
Abstract
Thirty-three migraineurs and 23 healthy controls were submitted to pressure algometry before and after light-induced discomfort was elicited by progressive light stimulation in a monoblind fashion. Pressure algometries were performed on the emergence of the supraorbital, infraorbital, mental and greater occipital nerves, and over the temporal muscles, always throughout the same sequence and from right to left. Measurements were carried out before and immediately after light stimulation and after 10 min of the second algometry. The final result for each site measured at each time-point was the mean of the three measurements. Light stimulation was carried out progressively until light-induced discomfort was reported, to a maximum of 20 000 lux. A heat-blocking glass protected patients' eyes. Migraineurs presented significant and persistent drops in pain perception thresholds after light stimulation, at all sites tested (P = 0.002 to < 0.0001). These drops were not seen in controls, in whom, conversely, a less significant increase was seen on right infraorbital and left temporal muscle sites. Our results indicate that in migraineurs, light may have a relevant role in trigeminal and cervical pain perception thresholds.
Introduction
Photophobia is defined as a painful sensation secondary to the exposure of the eyes to light, usually associated with blepharospasm and lacrimation (1). Discomfort to light has been reported in five conditions: (a) diseases of the anterior aspect of the eye; (b) diseases of the vitreous and/or the retina; (c) acquired optic neuritis; (d) after trauma, surgery, or intracranial inflammation or infection; and (e) individual sensitivity to light (2). However, it seems that environmental light is the main precipitating factor, since photophobia is highly reduced at night or in the darkness (1).
In migraine, photophobia is a frequent complaint, being reported by 66–88% of patients (3). Indeed, photophobia is included in the International Headache Society diagnostic criteria for migraine (4). In migraineurs, light stimuli may result in several symptoms, from mild discomfort limited to the eyes to triggering or aggravating migraine attacks. Even between migraine attacks, migraineurs reported more light–induced discomfort than normal individuals (3, 5, 6). During migraine attacks, phonophobia and osmophobia are frequently reported to be associated with photophobia, probably due to an enhanced cortical excitability. It has been suggested that migraineurs have lower sensorial thresholds, due to lower inhibitory activity (5). However, the way light stimulation increases migraine pain is a question that has remained to be answered.
This study aims to determine the influence of light stimulation on trigeminal and cervical pain perception thresholds, measured by pressure algometry, by comparing the changes on these thresholds before and after light stimulation of migraineurs, with those of normal controls.
Methods
Two groups of individuals were selected from the Hospital de Clínicas personnel: a group of migraineurs, selected according to the IHS criteria, and a control group of healthy volunteers. Exclusion criteria consisted of major visual abnormalities, epilepsy, pain syndromes other than migraine, or a migraine attack in the preceding 48 h. Individuals taking a drug known to have prophylactic effects on migraine were also excluded. All the individuals were advised not to smoke, drink coffee or take spirits in the 6 hours preceding the examination. The control group was composed of 18 females and five males, with a mean age of 32.1 years. Three subjects of the control group were blue-eyed, and three were green-eyed. Of the migraineurs, 30 were females and three males. Three migraineurs had migraine with visual aura. The mean age of the migraineurs was 35.3 years. One subject of the migraine group was blue-eyed, and five were green-eyed.
Migraineurs and controls were examined by an investigator blind to their condition. After a physical and neurological examination they were submitted to an algometric procedure on selected trigeminal cervical sites. Algometry was carried out with a Somedic Sales AB pressure algometer. Pain perception thresholds were measured bilaterally over the emergence of the three trigeminal branches, and over the temporal muscles and greater occipital nerves, always in the same sequence and beginning on the right side of the head. The complete procedure was conducted three times, and for each site the mean of the three algometric measurements was considered as the final result.
The individuals were then submitted to progressive light stimulation, by means of a specially built electronic dimmer controlled by a computer, through a method similar to that described by Vanagaite et al. (3). Light stimuli lasting 2 s, starting at 50 lux, had their intensity increased at a rate of 30 lux, with 2 s, light-free intervals separating each stimulus from the next. The highest light intensity achieved by our equipment was 20000 lux. To avoid lesions of the cornea, a heat filtering barrier, consisting of two framed 40 cm × 40 cm pieces of 6 mm thick TotalGlass® (Blindex), separated by a 12-mm thick air chamber, was interposed between the light source (25 cm distant) and the eyes of the individuals being tested (40 cm distant).
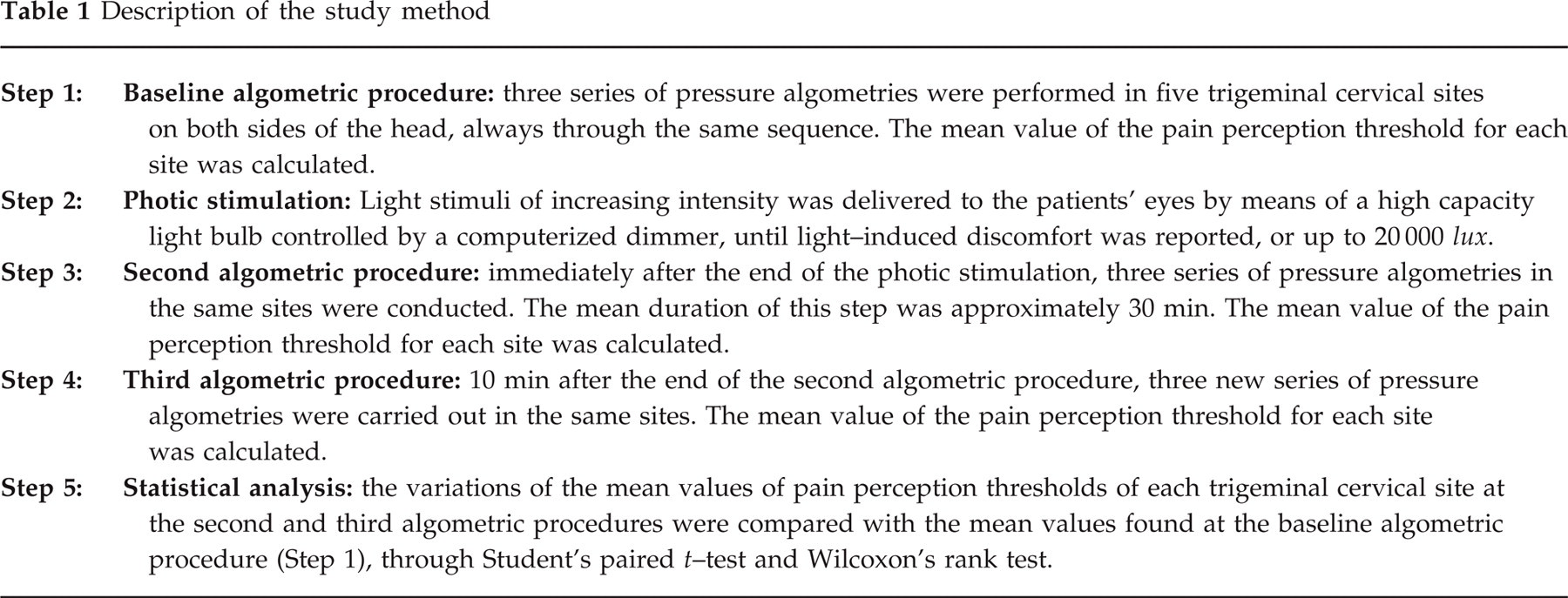
Light stimulation was interrupted when light-induced discomfort was reported, and then the tested individuals were again submitted to two complete algometric procedures: one immediately after light stimulation was discontinued, and the other 10 min after the end of the second series of algometric procedures. Table 1 summarizes the method. Variations in pain perception thresholds were analysed through Student's paired t-test and Wilcoxon's rank test, the later being used for those results with higher dispersion rates. The study was approved by the Ethics Committee for Human Research of the Hospital de Clínicas, and all the examined individuals were asked to read and sign an informed consent form prior to their inclusion.
Description of the study method
Results
Only five of the healthy volunteers tolerated light stimulation at 20000 lux without reporting light-induced discomfort. In migraineurs, light-induced discomfort was obtained at lower light intensities (mean 1747 lux, median 680 lux) compared with normal controls (mean 6429, median 2510) (P < 0.0001). Blue-eyed and green-eyed controls and migraineurs reported light-induced discomfort at lower light intensities (median 2069 lux and 929 lux, respectively) than dark-eyed subjects (median 7964 lux and 1929 lux, respectively) but these differences did not influence the results.
Migraineurs, after light-induced discomfort, presented a significant and sustained lowering of pain perception thresholds at all tested trigeminal cervical sites (Table 2). In the control group, a lowering of pain perception thresholds was not seen, but there was conversely a tendency of those thresholds to increase, significant only in the measurements at the right infraorbital and the left temporal sites (P = 0.003 and 0.002, respectively, Table 3). In fact, the significance of the increase in pain perception thresholds observed in the healthy volunteers was smaller than that of the reduction seen in the migraineurs. The results of both groups were further re–analysed, considering individuals above and below the median lux reported to trigger light-induced discomfort in each group, with a gating effect of higher light intensities being excluded.

Kilopascals per second;
each site was tested three times at each assessment;
Student's paired t-test;
Wilcoxon's rank test.

Kilopascals per second;
each site was tested three times at each assessment;
Student's paired t–test;
Wilcoxon's rank test.
A single migraine patient developed a severe retro-orbital non-migrainous headache after light stimulation, which resolved after a few minutes.
Discussion
Although visual symptoms associated with migraine attacks are a common complaint of migraineurs, their pathophysiology remains unclear. At the beginning of the century, accomodation disorders were hypothesized to cause migraine, and their correction to resolve it (7). Asthenopia is considered to be a symptom related to defective accomodation, secondary to the efforts to improve vision. They include a mild, dull pain around or behind the eyes, a sensation of tiredness, heat, soreness, or of an intraocular foreign body. These sensations are reported sometimes to project over the forehead, to the temporal areas, or to be associated with tearing (2). A higher sensitivity to light is a common complaint of patients with chronic headaches, being reported between the attacks by 44.7% of the patients, and by 71.3% of them during the headache episodes (8). In migraineurs, an increased sensibility to light is reported by 83.2% of the patients (9).
In migraineurs, visual symptoms may be classified as specific and non-specific. Specific symptoms consist of the several types of visual migraine aura. Non-specific symptoms consist of glare, characterized by an increased sensitivity to light, manifested by the perception of brightness, visual blurring, and/or visual discomfort (5), and photophobia, a painful sensation to light stimuli, frequently associated with tearing and blepharospasm (1). Several authors have discussed the increased sensitivity of migraineurs to light (3, 5, 6, 8, 10, 11). Although its exact mechanism remains unknown, it is presumed to involve the trigeminal cervical system, the visual pathways and the pupillary pathways (5, 6, 12). Indeed, non-senile miosis can be appreciated in migraineurs during a migraine attack, when compared with healthy controls (12–14).
Compression of the sympathetic fibers by an oedematous carotid and/or a central aminergic compromise are some of the hypotheses given to explain this finding (12). Drummond also suggested that the changes in extracranial vasculature and in the ocular sympathetic function seen in migraine attacks are secondary to activation of trigeminalvascular reflexes, to antidromic transmission, and to the release of vasoactive peptides in trigeminal nerve terminals (15). It is known that the release of substance P and of calcitonin gene-related peptide (CGRP) in nerve terminals at the anterior uvea result in myosis (16, 17). Stimulation of the infratroclear nerve can produce haematropin-resistant myosis, suggesting a non-cholinergic drive (18), or an inbalance between parasympathetic and sympathetic drives. It is also known that light stimulation may increase adrenaline and decrease noradrenaline urinary excretion (19), an effect blocked by the administration of propranolol and amitryptiline (20), medications known to be effective in migraine prophylaxis.
When exposed to light stimulation, migraineurs report more visual discomfort, even during interictal periods (3). Thermal or mechanical stimulation of the supraorbital nerve was reported to increase light-induced visual discomfort, suggesting that trigeminal afferences may contribute to the mechanisms of glare and photophobia in migraineurs (10). Vanagaite et al. (3) have reported migraineurs to be more sensitive to light stimulation than controls, and that their light-induced visual discomfort thresholds diminished after repeated stimulation, a finding suggestive of a defective adaptation to light and to repetitive or increased light stimulation afferences, leading to fatigue of the CNS and to an increased sensitivity to light (3). Curiously, photophobia has been reported in children who were visually impaired by lesions of the occipital cortex, a finding that suggests a subcortical mechanism for visual discomfort (21). The report of dazzle secondary to lesions at the thalamus and at brainstem nuclei (1, 22) reinforces this view.
Wray et al. (23) reported that migraineurs with aura perform better than controls in tests of pre-cortical visual processing. This difference was not seen in cortical visual processing tests, a finding that suggested an increased sensitivity of the pre-cortical visual mechanisms. These observations reinforce the current views that migraine-related glare may be secondary to a hyperexcitable sensorial system, and migraine-related photophobia to the activation of the trigeminal pathways (10). Indeed, Vanagaite et al. (3) postulate that a convergence of visual and trigeminal afferences may occur at the thalamus, probably beginning at the lateral geniculated body, since repetitive monocular light stimulation could induce binocular photophobia. Anatomical correlates of these considerations are the facts that trigeminal nuclei project to the ipsilateral thalamus, and that thalamic lesions may cause severe dazzle (1). However, since in migraine photophobia is usually associated with phonophobia and osmophobia, a dysfunction of inhibitory systems has also been postulated (24).
During our experiment, although individuals were submitted to progressive light stimulation up to the occurrence of light-induced discomfort, no individual reported visual pain. As described in previous reports (3), light-induced discomfort thresholds were lower in migraineurs than in controls. The persistent drop in pain perception thresholds seen in migraineurs reinforces the influence of visual afferences on trigeminal cervical nociception, posing a further challenge to clarify the relevance of its role in the migraine process.
Footnotes
Acknowledgements
The authors express their thanks to Dr Jolanta Vanagaite and especially to Eng. Ole Storen, for their help in clarifying doubts regarding the method; to Mr Nelson Torres, for his review of the language; and to Mr Ricardo Antunes de Macedo, of Engevidros, for providing us with the TotalGlass® sample needed for the study. The algometer was donated by Libbs Farmacêutica. The project, coded Banpesq 98005263, was supported by a PIBIC/CNPq Grant to Dr Tatsui, sponsored by the Conselho Nacional de Pesquisa (CNPq).