagnosis, sample size, outcome, and type of algometer were extracted independently by two authors, again, in consensus on each item on the data-extraction. If disagreement occurred, a third author participated. No differences were observed in data extraction between both authors. Authors were contacted for requesting missing info, if necessary.
Assessment of risk of bias/methodological quality
The Newcastle-Ottawa Scale, a star rating system evaluating the methodological quality of case-control/cohort studies (18), was used to determine the risk of bias (RoB). This scale consists of three fields: case selection (4-items: case definition, representativeness of the cases, definition and selection of the controls), between-groups comparability (3-items: groups controlled for age, sex, or other factors) and exposure (2-items: blinding assessment and non-response rate). The maximum score is 9 stars where studies scoring ≥7 are considered of good quality; those scoring 5–6 are of fair quality; and those scoring 0–4 are of poor quality (19). Risk of bias was also evaluated by two authors (MNS, GPM), and differences discussed if needed. In case of disagreement, a third researcher arbitrated a consensus (DPRdS).
Level of evidence
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was used for determining the level of evidence (20). The level of evidence was classified as high, moderate, low or very low according to the presence or absence of the following items: 1, risk of bias (Newcastle-Ottawa Scale), when several studies showed substantial risk of bias; 2, inconsistency of the results/unexplained heterogeneity, when those statistically significant results showed moderate to high heterogeneity (I2 > 60%); 3, indirectness of evidence, when evidence was not directly comparable to the question of interest (e. g., population, exposure, comparator, outcome); 4, imprecision of the results, when the studies included few participants and few events (wide confidence intervals); and, 5, probability of publication bias, if the funnel plot presented substantial asymmetry and statistically significant Egger Test (21). The level of evidence was classified as high when all items were negative; moderate when one item included serious risk; low when two items showed serious risk or one item showed very serious risk; very low when all items had serious risk or two or more items showed very serious risk.
Data synthesis and analysis
The Review Manager statistical software (RevMan version 5.3) and the R software 4.0.0 were used for conducting the meta-analysis. Data synthesis was categorized by the diagnosis (chronic or episodic migraine) and by sex (men or women).
Sample size, means and standard deviations were extracted for each PPT. When standard errors were provided, they were converted to standard deviations. Non-parametric data, if provided, were also converted to means and standard deviations (22). Means and standard deviations were estimated from graphs with the GetData Graph Digitizer v.2.26.0.20 software, if needed. Eventually, if a study reported mean differences with their interval confidence or standard errors, standard deviations were also estimated, as needed.
Mean and standard deviation values of every point (trigeminal, cervical spine, and remote pain-free) were obtained using dmtar package for R software and pool. groups function. When the data of different groups (men/women) was presented separately, pool. groups function was used to calculate the mean and standard deviation of the total sample. The between-groups mean differences with their 95% confidence intervals (CI) of each study were obtained. A random-effect model was used to determine the overall effect size (MD). Pressure pain thresholds are expressed in kPa, when another unit was presented in (e.g., kg), they were converted to kPa.
Data extracted from the articles are summarized in tables (see results section). If multiple sites were analyzed in the same region, e.g., temporalis, masseter, or frontalis for the head, the average of all PPTs on each area (trigeminal, cervical spine, or remote pain-free) was calculated. Additionally, absolute mean PPTs for each area (trigeminal, cervical spine, remote pain-free) were pooled regardless of the location and compared between patients and headache-free controls. When results are presented by subgroups (episodic/chronic, men/women), each subgroup was separately treated. In those studies with a single headache-free control group but different patient subtypes, we pooled data from each group of patients vs. the same control group. Due to the low number of studies and participants directly comparing episodic versus chronic migraine, we did no pool for this comparison.
The heterogeneity of the studies was assessed using the I2 statistic considering the Cochrane group interpretation: 0%–40% no relevant/important heterogeneity; 30%–60% moderate heterogeneity, 50%–90% substantial heterogeneity, and 75–100% considerable heterogeneity (23). Publication bias was assessed using a funnel plot, if there was asymmetry and suspicion of publication bias, Egger’s Test was realized to detect publication bias. The assessment of publication bias was evaluated if 10 different studies were included in the same meta-analysis.
Results
Study selection
The electronic search initially identified 1,946 potential studies for review. After removing duplicates, 879 studies remained. Seven hundred and nine (n = 709) studies were excluded based on examination of their title, whereas 141 were excluded based on their abstract, leaving 29 articles for full-text analysis. Twelve studies were excluded, leaving a total of 18 studies (24–41) to be included in the review and meta-analysis (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow diagram.
Study characteristics
The characteristics of the populations of the included studies are shown in Table 1. All articles diagnosed the group of patients with migraine according to the IHS criteria (n = 4, first edition 1988; n = 9 second edition 2004; n = 4 third edition beta version 2013, n = 1 third edition 2018). Five articles (25–27,32,38) included patients with chronic migraine, 8 articles (24,25,27,31,36,37,39,40) patients with episodic migraine, and the remaining 5 (26,30,33–35) did not differentiate between episodic/chronic migraine. Seven studies included women with migraine (25,27,28,30,33,36,40), and the remaining eleven included both gender (24,26,29,31,32,34,35,37–39,41). The total sample included 835 patients (135 men, 700 women) and 664 headache-free controls (178 men, 486 women). Two hundred and forty-five (n = 245) were patients with chronic migraine (28 men, 217 women), 303 with episodic migraine (59 men, 244 women) and 287 (48 men, 239 women) individuals with migraine without differentiation. All studies included a comparable headache-free group, but only in six studies was this control group mentioned to be matched (24,26,27,31,38,40). In six (33%) studies (24,25,28–30,34), patients were asked not to take analgesic medication 24h or longer before examination. Few articles mentioned prophylactic treatment, but overall, there was insufficient data on medication. Most studies evaluated patients in headache-free periods (inter-ictal phase) or when headache intensity was less than 3/10 (in those with high frequency of headache).
Characteristics of the population and algometer of the included studies.
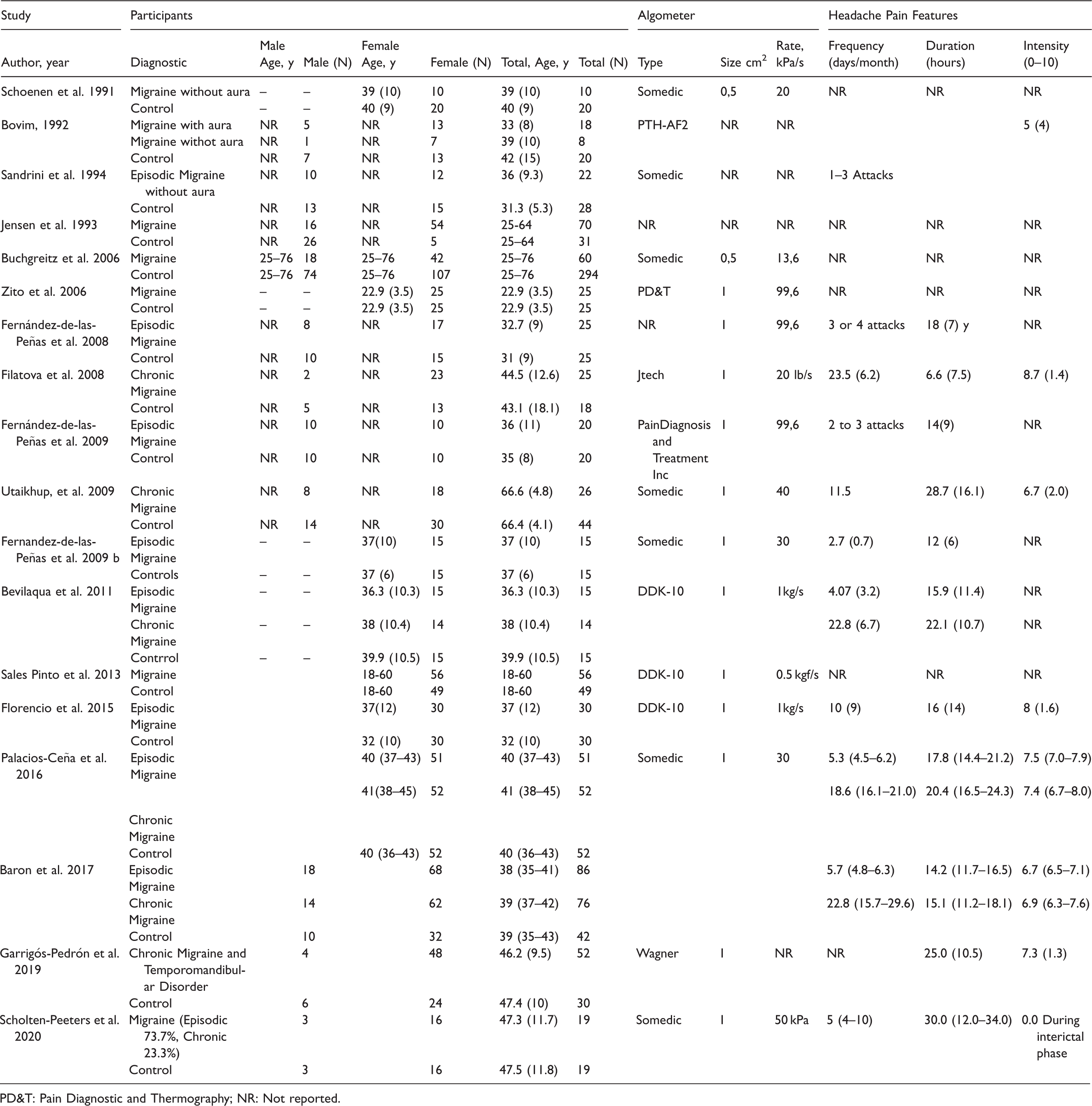
PD&T: Pain Diagnostic and Thermography; NR: Not reported.
The pressure algometer used in seven studies (41.2%) was from the company Somedic© (Sweden). The size of the algometer probe surface was reported in 14 (82.4%) studies and ranged from 0.5 (n = 2) to 1cm2 (n = 12). Pressure pain thresholds were assessed in trigeminal-related areas in 15 studies (temporalis n = 11, frontalis n = 4, parietal bone n = 2, masseter n = 3), in the cervical spine in 9 studies (upper trapezius n = 5, neck n = 2), and in remote pain-free areas in seven (tibialis anterior/Achilles tendon n = 3, hand/finger n = 2 and peripheral nerves n = 1). Supplementary Table summarizes PPT findings of the included studies on each point.
Risk of bias/methodological quality
The methodological quality scores ranged from 4 to 8 (mean: 6.6, SD: 1.4) out of a maximum of 9. Three studies were considered of poor quality (4 stars) (28–30), three of fair methodological quality (5–6 stars) (24,34,35), and the remaining twelve of good quality (7–8 stars) (25–27,30,32,33,36–41). The most frequent biases were lack of control for additional factors as psychological aspects (e.g., anxiety/depression) or ascertainment of exposure (blinding assessment). Differences in scores between reviewers were discussed and solved properly (overall agreement of 97%), therefore, arbitration was not needed. Table 2 summarizes the Newcastle-Ottawa Scale on each study and a summary of every item.
Newcastle – Ottawa Quality Assessment Scale evaluating Methodological Quality/Risk of Bias.

Pressure pain thresholds between migraine patients and controls
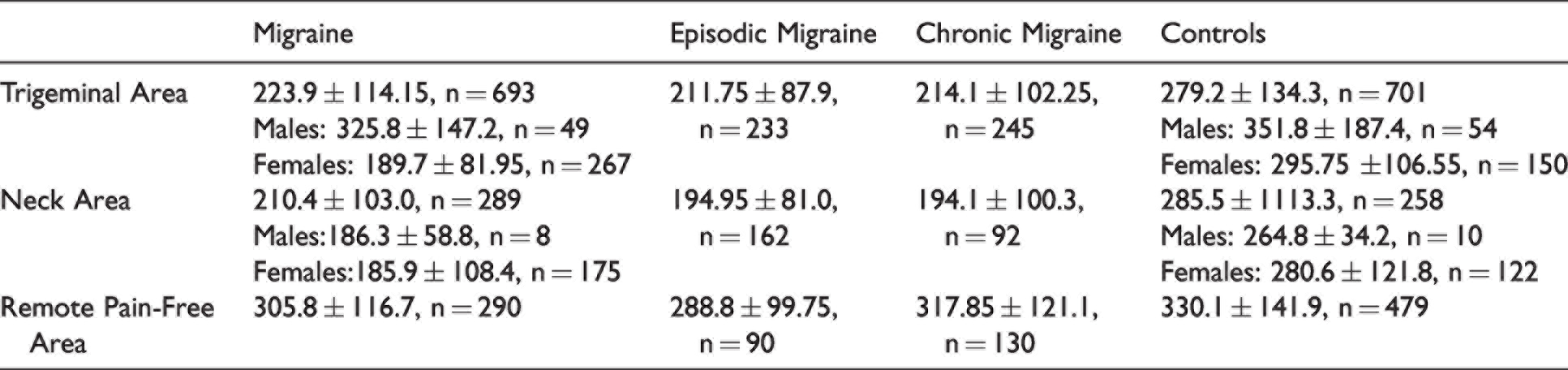
The pooled data of all PPTs revealed, in general, that individuals with migraine exhibited lower values (mean ± SD, kPa) than headache-free controls at trigeminal, neck and remote pain-free areas (Table 3).
Pressure pain thresholds (pooled means ± SD, KPa) in trigeminal, extra-trigeminal and remote pain-free areas in adults with migraine and headache-free controls.
The meta-analysis found overall that patients with migraine exhibited significant reduced PPTs at the head (MD −71.33, 95%CI −92.14 to −50.53, Z = 6.72, P < 0.001, Figure 2), the cervical spine (MD −68.50, 95%CI −84.67 to −52.33, Z = 8.30, P < 0.001, Figure 3) and remote pain-free (MD −62.49, 95%CI −99.52 to −25.45, Z = 3.31, P < 0.001, Figure 4) areas with high heterogeneity (I2 > 75%) between studies in most meta-analyses. The funnel plot did not show asymmetry in overall PPTs at the trigeminal area (Supplementary Figure) with a non-significant Egger’s test (intercept: 0.314, P = 0.845); therefore, no publication bias was observed in this meta-analysis.

Summary of forest plot results for meta-analyses of PPTs in the trigeminal area by chronicity. Negative values indicate that migraine patients < controls. Lower PPTs were found in both patients with episodic and chronic migraine when compared with headache-free controls.

Summary of forest plot results for meta-analyses of PPTs in the cervical spine by chronicity. Negative values indicate that migraine patients < controls. Lower PPTs were found in episodic, but not chronic, migraine patients when compared with headache-free controls.

Summary of forest plot results for meta-analyses of PPTs in remote pain-free areas by chronicity. Negative values indicate that migraine patients < controls. Lower PPTs were found in episodic, but not chronic, migraine patients when compared with headache-free controls.
Pressure pain thresholds according to migraine diagnosis
Secondary analyses revealed that patients with episodic migraine showed consistently lower PPT at the head (MD −81.30, 95%CI −96.11 to −66.49, I2 = 21%, Figure 2), the cervical spine (MD −77.95, 95%CI −92.88 to −63.02, I2 = 0%, Figure 3) and remote pain-free (MD: −92.82, 95%CI −116.92 to −68.71, I2 = 0%, Figure 4) areas when compared to healthy controls, whereas subjects with chronic migraine exhibited lower PPTs just at the head (MD −67.36, 95%CI −101.31 to −33.42, I2 = 80%, Figure 2), but not at the cervical spine (Figure 3) or remote pain-free areas when compared to healthy controls (Figure 4).
Pressure pain thresholds by sex
Women with migraine exhibited lower PPT at the trigeminal area (MD −82.07, 95%CI −125.98 to −38.15, Z = 3.66, P < 0.001, I2 = 89%, Figure 5) and the cervical spine (MD −88.54, 95%CI −105.88 to −71.20, Z = 10.01, P < 0.001, I2 = 0%, Figure 6) as compared with headache-free women (Table 3). Differences between males with migraine and headache-free controls were significant for the cervical spine (MD −78.45, 95%CI −125.91 to −30.99, Z = 3.24, P = 0.001, I2 = N/A), but not for the trigeminal area: MD −46.47, 95%CI −113.73 to 20.79, Z = 1.35, P = 0.18, I2 = 59%). However, cervical spine results were based on just one paper (37).
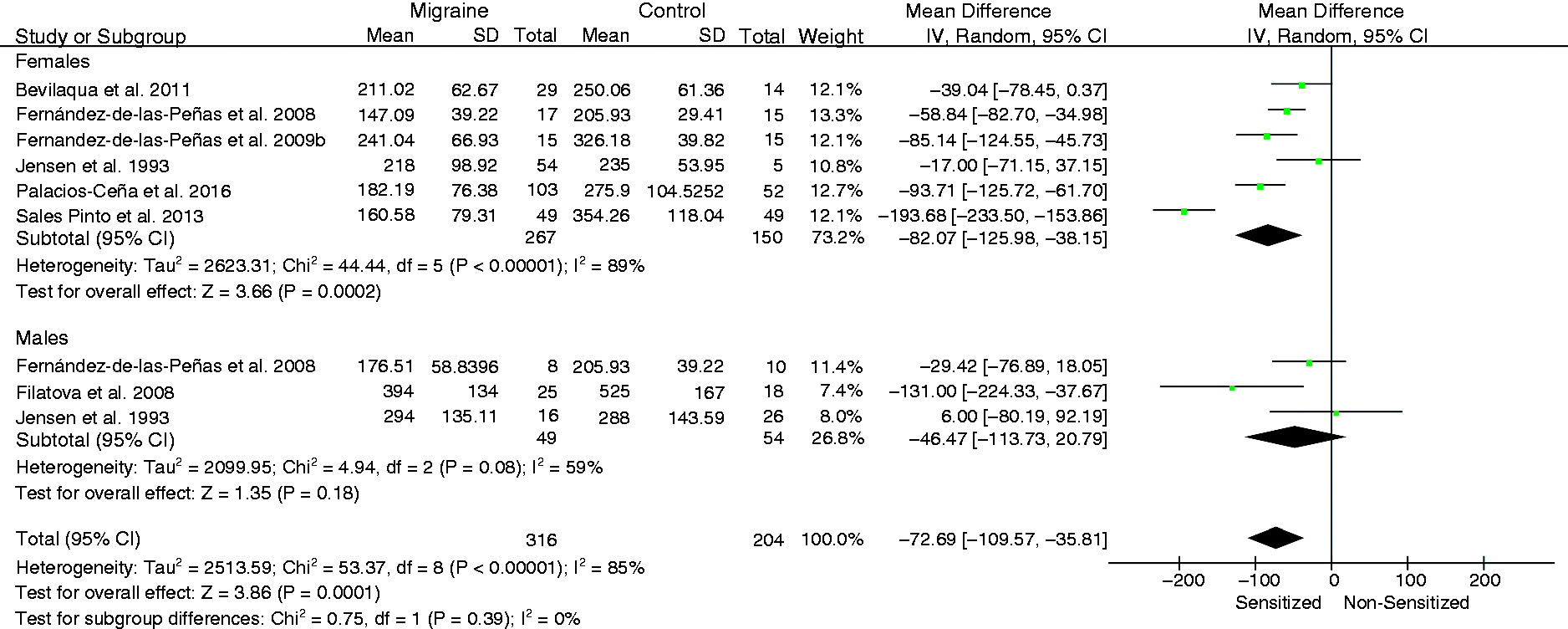
Summary of forest plot results for meta-analyses of PPTs in the trigeminal area by gender. Negative values indicate that migraine patients < controls. Lower PPTs were found in women, but not men, with migraine compared with headache-free women.

Summary of forest plot results for meta-analyses of PPTs in the cervical spine by gender. Negative values indicate that migraine patients < controls. Lower PPTs were found in women and men with migraine compared with headache-free women or men, respectively. Note: Men comparison was based on just one study.
Level of evidence
The GRADE assessment showing Risk of Bias (RoB), inconsistency of the results, indirectness of evidence, imprecision of results, and high probability of publication bias is shown at Table 4. In general, the inconsistency of the results downgraded one or low levels the evidence quality leading to low evidence in several pooled data.
GRADE evidence profile for differences in pressure pain thresholds between headache patients and controls.

#Statistically significant.
Discussion
To our knowledge this is the first meta-analysis conducted to date analyzing differences in PPT between patients with migraine and headache-free controls considering the diagnosis of migraine (chronic or episodic) and sex. The results found low-quality evidence for lower PPTs in the trigeminal and remote pain-free areas between migraine sufferers and headache-free controls, and high-quality evidence for lower PPTs in the cervical spine. Sensitivity to pressure pain was consistently higher and more widespread (moderate to high evidence) in individuals with episodic migraine, and localized in those with chronic migraine, when compared to headache-free controls. In general, women exhibited lowers PPTs than men.
Findings
We identified 18 studies of fair to good methodological quality assessing pressure pain sensitivity in migraine. Overall, pooled data found lower PPTs within the trigeminal (head), extra-trigeminal (cervical spine) and distant pain-free areas in migraineurs when compared to headache-free controls. Current results are in line previous systematic review and meta-analyses showing that patients with migraine exhibit reduced PPT scores in the craniofacial and cervical musculature (9–11). Andersen et al. (9) reported PPTs in the temporalis muscle of 231.26 ± 38.3 kPa for migraine sufferers, values similar to those pooled for the head in our meta-analysis (mean: 223.9 ± 114.15, n = 693). Similarly, Castien et al. (10) reported a pooled mean difference of −55.75kPa (95%CI −79.80 to 31.70) in people with migraine again similar to our data (MD −68.50, 95%CI −84.67 to −52.33). Nahman-Averbuch et al. (11) provided effect sizes, but not mean differences, so comparison between results was not possible.
An important topic to discuss is to determine if differences between patients with migraine and controls represent pressure pain hyperalgesia and should be considered as clinically relevant. Romero-Morales et al. (42) reported that differences of 16.2kPa and 78.9 kPa in the head and neck could be considered as the minimal clinically relevant difference in people with headaches, respectively. In healthy people, Walton et al. (43) proposed a change of 42.7 kPa for the neck and of 86.3kPa for the tibialis anterior as the minimal detectable changes. Our pooled estimates were larger than these values for the head and neck areas, but lower for remote pain-free areas, supporting the presence of real differences (larger than test error) between migraine patients and healthy controls in the trigeminocervical region. In fact, Andersen et al. (9) determined that 230kPa should be considered as the cut-off score for PPTs at the head to determine the presence of sensitization and a risk for the promotion of headaches. These results support the presence of pressure pain hyperalgesia in the trigeminocervical area in people with migraine as previously suggested (9–11).
Previous meta-analyses did not differentiate between episodic or chronic migraine. The current meta-analysis is the first one providing data of PPT differences differentiating between the episodic and chronic forms of migraine. Our results reported that individuals with episodic migraine showed lower PPTs in the head, cervical spine, and remote pain-free areas, whereas individuals with chronic migraine showed decreased PPTs just in the head, but not in the cervical spine or remote pain-free areas when compared with controls. Current results support the presence of trigeminal sensitization in both groups of migraine patients, and the presence of trigeminocervical and widespread sensitization in episodic, but not chronic, migraine. These results were unexpected, since chronic headaches are usually associated to central mechanisms in a greater extent than their episodic forms. In fact, the presence of more generalized hyperalgesia in tension-type headache is present on its chronic, but not on its episodic, form (12). Nevertheless, the lack of information related to migraine features in several studies does not allow us to determine the frequency of the headaches and properly classify migraineurs. In addition, the number of studies analyzing PPTs in remote pain-free areas was small and we cannot exclude that lack of findings in the chronic form was not merely due to low power (type II error). This type I error would agree with the results by Palacios-Ceña et al. (27) where no differences in widespread PPTs were observed between women with episodic or chronic migraine. Nevertheless, it should be considered that this meta-analysis did not compare episodic versus chronic migraine, since the number of studies and the number of participants were extremely small. Finally, it has been also suggested that the impairments in nociceptive gain processing in migraine could be more modality specific, i.e., heat or electrical, than in other primary headaches such as tension-type headache.
We also observed that women showed lower PPTs than men in the trigeminal area regardless of the presence or absence of migraine. No sex differences in the cervical spine or remote pain-free areas could be calculated due to the lack of studies including men with migraine. The presence of higher hyperalgesic mechanical responses in women is consistent in the literature and is in line with higher responsiveness to nociceptive stimuli associated to biological, hormonal or biopsychosocial factors (44,45). An interesting finding was that differences between migraineurs and headache-free controls in the trigeminal area were more consistent in women than in men, which deserves further research. Future studies investigating PPTs in individuals with migraine should include large sample sizes and differentiate by sex to further confirm current results, since we were not able to pool PPTs by sex in most locations.
Strengths and limitations
The rigorous methodology applied for literature search, study selection, screening for eligibility, assessment of risk of bias, and pooling analysis of data were different strengths of the current meta-analysis. We identified a total of 18 studies, a greater number than those previously included in published reviews (9,10). In fact, several studies included in our review fulfilled recommendations provided by Andersen et al. (9) for assessment of pressure algometry: an algometer probe size of 1 cm2, using the mean score of three consecutive assessments and control groups comparable by age.
Nevertheless, this review also exhibits some limitations. First, we could not conduct a meta-regression due to the high heterogeneity between the studies. Second, the lack of data of headache features in several studies may influence the result. Although all studies applied ICHD criteria, not all studies clearly reported the severity/frequency of migraine attacks and consecutiveness of patients. Third, the number of studies investigating PPT separately in women and men was limited and most studies did not control the menstrual phase in women, a topic recently discussed (46). Accordingly, current PPTs stratified by sex should be considered with caution. Similarly, the effect of medication on pressure pain sensitivity was not considered in any of the studies included. Fourth, we pooled distant pain-free areas independently of the anatomical site (hand, wrist or tibialis anterior) due to the small number of studies. Although PPT could be different between upper and lower extremity area, the between-groups comparison between patients and controls would not be altered the direction of the results. Finally, only articles published in English were included, but because the majority of available articles are in English, this probably did not a major impact on the overall findings.
Clinical and research implications
The current meta-analysis highlights the importance of pressure pain hyperalgesia in people with migraine as manifestation of sensitization and opens several questions for future research. First, it has been found that lower PPTs predict future pain and disability in musculoskeletal pain (47); therefore, early identification of individuals with migraine with higher sensitization may help to reduce the possibility of chronicity. Second, standardized protocols for PPT assessment would permit better characterization of differences between primary headaches and headache-free subjects. This is highly important considering that PPT assessment should be migraine phase-specific since mechanical hyperalgesia and/or allodynia is dynamic and starts to decrease when the migraine attack starts (the ictal phase), falls to its maximum decrease during the migraine attack, and gradually increases after the attack (post-ictal phase) until the potential next attack (post-migraine cutaneous allodynia or hyperalgesia) (48). In fact, most studies included in this meta-analysis did not differentiate between the migraine-phases. Finally, better study designs providing PPTs separately by sex and by clearly differentiating the frequency of migraine attacks (chronic or episodic) and including both subgroups of migraineurs are needed to obtain more solid and robust conclusions.
Conclusions
This meta-analysis found low to high quality evidence showing lower PPT scores in trigeminal (head), extra-trigeminal (cervical spine) and remote pain-free areas in people with migraine when compared with headache-free controls. Hypersensitivity to pressure pain locally and widespread was consistently found in episodic migraine, but just locally in chronic migraine as compared to headache-free controls. Women with migraine seem to be more sensitive than men.
Key findings
The current meta-analysis found low to high quality evidence supporting pressure pain hyperalgesia in migraine patients in comparison with controls. Patients with episodic migraine exhibited localized and widespread hypersensitivity to pressure pain in comparison with controls. Patients with chronic migraine exhibited localized, but not widespread hypersensitivity to pressure pain in comparison with controls.
Supplemental Material
sj-jpg-1-cep-10.1177_03331024221084217 - Supplemental material for Localized and widespread pressure pain hypersensitivity in patients with episodic or chronic migraine: A systematic review and meta-analysis
Supplemental material, sj-jpg-1-cep-10.1177_03331024221084217 for Localized and widespread pressure pain hypersensitivity in patients with episodic or chronic migraine: A systematic review and meta-analysis by César Fernández-de-las-Peñas, Marcos J Navarro-Santana, Francisca Curiel-Montero, Gustavo Plaza-Manzano, Francisco Alburquerque-Sendín and Daiana P Rodrigues-de-Souza in Cephalalgia
Supplemental Material
sj-pdf-2-cep-10.1177_03331024221084217 - Supplemental material for Localized and widespread pressure pain hypersensitivity in patients with episodic or chronic migraine: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-cep-10.1177_03331024221084217 for Localized and widespread pressure pain hypersensitivity in patients with episodic or chronic migraine: A systematic review and meta-analysis by César Fernández-de-las-Peñas, Marcos J Navarro-Santana, Francisca Curiel-Montero, Gustavo Plaza-Manzano, Francisco Alburquerque-Sendín and Daiana P Rodrigues-de-Souza in Cephalalgia
Supplemental Material
sj-pdf-3-cep-10.1177_03331024221084217 - Supplemental material for Localized and widespread pressure pain hypersensitivity in patients with episodic or chronic migraine: A systematic review and meta-analysis
Supplemental material, sj-pdf-3-cep-10.1177_03331024221084217 for Localized and widespread pressure pain hypersensitivity in patients with episodic or chronic migraine: A systematic review and meta-analysis by César Fernández-de-las-Peñas, Marcos J Navarro-Santana, Francisca Curiel-Montero, Gustavo Plaza-Manzano, Francisco Alburquerque-Sendín and Daiana P Rodrigues-de-Souza in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.