
Abstract
We conducted a multicentre, randomized controlled trial with blinded outcome assessment. The treatment period was 6 weeks with follow-up assessment immediately thereafter and after 6 months. The objective was to determine the effectiveness of a craniocervical training programme combined with physiotherapy for tension-type headache. Eighty-one participants meeting the diagnostic criteria for tension-type headache were randomly assigned to an exercise group (physiotherapy and an additional craniocervical training programme) and a control group (physiotherapy alone). The primary outcome measure was headache frequency. Secondary outcomes included headache intensity and duration, Quality of Life (SF-36) and the Multidimensional Headache Locus of Control scale (MHLC). At 6 months' follow-up, the craniocervical training group showed significantly reduced headache frequency, intensity and duration (P < 0.001 for all). Effect sizes were large and clinically relevant. Loss to follow-up amounted to 3.7±. Physiotherapy including craniocervical training reduces symptoms of tension-type headache significantly over a prolonged time frame.
Introduction
Tension-type headache is the most prevalent headache type. Almost 80% of the total population will experience a tension-type headache at some time. Headache is one of the 10 major complaints of patients seen in primary care practices and 47% of all headaches are tension-type headaches (1). ‘Tension-type’ labels a headache classification developed in 1988 by the International Headache Society (IHS). It can be divided into an episodic and a chronic version (2) and is commonly more experienced by women (female:male ratio 5 : 4) (3).
Because of its high prevalence—1-year prevalence in women 86% and in men 63% (4)—and its wide spectrum of disability, tension-type headache has a greater socioeconomic impact than any other headache type (5). In spite of this, only 15% of people with tension-type headache seek medical attention (2) and 60% of those reporting severe headaches use only ‘over-the-counter medication’, standing a chance of analgesic rebound (6). Instead of self-management, a therapeutic approach, incorporating both non-pharmacological and pharmacological intervention, shows a success rate of >90% in patients with tension-type headache (7–9).
The specific cause of tension-type headache is unknown, but is most likely multifactorial (10–19), as adequately described by Olesen's vascular-myogenic-supraspinal model (20).
Until now, no previous trial has investigated the effect of craniocervical training in tension-type headache, dealing with specific deficits in muscle control of the cervicospinal part of the neck (21, 22). This randomized, controlled trial assessed the short- and long-term effects of two approaches to tension-type headache: standard physiotherapy including a craniocervical training programme (CTP) in order to re-educate muscle control of the cervicospinal region (CTP group) and standard physiotherapy alone (control group) (23–25).
Methods
Design
The study was a prospective, multicentre, randomized controlled trial with blinded outcome assessment. Allocation was by means of a computerized randomized block design with stratification for version of tension-type headache (episodic vs. chronic), sex and treatment centre (one of the seven participating trial centres).
Based on sample size calculation with a two-sided α of 0.05 and a power of 0.80, 80 patients had to be included to detect a 60% reduction of headache frequency in the intervention group, such a treatment effect being considered clinically relevant (26). Informed consent was obtained before randomization. The procedures followed were in accordance with the ethical standards of the responsible committees on human experimentation and with the Helsinki Declaration.
Participants
Eligible patients were referred by general practitioners, after which they were screened on inclusion and exclusion criteria in one of the seven participating primary healthcare centres in the area of Amsterdam, the Netherlands. Those who fulfilled the symptomatic criteria underwent physical examination of the cervical spine including three function tests with relevance to the prescribed exercises of the intervention group.
The inclusion criteria followed the IHS classification for tension-type headache. The episodic version is defined as recurrent episodes of headache lasting minutes to days and <15 days per month. Pain quality is typically ‘pressing’ or ‘tightening’, of mild to moderate intensity, bilateral in location and not worsening during routine physical activity. Nausea and vomiting are absent, but photophobia or phonophobia may occur (2). The chronic version differs from the episodic since headache is present for at least 15 days per month, while in addition to photophobia or phonophobia, nausea may occur (2). During the trial period, the IHS classification was revised (ICHD-II). However, the diagnostic criteria for tension-type headache were unchanged and therefore the revised classification did not interfere with the inclusion criteria of this study. Exclusion criteria specified the other headache types as described in the ICHD-II classification. Moreover, the presence of more than one type of headache in addition to tension-type headache, cervical function problems and previous physiotherapy treatment for tension-type headache during the last 6 months were excluded.
Interventions
Physiotherapy consisted of a threefold approach: conventional Western massage techniques, oscillation techniques and instruction on postural correction. Conventional massage techniques included the following modes: ‘effleurage’ (stroking), ‘petrissage’ (kneading) and ‘friction’ (deep pressure). Mode and intensity were determined by the physiotherapist in accordance with the diagnosis and the patient's condition as a clinical routine. Oscillation techniques included the use of low-velocity, passive cervical joint mobilization, in which the cervical segments are rhythmically moved following a regimen described by Maitland (27). The two approaches described above are intended to reduce pain and musculotendinous tension.
Instruction on postural correction originates with the worst postural position of craniocervical extension (anteversion) of the head, cervicothoracic flexion, protraction of the shoulders and increased thoracic kyphosis and flattened lumbar lordosis while sitting. The physiotherapist instructs patients to correct these postural abnormalities through craniocervical flexion (retroversion) and cervicothoracic extension, retraction of the shoulders, extension of the thoracic spine and normalization of lumbar lordosis.
The craniocervical training programme was a new developed programme using low-load endurance exercises in order to train and/or to regain muscle control of the cervicoscapular and craniocervical regions (28). To address the impairment in neck flexor synergy found in cervicogenic headache and other neck pain disorders (29, 30), craniocervical flexion exercises were performed, using a latex band (Thera-Band®, Resistive Exercise Systems; Hygenic Corporation, Akron, OH, USA blue colour-coded level of progressive resistance). The 150-cm latex band was used as a circular band, with one side positioned at the craniocervical region of the patient's neck and the other side fixed somewhat above the horizontal. The resistance of the band was used in such a way that it facilitated the longus colli muscles (31). Exercises were performed in a sitting position with a natural lumbar lordosis, under slight scapular retraction and adduction and slightly elongating the cervical spine. Participants were instructed to perform a slow and controlled craniocervical flexion over various ranges of motion, resulting in various resistances, with various speeds using isometric contractions in various positions (Fig. 1a,b).

(a) Starting position in craniocervical extension (anteversion). (b) Final position with craniocervical flexion (retroversion).
This craniocervical low-load training regimen was also incorporated in postural correction exercises. The duration of the CTP part of the treatment session did not exceed 15 min. During the intervention period, the participants were instructed to practice this CTP at home twice a day for 10 min per session. Using a daily diary, changes in headache frequency, intensity, duration and medication intake were monitored and compliance was controlled. After the treatment period the participants were instructed to continue the craniocervical training at home with a frequency according to their complaints, but at least twice a week. Preceding the start of the trial, 20 experienced senior physiotherapists in the seven participating treatment centres were explicitly trained to execute the protocolled treatments.
Measurement instruments
Pain was assessed using a Numerical Rating Scale (NRS), an 11-item scale, with 0 representing no pain and 10 representing pain as bad as it could be, depicted on a horizontal line. Subjects were asked to mark the number that best represented the current level of pain they were experiencing. Various formats of the NRS (11-point levels of measure, 21-point levels of measure and 101-point numerical rating scale) have provided reliable data with coefficients >0.99 (32). The validity and reliability of the NRS to measure pain in patients experiencing pain of acute and chronic origin have been demonstrated (33–36).
The Short-Form General Health Survey (SF-36) was used to asses health-related quality of life. The SF-36 is a generic 36-item self-administered survey that measures eight health domains: physical functioning (PF), social functioning (SF), role limitations due to physical health (RP), role limitations due to mental health (MH), general health (GH), emotional well-being (RE), vitality (VT) and bodily pain (BP) and two summary scores, physical component summary (PCS) and mental component summary (MCS). Three scales (PF, RP, BP) correlate most highly with the physical component and contribute most to the scoring of the PCS measure. The mental component correlates most highly with the MH, RE, and SF scales, which also contribute most to the scoring of the MCS measure. Three of the scales (VT, GH, SF) have noteworthy correlations with both components. The health domains described in the SF-36 range in score from 0 to 100, with higher scores indicating higher levels of functioning or better health. The reliability of the SF-36 has been estimated using both internal consistency and test–retest methods. With rare exceptions, published reliability statistics have exceeded the minimum required level of 0.70 recommended for measures used in group comparisons and most have exceeded 0.80. Validity studies generally support the intended objective of high and low SF-36 scores as documented in the original user's manuals (37–41).
The Multidimensional Health Locus of Control (MHLC) scales have been developed as specific instruments for measuring locus of control in the healthcare field. The MHLC scales used are moderately reliable; Cronbach alphas range from 0.60 to 0.75 and test–retest reliability coefficients from 0.60 to 0.70. Convergent validity has been calculated at r = 0.62–0.73 (42, 43).
The MHLC used in this trial was specified for headache (Multidimensional Headache Locus of Control) and was examined to determine whether the patient's health beliefs, specifically about the control over one's headache, were influenced by the interventions.
Statistical analysis
Baseline characteristics were summarized with descriptive statistics (Table 1). Furthermore, between-group analyses were performed using Mann–Whitney U-tests at end-point and at 6-month follow-up. Within-group analyses were performed using the Wilcoxon signed ranks test at end-point and at the 6-month follow-up. Spearman's rank correlation coefficients were calculated to examine the correlation between the Headache Locus of Control and the primary and secondary outcome measures.
Comparability of intervention groups at baseline in headache characteristics, prognostic variables and outcome measures

Data are expressed in frequencies or means (±SD).
CTP, Craniocervical training group; ETTH, episodic tension-type headache; CTTH, chronic tension-type headache; NRS, numeric rating score; WDD, weekly dose expressed in days; SF-36, Short-Form 36; PCS, physical component summary; MCS, mental component summary; MHLC, Multidimensional Headache Locus of Control.
For all outcome measures effect sizes of mean differences (ES) were calculated by dividing the difference between the mean changes in the outcomes of the control group and the CTP group by the within-group standard deviation of the total group.

Effect sizes were considered small (0.2), medium (0.5) or large (0.8) (44). All analyses were done with SPSS 12.0 (SPSS Inc., Chicago, IL, USA) according to the intention-to-treat principle.
Results
Of the 81 participants who entered the trial group, 38 in the CTP group and 42 in the control group received treatment and 3.7% were lost to follow-up. Participant flow and retention are summarized in Fig. 2. Randomization started in December 2003, recruitment was completed in April 2005 with follow-up scheduled to continue through October 2005. Baseline characteristics between the two groups were analogous (Table 1). No adverse events were reported in any group.
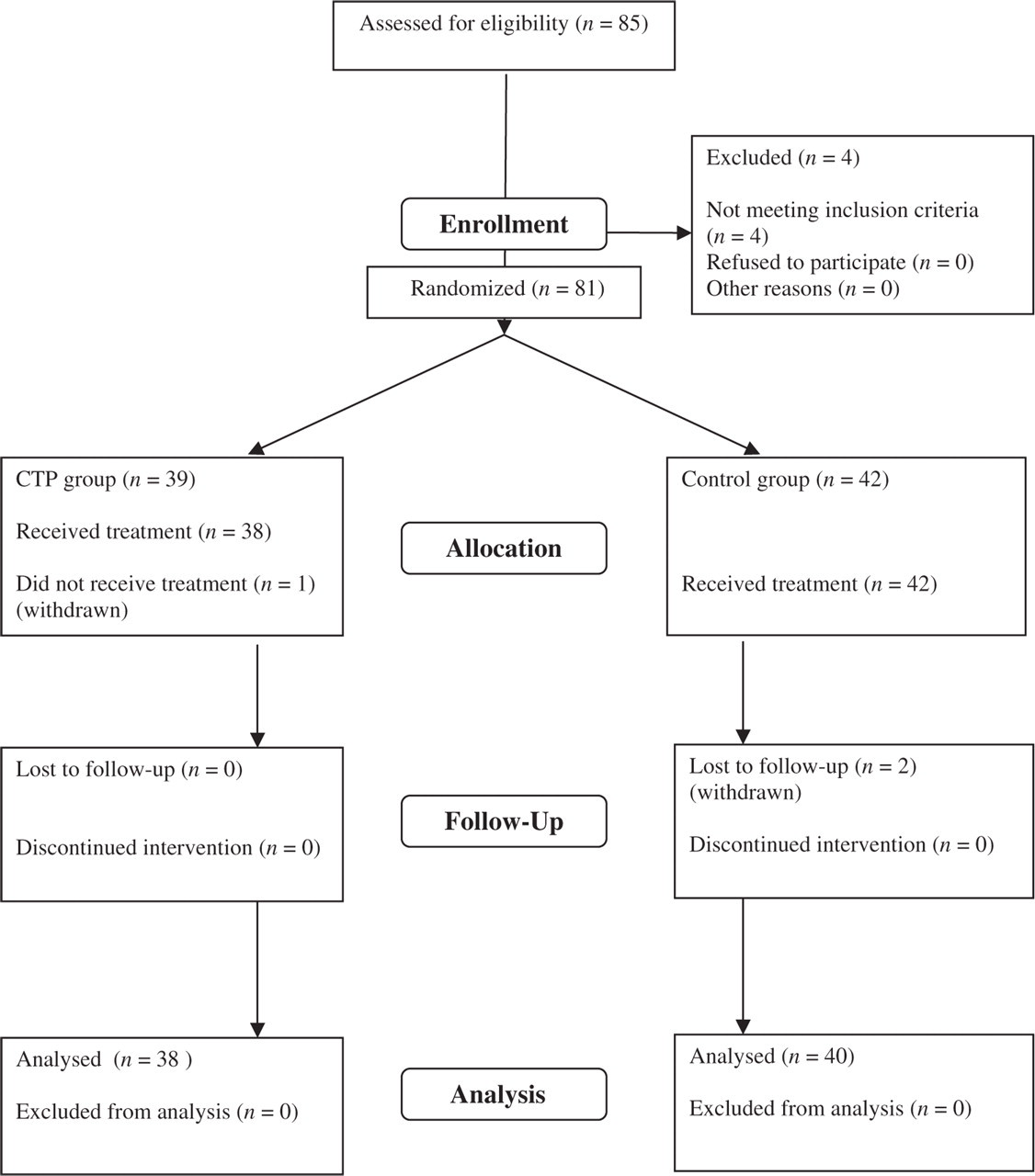
Flow diagram of progression of participants through the trial.
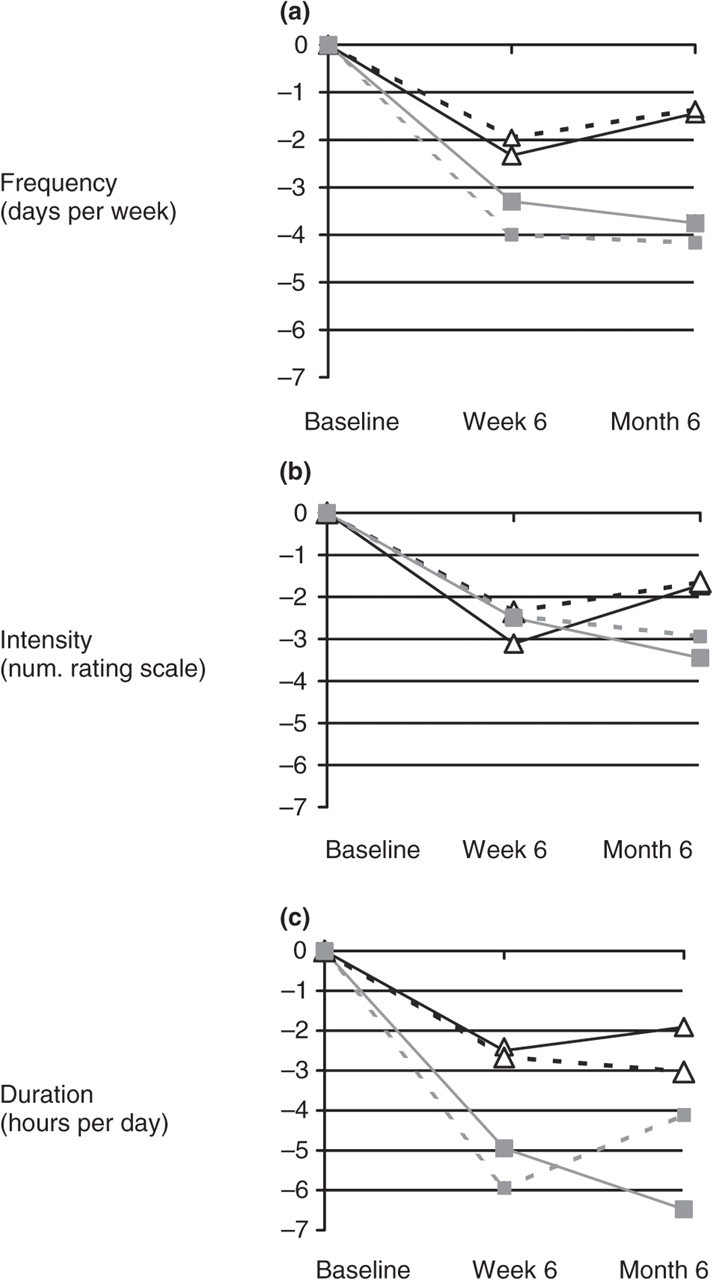
Mean changes in headache frequency, intensity and duration from baseline to end-point and follow-up are plotted in Fig. 3a–c. Wilcoxon signed ranks analyses showed that treatment within both the control group and the CTP group significantly reduced headache frequency, intensity and duration immediately after treatment. At this point, however, Mann–Whitney U analyses showed no significant difference between the control and CTP groups.

Mean changes in headache frequency (a), intensity (b) and duration (c) from baseline to end-point (week 6) and follow-up (month 6) per treatment group. ▵, Control; ▪, craniocervical training programme.
In the control group, however, from end-point to follow-up a significant increase in frequency, intensity and duration in headache occurred (P = 0.007, P = 0.001, P = 0.022, respectively). In contrast, the CTP group showed further reduction of headache frequency (P = 0.039), intensity (P = 0.007) and duration (NS).
At follow-up, the CTP group differed significantly from the control group in terms of headache frequency, intensity and duration (P = 0.0001, P = 0.001, P = 0.011, respectively) (Table 2).
Mean changes (95% CI) in primary and secondary outcome measures at end-point (week 6) and follow-up (month 6)

PCS, Physical component summary; MCS, mental component summary.
Significant difference (P = 0.05).
Quality of life assessment in terms of mean changes in PCS and MCS showed significant improvement in PCS (P < 0.001 for all) within groups and significant improvement between groups at follow-up in RE (P = 0.014), MH (P = 0.05), VT (P = 0.039) and BP (P = 0.017).
Calculation of treatment effect showed at a large effect size in both groups in terms of reduction of frequency, intensity and duration of the headache. The mental component summary showed a medium effect. Overall, at end-point, the CTP group showed the largest effect sizes.
The effectiveness of the two approaches was also investigated by examining the number of subjects who met the bench-mark cut-off point of a ≥50% reduction in headache frequency. In the control group 52% and 35% of the participants (at end-point and follow-up, respectively) met this criterion, in the CTP group the percentage amounted to 82% and 85% (at end-point and follow-up, respectively).
At end-point, the Wilcoxon signed ranks test showed up to 40% reduced medication intake within both treatment groups (control group P = 0.001; CTP group P = 0.0001). At follow-up, however, no significant reduction in the control group (P = 0.081) was found; in contrast, the CTP group showed a 65% reduction (P = 0.0001).
Within the CTP group, the Mann–Whitney U-test showed a significant difference between the two groups (P = 0.003). Subgroup analysis showed a significant reduction in favour of the chronic tension-type headache group (P < 0.0001). Subgroup analysis for chronic tension-type headache (CTTH) and episodic tension-type headache (ETTH) by the Wilcoxon signed ranks test and the Mann–Whitney U-test showed that the within- and between-group headache frequency was in accordance with the unstratified analysis. Mean changes in headache frequency, intensity and duration for these subgroups are plotted in Fig. 4a–c.
Mean changes in headache frequency (a), intensity (b) and duration (c) from baseline to end-point (week 6) and follow-up (month 6) per treatment group after stratification for type of headache. ▵, Control episodic tension-type headache (ETTH); - - ▵ - -, control chronic tension-type headache (CTTH); - - ▪- -, craniocervical training programme (CTP) CTTH; ▪, CTP ETTH.
Analysis of mean changes of the headache locus of control revealed no significant differences, either within or between the treatment groups. Spearman's rank correlation analysis showed no significant correlation between the headache locus of control and any outcome measures.
Discussion
This trial supported evidence that physiotherapy combined with a specific therapeutic exercise regimen was effective for tension-type headache. Although there was no significant difference between the two treatment groups immediately after treatment (end-point), at follow-up a significant and clinically relevant effect was shown in the CTP group.
As various research suggests (11, 13, 20, 22, 23, 45), afferent input produced by joint mobilization stimulates inhibitory systems at various levels in the spinal cord and modulates pain perception. It is most likely that the mechanisms of the treatment effect in this trial are to be found in the afferent input attributed to the mobilization and oscillation techniques of physiotherapy and to treatment by craniocervical exercises. This specific craniocervical training programme emphasized motor control rather than muscle strength and was carried out daily to twice a week in the post-treatment period. In this way, afferent input was continued in the craniocervical training group after end-point measurement. Possibly, this post-treatment period had a consolidating effect.
The CTP group showed a decrease in medication intake of 60%, which is more than 50% compared with the control group. The ETTH assessed in this study is synonymous with the frequent ETTH according to the ICHD-II classification. Participants suffering from infrequent ETTH were not included. Within the CTP group, a higher reduction of medication intake was shown in the CTTH group compared with the ETTH group.
The calculated effect size showed a large effect for all headache symptoms. A 50% reduction in headache frequency is regarded as clinically relevant by the IHS (26). In this study 85% of the participants in the CTP group showed a ≥50% reduction in headache frequency at follow-up, with 48% reporting 80–100% reduction at that time, indicating substantial clinical relevance. In contrast to what might be expected, the Headache Locus of Control was not influenced by the treatment effect and consequently could not be regarded as a predictive factor for any outcome measure.
Since patients with tension-type headache very often use self-administered
pain-relieving manoeuvres with only scant efficacy (46), the craniocervical training in
this trial caters for this target group since the exercises are easy to perform,
take little time and are effective. Considering the fact that reduction of headache
frequency, intensity and duration continues after 6 months, a follow-up study
including a longer time frame should be conducted to determine the efficacy of
craniocervical exercises as a potential stand-alone treatment over a longer period
of time. A substantially longer follow-up will also emphasize the aspect of
self-management of craniocervical training and might eventually detect a change in
the Headache Locus of Control. The question arises whether the underlying mechanisms
of craniocervical training reflect modulation of pain perception through increased
afferent input, or the effect on craniocervical posture resulting in reduction of
cervicoscapular muscle tone. In other words: is it the action, or is it the posture?
No answer can be provided from this trial, but the results underline the necessity
for researching multimechanisms to explain pain reduction by this physiotherapeutic
treatment. Trials of non-invasive physical therapies for tension-type headache have
been criticized for poor methodological quality (47–49). Reviewers’
recommendations suggest the necessity of further research, using rigorous scientific
methods. We tried to fulfil this condition by following the
In conclusion, this trial has shown that physiotherapy including a craniocervical training programme is effective in the management of chronic and episodic tension-type headache over a prolonged time frame.