
Abstract
Background
This systematic review assesses the effectiveness of physiotherapy on headache parameters and quality of life of patients with tension-type headache using network meta-analysis.
Methods
A systematic search was conducted in the databases Web of Science, Medline, Cochrane Library and Physiotherapy Evidence Database up to August 2021. Randomised controlled trials investigating the effect of physiotherapy on tension-type headache were included. Risk of bias assessment was performed using the Risk of bias tool 2.0. Results were presented according to the Cochrane handbook and the PRISMA statement.
Results
Twenty reports were eligible and 15 were included in network meta-analysis for pain intensity and frequency. Transcutaneous electrical stimulation combined with physiotherapy was the most effective approach to reduce pain intensity compared to control (mean difference (MD): −4.18, moderate confidence) and usual care (MD: −3.8, moderate confidence) Manual therapy (joint mobilisation) plus exercise was the most effective intervention to reduce headache frequency compared to control (MD: −13.03, low confidence) and usual care (MD: −13.95, moderate confidence).
Conclusion
Results suggest a combination of passive physiotherapy techniques with exercise and/or transcutaneous electrical stimulation as the most effective physiotherapy intervention to reduce pain intensity and frequency in the short term. More research is needed to investigate mid-term and long-term effects.
Background
The prevalence of tension-type headache (TTH) ranges from 2.2% to 38.3% (1). For the treatment of acute phases and the reduction of headache frequency, pharmacological and non-pharmacological approaches can be used. A commonly used non-pharmacological treatment for TTH is physiotherapy (2), involving various modalities such as exercises, electrical stimulation, massage, joint mobilisation, trigger-point therapy and many more. But despite the abundance of physiotherapy interventions available, the majority of these have not been thoroughly evaluated for effectiveness. Hence, only a weak recommendation for their use is given by clinical guidelines (2). Several reviews and meta-analyses have confirmed a general effectiveness of physical therapy modalities on patients with TTH in the past (3–5). However, an evaluation of the most effective physiotherapy intervention using network meta-analysis (NMA) has never been attempted. The advantages of NMA, such as improvement in precision, the ability to compare treatments that have not been directly compared as well as the quantitative comparison of more than two treatments, suggest that this quantitative method could serve decision-making better than conventional pairwise meta-analysis (6). The purpose of this review was to assess the effectiveness of physiotherapy interventions on the intensity, frequency, and duration of headaches, as well as on the quality of life of patients with TTH using NMA.
Methods
The present systematic review was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses Statement for network meta-analysis (PRISMA-NMA) (7), as well as the Cochrane Handbook for Systematic Reviews of Interventions (8). The review protocol was prospectively registered on 12 August 2020 in www.aspredicted.org under the registration number #46098 and an updated protocol was registered on 23 February 2021 in the Open Science Framework (OSF) with the registration DOI: https://doi.org/10.17605/OSF.IO/RVUEY.
Information sources
A systematic literature search was carried out on 5 October 2020 in the following databases: Physiotherapy Evidence Database (PEDro), Web of Science, Medline via Pubmed and Cochrane Library. This search was updated on 23 August 2021. In addition, reference lists of included studies were reviewed to identify additional studies. The search strategy for each database is presented in Supplementary material A and the search was performed by two research clinicians independently.
Eligibility criteria
Records were screened using the following eligibility criteria (Table 1): Randomised controlled studies (RCTs) examining the effect of physiotherapy interventions on an adult TTH population were included. If TTH was not diagnosed according to the third edition of the International Classification of Headache Disorders (ICHD-3) (9) or previous editions (10,11), the study was excluded. Comparisons with control interventions including waiting list, sham therapy, placebo, standard care, or other active interventions were required for inclusion. In case of multi-arm trials, only data of eligible interventions (-arms) were extracted for quantitative synthesis. Data from outcome measurements assessing headache intensity, duration, frequency or quality of life were included.
Eligibility criteria.

ICHD-3: International Classification of Headache Disorders (3rd edition); IHS: International Headache Society.
Study selection
Titles and abstracts as well as full-texts were screened by two independent reviewers according to predefined eligibility criteria (Table 1). The inter-rater reliability of the reviewers’ agreement regarding study eligibility was expressed using Cohen’s kappa coefficient. In the event of a disagreement between the two investigators, a third reviewer was consulted to reach consensus.
Data collection process
Included data were manually extracted by one reviewer and controlled for accuracy by a second reviewer. The data items were extracted into a pre-specified extraction table: i) Author, date and country; ii) classification used for diagnosis; iii) participant numbers, age, sex (for each group); iv) type of the intervention including data on intervention and/or control intervention: Frequency, intensity, timing, length of treatment, staff qualification and setting; v) outcome measures (for each group): Measurement tools and timepoint of assessment. Where key data was missing, corresponding study authors were contacted.
Risk of bias assessment
Risk of bias (RoB) assessment was performed by two independent reviewers using the revised Cochrane Collaboration RoB 2.0 tool (12), which is a domain-based assessment tool addressing bias arising at different stages of the RCT. The RoB assessment was conducted according to the manual (https://www.riskofbias.info/welcome/rob-2-0-tool) and pilot tested prior to the data extraction. Since there is no explanation in the manual of how to rate the RoB in studies with retrospectively registered trial protocols, it was decided to treat them equally to non-existent protocols and the domain “bias in selection of the reported results” was rated as “some concerns”. Trial protocols that were retrospectively registered, but before unblinded data were available, were treated as prospective, since they do not raise concerns about bias according to the manual (13). RoB plots were created using the robvis tool (14).
Certainty of the evidence
The certainty of evidence of NMA was assessed using the Confidence in Network Meta-analysis (CINeMA) web application (https://cinema.ispm.unibe.ch), which is based on the framework described by Salanti et al. (15). This software allows to run a semi-automated assessment of the quality of evidence (16). Six different components are considered: Within study bias, reporting bias, indirectness, imprecision, heterogeneity, and incoherence. An examination of publication bias using a comparison-adjusted funnel plot (17) and linear regression test of funnel plot asymmetry (Egger test) were considered if there were more than 10 studies included in NMA for each outcome (18).
Analysis
Prior to statistical analyses, data was assessed for transitivity according to Salanti (6). Similarities of included reports were compared by age, sex, diagnostic/classification criteria, treatment parameters as well as study setting to evaluate if interventions included in the NMA were “jointly randomizable” (6). NMA was performed using a frequentist method with the statistical package “netmeta” (version 1.4-0) in R (https://www.r-project.org/). The “netgraph” function was used to present the network structure and to inspect the network geometry for each outcome of interest. Outcomes were pooled and analysed as mean difference (MD) for pain intensity and headache frequency using a random effects model and their 95% confidence interval (CI). Post-scores with its standard deviations (SD) were used to pool data in NMA. If no post-score of pain intensity or frequency was available in a trial, the reported change-score (from baseline) and its SD was considered, since it is legitimate to pool post- and change-scores together using the (unstandardised) MD according to the Cochrane Handbook (19). For headache frequency, the data of included trials was rescaled to a timeframe of 30 days. It was planned to pool data for short-term results (≤12 weeks), mid-term results (13 weeks to 6 months) and long-term results (>7 months) of each outcome individually. If two or more results were available for the same time-period described above, the last one was extracted for quantitative analysis. To assess for incoherence (inconsistency between direct and indirect evidence), two approaches, a local and a global approach, were used. For the local approach, the node-split function “netsplit” was used and differences between direct and indirect comparisons were tested statistically and reported using p-values. For the global approach, the design‐by‐treatment interaction test was performed by the CINeMA app (16). Statistical heterogeneity was assessed using I2 and Cochrane’s Q tests of heterogeneity within designs and between designs. The ranking of treatments was assessed using the P-score, which is a frequentist analogue to the SUCRA-value of the Bayesian approach (20). The P-score is a value between 0 and 1. The larger the P-score, the greater the likelihood of being the best treatment. Sensitivity analysis excluding studies with high RoB was considered.
There are no publications investigating clinically important changes of pain intensity, pain duration or pain frequency in patients with TTH. Therefore, clinically important changes were derived from other chronic pain populations (21) and recommendations in behavioural headache research (22). A reduction of 2.4 points on a 0–10 numerical scale was considered clinically important for pain intensity (21). For pain duration and pain frequency, a reduction of 50% was considered clinically important (22). For the latter two, a weighted mean of all included baseline data in NMA was derived based on sample size, to calculate the threshold for clinically important changes in NMA. Thus, the clinically important change for NMA of headache frequency and duration was a reduction of 7.5 headache days within a month and a reduction of 7.3 h respectively.
Results
A total of 378 records were identified through the electronic and hand search (Figure 1). After removing duplicates and title/abstract screening (Table 1), 40 reports were reviewed in full text. Twenty reports were included for qualitative synthesis, 20 were excluded due to reasons specified in Supplementary material B. The screening of reports reached a substantial inter-reviewer agreement (k = 0.78).

PRISMA flow-chart for study inclusion.
The characteristics of included studies are summarised in Table 2. The 20 studies included in this review evaluated numerous physiotherapy interventions such as cryotherapy, transcutaneous electrical nerve stimulation (TENS), trigger point therapy, soft tissue techniques, various mobilisation and manipulation techniques. Eight studies assessed a single modality (23–30), while the remaining studies evaluated multiple modalities. In all studies, participants were allowed to use abortive (acute) medication, regardless of the intervention allocation. The most common outcome measured was headache intensity via the visual analogue scale (VAS) (24,26,30–34), the numerical rating scale (NRS) (25,27,29,35–38), the verbal rating scale (28) or the 3-point severity index of the headache disability inventory (HDI) (39,40). Headache frequency was measured via a headache diary (1 week to 3 months) (23,25,26,28–32,35,36,38), the 3-point scale of the HDI (39,40), a 4-point scale (33) or a 5-point Likert scale (27). Quality of life was measured in three studies (24,38,41) (using SF-12 and SF-36) and headache duration was evaluated in five studies (25,28,30,31,38). With the exception of three studies (28,35,38), all included reports exclusively assessed the short-term effectiveness of physiotherapy interventions.
Characteristics of included studies.

CTM: connective tissue manipulation; CTP: craniocervical training program; CTTH: chronic tension-type headache; DT-MFR: direct technique myofascial release; E: experimental intervention; ETTH: episodic tension-type headache; IDT-MFR: indirect technique myofascial release; MT: manual therapy; MTrP: myofascial trigger point; NRS: numerical rating scale; NSAID: non-steroidal anti-inflammatory drug; QoL: quality of life; TCA: tricyclic antidepressants; TENS: transcutaneous electrical nerve stimulation; TPR: trigger point release; US: ultrasound; VAS: visual analogue scale; VAT: vertebral artery test; VRS: verbal rating scale.
*corrected data provided from corresponding author.
Narrative synthesis
Risk of bias within studies
In Figure 2 the results of the RoB assessment are presented. Most studies had “some concerns” as an overall rating, four had a “high risk of bias” (23,26,27,42) and one was rated as of “low risk of bias” (37). The lack of pre-registered protocols as well as the registration of retrospective protocols was the most critical factor, which highlighted “some concerns” in the domain “bias in selection of the reported result” (n = 15).

Risk of bias within studies.
Reports not included in NMA are being described in the following section. Demirturk et al. (42) investigated the effect of a combination of heat, massage and soft tissue techniques compared to heat, massage and manual therapy (MT). Both groups reported a statistically significant decrease of Headache Index values immediately after treatment and 1 month after treatment. However, there were no significant differences between groups.
One four-arm trial by Espi-Lopez et al. (39,41) compared spinal manipulative treatment versus suboccipital soft tissue inhibition (SI) versus a combination of both therapies versus no active treatment. Results showed that patients receiving the spinal manipulative treatment alone and a combination of both experimental treatments experienced significantly reduced HDI scores on headache frequency (39). The SI group experienced a significantly reduced headache intensity but no change in headache frequency (39). Only the SI group had significant improvements in the overall quality of life score at follow-up, while there were no significant improvements for any of the interventions post-treatment (41). Espi-Lopez et al. (40) evaluated the effectiveness of spinal manipulative treatment combined with gentle cervical massage versus gentle massage alone. Outcome measurements resulted in a significant reduction of headache frequency at follow-up for the manipulation group, while no significant changes were reported on all other timepoints as well as pain intensity in both groups.
Meng et al. (27) evaluated two cryotherapy treatment groups: A 10% weighted bamboo fibre pack group and a pure water ice pack group. Although both groups reported significant improvements regarding headache intensity and frequency after treatment, there was no difference between intervention groups.
Quantitative synthesis
After evaluation of transitivity, collation of treatments into treatment nodes and examination of the network geometry, a total of 15 reports (23–26,28–38) were included in NMA (14 reports for pain intensity and 10 reports for pain frequency). The remaining reports (n = 5) (27,39–42) could not be included in NMA because of a lack of transitivity, the outcome measurement method reported was not adequate to (statistically) pool, or because they had no connection to the network. No comprehensive networks could be built for headache duration and quality of life. Furthermore, mid-term or long-term results were reported by only three reports (28,35,38). Thus, NMA was only possible for the outcomes “headache intensity and frequency” in the short term (≤12 weeks). For all other outcomes, and for mid-term as well as long-term results, NMA was not possible. An overview of the treatment nodes and their description can be seen in Table 3.
Presentation and definition of treatment nodes.

In the present review, a total of 136 comparisons in headache intensity and 66 comparisons in headache frequency were analysed. Only statistically significant results of experimental interventions compared to control intervention or usual care are presented in the following sections. All results (forest plots) of NMA of headache intensity and frequency can be viewed in Supplementary material C and the certainty of the evidence of all comparisons in NMA can be viewed in Supplementary material D.
NMA of pain intensity for TTH
Summary of network structure and geometry
Fourteen reports (24–26,28–38) comprising a total of 820 patients with TTH were included in NMA of pain intensity. The network structure for pain intensity can be seen in Figure 3. Seventeen interventions were investigated in this network. Studies with multiple treatment arms are highlighted in Figure 3 as blue-coloured areas between treatment nodes. Most direct comparisons were evaluated by single studies. Only one direct treatment comparison was investigated by more than one study: Trigger-point therapy versus usual medical care (four studies).
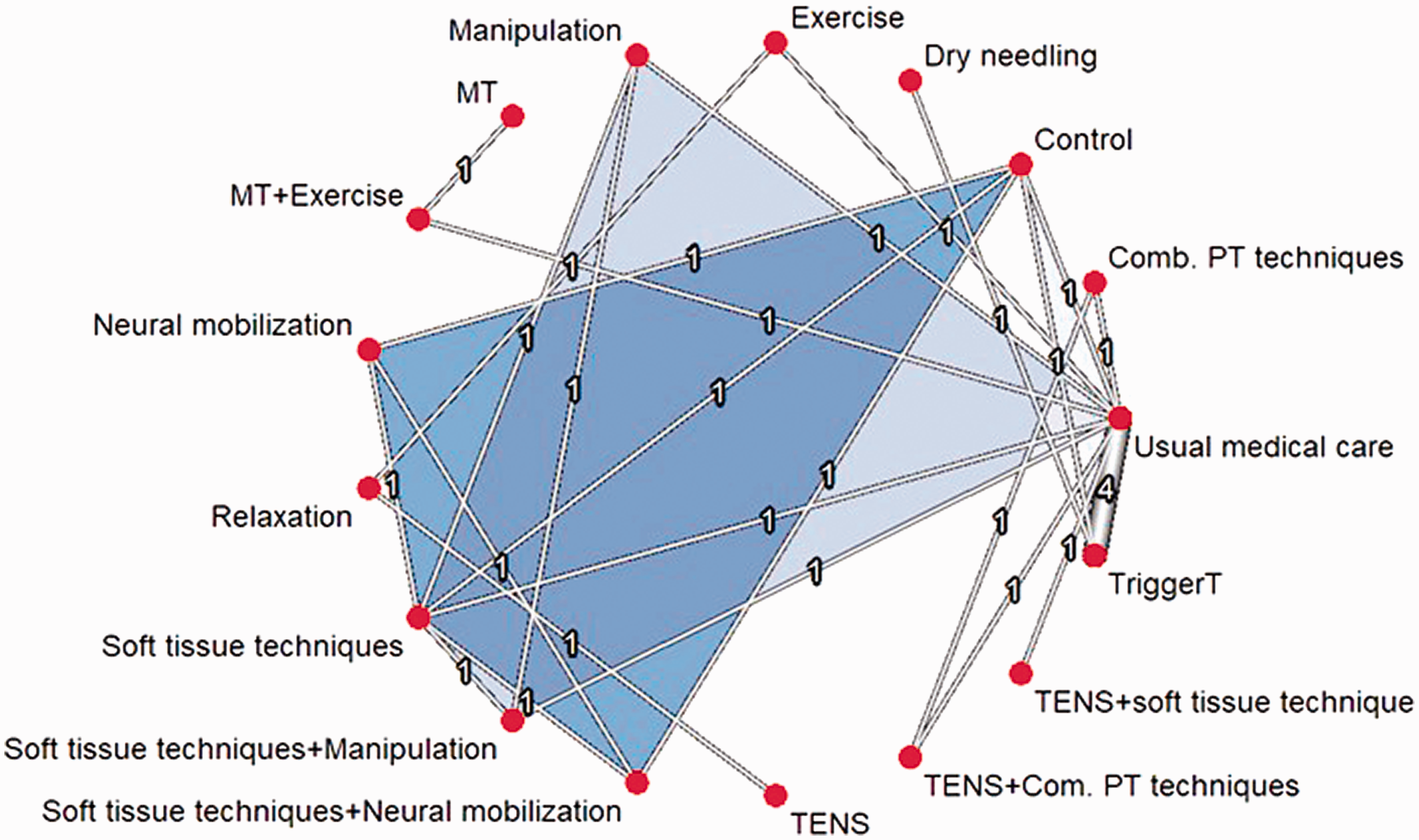
Network for headache intensity.
Exploration of inconsistency
There was evidence of statistical heterogeneity (p = 0.0161) according to the Cochrane’s Q test (Table 4). This was also confirmed by the I2 test (I2 = 67.1%, CI: 14.7% to 87.3%), representing substantial heterogeneity. According to the global test (p = 0.476) and the node split function (local test), there was no evidence of incoherence (Supplementary material E). Based on the funnel plot symmetry and the Egger test (p = 0.9778) (Supplementary material C) there was no sufficient evidence for publication bias.
Tests of heterogeneity (within designs) and inconsistency (between designs) for headache intensity.

Synthesis of results
TENS with various passive physiotherapy modalities was the most effective intervention according to the ranking of treatments (Table 5). Six interventions were significantly better when compared to control (placebo) intervention: TENS plus a combination of various passive physiotherapy techniques (MD: −4.18, CI: −6.16 to −2.19; moderate confidence), dry needling (MD: −2.76, CI: −5.49 to −0.03; low confidence), soft tissue techniques (MD: −2.13, CI: −3.46 to −0.79; low confidence), soft tissue techniques plus neural mobilisation (MD: −2.16, CI: −3.69 to −0.63; low confidence), MT (joint mobilisation) plus exercise (MD: −2.18, CI: −4.29 to −0.06; low confidence) and trigger point therapy (MD: −1.54, CI: −2.91 to −0.16; low confidence). Only four interventions were significantly better than usual medical care: TENS plus a combination of various passive physiotherapy techniques (MD: −3.8, CI: −5.3 to −2.3; moderate confidence), soft tissue techniques (MD: −1.75, CI: −3.21 to −0.3; low confidence), MT (joint mobilisation) plus exercise (MD: −1.8, CI: −3.47 to −0.13; low confidence) and trigger point therapy (MD: −1.16, CI: −2.07 to −0.26; low confidence). These results are presented in the two forest plots for headache intensity ranked by treatment effectiveness (Figure 4).
Treatment ranking (headache intensity): 17 treatments.

PT: physiotherapeutic; TENS: transcutaneous electrical nerve stimulation; MT: manual therapy.
*A larger P-score indicates a better treatment or “the probability of being superior to a competing treatment” (20).

Forest plots for headache intensity, other interventions vs. control (top) and other interventions vs. usual medical care (bottom), ranked by P-score.
NMA of headache frequency for TTH
Ten studies (23,25,26,28–32,35,36) assessing a total of 659 patients with TTH were included in NMA of headache frequency. The network structure for headache frequency can be seen in Figure 5. Twelve interventions were investigated in this network. Three studies had multiple treatment arms, which are indicated by the blue coloured areas between treatment nodes (Figure 5). Similar to the network on headache intensity, most direct comparisons were evaluated by single studies. Only two direct treatment comparisons were investigated by more than one study: Soft tissue techniques versus control (two studies) and trigger-point therapy versus usual medical care (three studies).

Network for headache frequency.
Exploration of inconsistency
There was evidence of statistical heterogeneity (p = 0.0076) according to Cochrane’s Q test (Table 6). and the I2 test (I2 = 71.2%, CI: 27.1% to 88.6%) also suggested substantial statistical heterogeneity. Based on the global test (p = 0.455) and the local test (Supplementary material E) there was no evidence of incoherence between indirect and direct comparisons. No funnel plot was created for headache frequency, given that there were not more than 10 studies included in the NMA.
Tests of heterogeneity (within designs) and inconsistency (between designs) for headache frequency.

Synthesis of results
Headache frequency is presented as the average of headache days per month (30 days). MT (joint mobilisation) combined with exercise was the most effective intervention according to the ranking of treatments (Table 7). Only three interventions were superior to a control intervention (placebo, sham): MT (joint mobilisation) plus exercise (MD: −13.03, CI: −20.90 to −5.16; low confidence), soft tissue techniques plus neural mobilisation (MD: −6.74; CI: −11.78 to −1.69; low confidence) and soft tissue techniques (MD: −3.88, CI: −7.39 to −0.37; low confidence). Five interventions were significantly superior to usual medical care: MT (joint mobilisation) plus exercise (MD: −13.95, CI: −20.24 to −7.66; moderate confidence), dry needling (MD: −9.95, CI: −18.76 to −1.13; low confidence), soft tissue techniques plus neural mobilisation (MD: −7.66, CI: −14.19 to −1.12; low confidence), soft tissue techniques plus manipulation (MD: −6.55, CI: −12.88 to −0.22; low confidence) and trigger point therapy (MD: −6.1, CI: −9.89 to −2.3; very low confidence). These results are presented in the two forest plots for headache frequency ranked by treatment effectiveness (Figure 6).
Treatment ranking (headache frequency): 12 treatments.

PT: physiotherapeutic; TENS: transcutaneous electrical nerve stimulation; MT; manual therapy.
*A larger P-score indicates a better treatment or “the probability of being superior to a competing treatment” (20).

Forest plots for headache frequency, other interventions vs. control (top) and other interventions vs. usual medical care (bottom), ranked by P-score.
Discussion
This is the first systematic review providing an NMA to evaluate the effectiveness of physiotherapy interventions on treatment outcomes of patients with TTH. A total of 20 reports of 19 studies were included for qualitative synthesis. Of these, 15 reports were included in the NMA.
The results of the quantitative analysis through NMA indicated that a combination of various passive physiotherapy techniques (including massage, traction, stretching and advice on postural correction) plus TENS as well as the combination of MT (joint mobilisation) with exercise and postural correction are likely to be the most effective physiotherapy approaches to reduce headache intensity or frequency in patients with TTH. Dry needling was also one of the most effective treatments to reduce pain intensity or frequency. Nevertheless, the effectiveness of dry needling should be interpreted with caution, since the results of this intervention are based on one report with a high RoB (26).
Interestingly, individual physiotherapy techniques were not as effective as combinations of approaches. For example, TENS or a combination of various passive physiotherapy techniques (individually) did not differ significantly from control or usual care, but they were superior to control or usual care and ranked as the most effective intervention to reduce pain intensity when combined. Likewise, MT or exercise (individually) were not as effective as the combination of both to reduce pain intensity or frequency compared to control or usual care. One possible explanation might be that each intervention adds a treatment and placebo response effect, and that the more interventions used, the greater the effect of placebo response could be expected to be (43). However, there are several factors (44) to consider and not enough information (from included studies) in order to confirm this hypothesis. Another interesting observation is that the combination of TENS and SI had no significant results when used simultaneously. The results for both outcomes are based on moderate to very low confidence in the NMA. The evidence regarding the most effective interventions to improve headache intensity or frequency compared to control or usual care is based on a moderate quality of evidence. Clinically relevant effect sizes for pain intensity (≥2.4) were reached by two interventions: TENS plus a combination of various physiotherapy techniques and dry needling. For headache frequency, clinically relevant effect sizes (≥7.5 days) were reached by three interventions: MT plus exercise, dry needling and soft tissue techniques plus neural mobilisation. Nonetheless, more research on minimal important change for the outcomes of headache intensity, frequency and duration of headache disorders is required.
Unfortunately, headache duration and quality of life could not be pooled in NMA. Additionally, no mid-term or long-term results could be assessed quantitatively, since all but three articles reported only on short-term results.
Although there are no other NMAs evaluating the effectiveness of physiotherapy on TTH, there are some reviews with a similar scope with and without meta-analyses. Kamonseki et al. (4) concluded after quantitative analysis that spinal manipulative treatment was not superior to “no therapy” (usual care), whereas soft tissue techniques and dry needling were superior to “no therapy” (usual care) for the reduction of pain intensity and frequency, thereby confirming the results of the current NMA. In the reviews by Fernández-de-Las-Peñas and Cuadrado (45) as well as Cumplido-Transmonte et al. (46), it was also affirmed that individual physiotherapy techniques seem not to be as effective as the combination of various physiotherapy techniques.
Overall, results of this current systematic review and previous reviews indicate that a combination of various physiotherapy interventions, including hands-on techniques (such as MT and soft tissue techniques), advice on postural correction, exercises, and/or TENS, are more effective than usual medical care alone. Whether physiotherapy can reduce or even replace medication intake cannot be assessed with the current data, since patients in the majority of studies were allowed to continue their medication regimen for ethical reasons.
Implications for future research
Most direct comparisons in the networks were based on single studies with “some concerns” regarding their RoB. More RCTs with “low” RoB are needed to confirm the results of the present review. Trial authors should be encouraged to pre-register their trials prospectively before unblinded data is available, since the lack of pre-registered protocols as well as the registration of retrospective protocols was the most critical factor which highlighted “some concerns” while evaluating the RoB of included studies. The use of a combination of various physiotherapy techniques should also be encouraged in future research, since there is evidence for their superiority regarding their effectiveness compared to individual physiotherapy intervention techniques. The assessment of mid-term and long-term results should be pursued in future trials.
Limitations
A limitation is that most studies included both episodic and chronic TTH patients and no subgroup analysis was provided by the authors. Therefore, baseline data for headache frequency was heterogenous between studies (between 11.6 and 23.7 headache days in a month). We were unable to separate both types for analysis. It is very likely that this affected the results for the outcome of headache frequency in the NMA, which could explain the presence of statistical heterogeneity. Nevertheless, it is unlikely that the inclusion of both classifications of TTH could have affected the outcome headache intensity since this is not dependent on the classification of TTH. A factor that could have led to the substantial statistical heterogeneity might be the heterogeneous intervention parameters (frequency, duration and length of interventions) in all included studies. However, sensitivity analysis to evaluate this potential limitation was not possible. Furthermore, presence of or controlling for other headache disorders (e.g. migraine) was not reported in five studies (25,26,29,32,36), which could limit the applicability of results. Lastly, no grey literature was searched and only reports in German or English language were included.
Conclusions
The results of the present review suggest that a combination of various passive physiotherapy techniques (including MT (joint mobilisation) and soft tissue techniques) with exercise, postural correction and/or TENS are the most effective physiotherapy interventions to reduce headache intensity and frequency of patients with TTH in the short term. Hence, these interventions can be considered in addition to usual care. Individual physiotherapy techniques seem not to be as effective as the combination of various physiotherapy techniques. This is supported by moderate to very low quality of evidence. More research is needed to confirm the results and especially to investigate mid-term to long term effects.
Clinical implications
Combined physiotherapy interventions are effective to reduce headache intensity and frequency and can be used as adjunct therapy to pharmacological interventions. Individual physiotherapy techniques seem not to be as effective as the combination of various physiotherapy techniques. More research on mid-term to long-term effects is needed. More studies with low risk of bias are needed.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024221082073 - Supplemental material for Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache. A systematic review and network meta-analysis
Supplemental material, sj-pdf-1-cep-10.1177_03331024221082073 for Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache. A systematic review and network meta-analysis by Andres Jung, Robert-Christopher Eschke, Julia Struss, Wiebke Taucher and Kerstin Luedtke in Cephalalgia
Supplemental Material
sj-pdf-2-cep-10.1177_03331024221082073 - Supplemental material for Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache. A systematic review and network meta-analysis
Supplemental material, sj-pdf-2-cep-10.1177_03331024221082073 for Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache. A systematic review and network meta-analysis by Andres Jung, Robert-Christopher Eschke, Julia Struss, Wiebke Taucher and Kerstin Luedtke in Cephalalgia
Supplemental Material
sj-pdf-3-cep-10.1177_03331024221082073 - Supplemental material for Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache. A systematic review and network meta-analysis
Supplemental material, sj-pdf-3-cep-10.1177_03331024221082073 for Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache. A systematic review and network meta-analysis by Andres Jung, Robert-Christopher Eschke, Julia Struss, Wiebke Taucher and Kerstin Luedtke in Cephalalgia
Supplemental Material
sj-pdf-4-cep-10.1177_03331024221082073 - Supplemental material for Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache. A systematic review and network meta-analysis
Supplemental material, sj-pdf-4-cep-10.1177_03331024221082073 for Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache. A systematic review and network meta-analysis by Andres Jung, Robert-Christopher Eschke, Julia Struss, Wiebke Taucher and Kerstin Luedtke in Cephalalgia
Supplemental Material
sj-pdf-5-cep-10.1177_03331024221082073 - Supplemental material for Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache. A systematic review and network meta-analysis
Supplemental material, sj-pdf-5-cep-10.1177_03331024221082073 for Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache. A systematic review and network meta-analysis by Andres Jung, Robert-Christopher Eschke, Julia Struss, Wiebke Taucher and Kerstin Luedtke in Cephalalgia
Footnotes
Original publication
The authors declare that this manuscript contains original unpublished work and is not being submitted for publication elsewhere at the same time. There were no previous submissions.
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Availability of data and materials
All data generated or analysed during this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Authors' contributions
All authors contributed to the design of the study. JS and WT designed the search strategy and conducted the systematic search. JS, WT, AJ and KL screened titles and abstracts as well as full-text reports. Data extraction was performed by JS and checked by WT. Quality appraisal and data analysis was performed by AJ, R-CE and KL. Statistical analysis was conducted by AJ and checked by KL. JS and AJ drafted the manuscript. R-CE and KL critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.