
Abstract
Background
Argentina has one of the largest territories in the world, which spreads over a lengthy latitudinal span. Its population is mainly composed of a mixture of South American natives and the descendants of numerous waves of European immigrants. Results from a previous study suggested that the prevalence of migraine in Argentina is the lowest in the region. Here we aimed to reassess the prevalence of migraine in Argentina applying a more sensitive and specific screening tool.
Methods
We conducted a random computer assisted telephonic interview (n= 2500) using the Migraine Screen Questionnaire to evaluate the prevalence of migraine and some of its features among Argentinian adults.
Results
The overall prevalence of migraine was 9.5% (14% in females and 5% in males). Estimated migraine prevalence rates ranged between 6.3% and 12% across different regions. The approximated prevalence of high frequency and chronic migraine were 1.9% and 1.5% of the total population respectively. Consumption of analgesics on 10 or more days per month was reported by 18% of migraine sufferers (≈1.7% of the population).
Conclusions
The prevalence of migraine in Argentina is higher than previously reported. Prevalence rates vary extensively across the territory. Specifically evaluating the determinants of these variations might be a promising avenue of research.
Introduction
Migraine is a multifactorial neurological disorder that results from the interaction between a genetically predisposed individual and an enabling environment (1,2). Therefore, although no region is spared from the burden of this disease, its prevalence rates vary across populations with diverse genetic and cultural backgrounds, living in areas with distinct climates, or facing different socioeconomic contexts (3).
Argentina has one of the largest territories in the world (2,780,400 km2) (4), which spreads over a lengthy latitudinal span and comprises multiple different ecosystems. Not only is its climate varied, but also its ethnicity is diverse. Argentina’s population (approximately 44.5 million in 2018) (4) is mainly composed of a mixture of South American natives and the descendants of numerous waves of European immigrants, but also includes several other ethnic groups in lesser proportions (5). From an economic viewpoint, Argentina (together with Georgia, Kosovo, and Sri Lanka) has recently been categorized into the upper-middle income level of the World Bank classification (6), which reflects the struggling nature of the economy of this nation. Geographically, Argentina can be divided into five main regions (i.e. Cuyo, North-western, North-eastern, Pampean, and Patagonian), with different sociocultural and climate conditions.
Headache medicine in Argentina is a developing field. Despite some major recent advances in the study of medication overuse headache features in this country (7,8), to date, little is known about the epidemiology of migraine and other primary headache disorders. Currently available data come from a study conducted 15 years ago, which evaluated the prevalence of migraine in six different Latin American countries including Argentina (9). In that publication, the authors reported a 1-year prevalence of migraine of 5.6% in females and 3.5% in males of the Argentinian population, the lowest in the region according to their findings. This study was relevant because it was the first of its kind to evaluate the problem of migraine in Latin America, but participation rates in Argentina were fairly low and agreement between the 49-item questionnaire that the investigators employed and expert neurologists’ diagnoses showed only a moderate (kappa coefficient 0.58) degree of concordance during the validation (9). Thus, results from that study might not accurately reflect the real–life scenario in this country, warranting the need for a reappraisal where more sensitive and specific diagnostic tools are applied (10).
The Migraine Screen Questionnaire (MS-Q) is a screening instrument originally developed in Spanish (Argentina’s official language) by a group of headache experts (11). It is based on the International Headache Society (IHS) criteria (12,13), and consists of five yes-no questions addressing headache frequency, intensity, duration, disability, and accompanying symptoms. A cut-off value of four positive responses has a sensitivity of 0.93 and a specificity of 0.81 for the diagnosis of migraine (11). Of note, although a new edition of the ICHD came out after the MS-Q was originally developed, diagnostic criteria for migraine without aura (1.1), upon which the MS-Q mostly relies, remained unchanged (12,13). Therefore, despite the Classification update, the MS-Q remains current in the present.
The purpose of this study was to reassess and describe the prevalence of migraine in Argentina using the MS-Q.
Materials and methods
This study was an initiative of the Headache group of the Argentinian Neurological Society. All Argentinian residents above 18 years of age were considered eligible. There was not an a priori defined upper age limit; all subjects deemed capable of comprehending and answering questions made by the interviewer were included. The target/intended population consisted of individuals who had suffered from headache during the last year. Taking into account across-country variations in telephone line-per-household density (mean 38.19%, range 75.1–23.09%), in order to obtain a sufficient number of cases per stratum, a probabilistic selection of residences with telephone lines (not regionally proportional) was performed. The sample was subsequently weighted by census parameters. From 8 March to 11 April 2019, 18,000 residences were screened via a computer assisted telephone interview (CATI). Computer-assisted telephone interviewing is a telephone surveying method in which a trained interviewer interrogates participants following instructions provided by specifically designed software and registers data in structured digital forms. In case of a busy line, up to three dialing attempts were performed. The initial screening question, intended to ensure the inclusion of all forms of migraine, was: “Have you had a headache during the last 12 months?” (14). The Migraine Screen Questionnaire (MS-Q) was then applied to participants responding positively to this question. In addition, positive cases were interrogated about other characteristics of their headache, such as analgesic consumption, and about their headache-related behaviours and beliefs. Some of these data are beyond the scope of this study and will be presented separately.
This study was approved by the FLENI ethics committee (Reg. 38-20). All data were fully anonymized. Due to the survey nature of this research, written informed consent was not required.
Statistical analyses and graphs were performed using Prism version 6.00 for Windows (GraphPad Software, La Jolla, California, USA) and Microsoft Excel (Microsoft Corporation, 2018).
Results
Out of the 18,000 total outgoing calls, 2500 led to valid contacts. This resulted in a calculated margin of error of ± 2.06% with a CI of 95%. Fifty-three percent of respondents reported having suffered from headache during the last 12 months and thus continued with the rest of the interview. On the basis of the MS-Q results, the overall prevalence of migraine was 9.5% (14% in females and 5% in males). In other words, 74% of positive migraine cases were female and 26% were male. Estimated migraine prevalence rates ranged between 6.3% and 12% across different regions. Response rates for each of the five items in the MS-Q are shown in Figure 1. Light/noise discomfort had the highest number of positive answers whereas nausea had the least. As far as they could recall, for the vast majority of patients headache developed between 12 and 49 years of age (Figure 2). On average, patients reported reduced performance due to migraine on 6 days per month (median = 3) (Figure 3). Regarding high frequency and chronic migraine, one third (≈34%) of migraine patients referred to having headache on 8 or more days per month, including 16% who referred to having headache on more than 15 monthly days. Consequently, the approximated prevalence of high frequency and chronic migraine were estimated at around 1.89% and 1.5% of the total population, respectively. In line with that, consumption of analgesics and/or anti-migraine drugs (i.e. the available triptans, sumatriptan, naratriptan, and eletriptan, or ergotamine-containing compounds) on 10 or more days per month was reported by 18% of migraine sufferers (≈1.7% of the population).
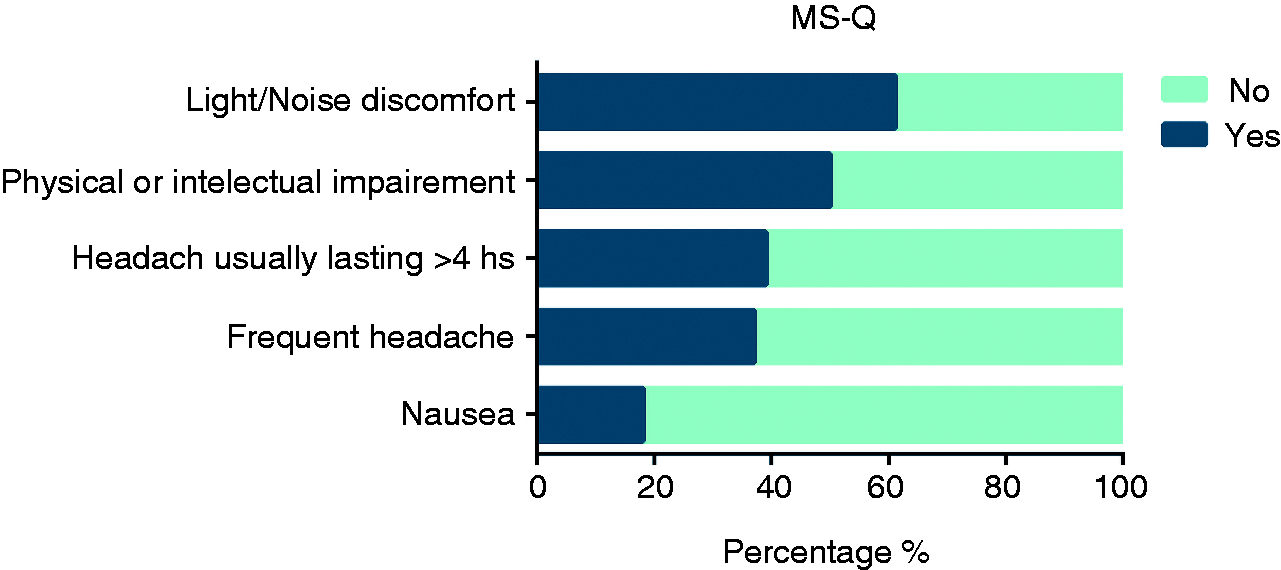
Migraine patients’ response rates to each of the five items in the MS-Q.

Age of disease development.

Monthly days of reduced performance due to headache.
Discussion
In this study, we evaluated the prevalence of migraine in Argentina using a validated questionnaire developed in Spanish and, in addition, we assessed some characteristics of the disease in the population. Our results markedly contrast with those previously reported (9) in the sense that the prevalence rates of migraine that our study found are significantly higher than the ones formerly described (14% vs. 5.6% for women and 5% vs. 3.5% for men) (9). We consider this to be the result of applying a more efficient screening instrument rather than what would represent a truly rapid augmentation of migraine’s prevalence in this country. Indeed, our results are more in line with global and regional migraine prevalence estimates (15), and therefore it is possible that they more accurately reflect the actual prevalence rates of the disease in Argentina compared with prior data.
Interestingly, we observed marked variations of prevalence rates across different regions in this country, which ranged between 12% in the southernmost (Patagonian) region, and 6.3% in the north-western region, next to the border with Bolivia and Chile (Figure 4). It is probable that a combination of different factors accounts for these variations, yet some particularities about these regions seem to provide valuable clues. For instance, people living in the region with the lowest migraine prevalence, the north-western region, have the lowest percentage of European ancestry in the country (33%) according to genetic studies (5). In contrast, the region with the highest migraine prevalence, the Patagonian region, has a high percentage of European inheritance (54%), but perhaps most notably, this region expands over the more extreme latitudes and therefore has the coldest weather (16,17). Remarkably, the economically less privileged region of the country (Nord-Eastern) (18) showed near-average prevalence rates (i.e. 9.9%). Similarly, illiteracy, taken as an indicator of the education level, did not contribute substantially to explain migraine prevalence in each region. The genetic nature of this condition (19) and its close relation with the environment (20,21) are well-established features of the disease, but based on previous research, a stronger pressure of the socioeconomic context might have also been expected (22). Further studies particularly evaluating this issue might help clarify and expand our findings.
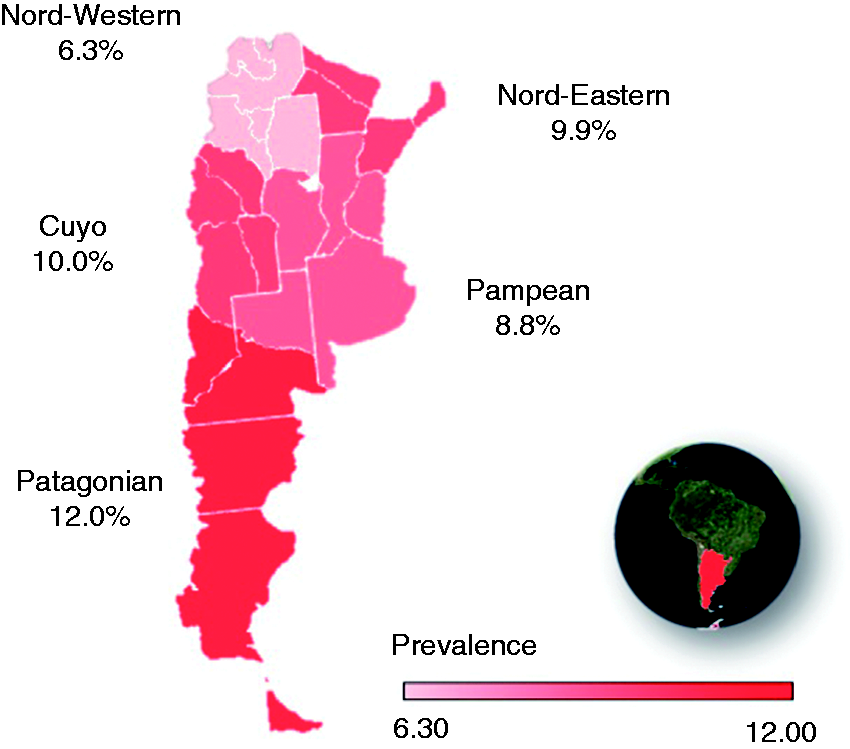
Migraine prevalence in the five main regions of Argentina (colour-coded).
Considering chronic migraine, the most burdensome facet of migraine, our prevalence estimates and the calculated proportion of patients overusing acute treatment were similar to the ones observed in other countries (23). Based on previous data (8), it is likely that most of these patients are overconsuming ergotamine-containing anti-migraine preparations, which could result in a more difficult withdrawal treatment. Updated region-specific treatment guidelines that address this particularity might thus be necessary (24).
Our study has some limitations worth mentioning. Most of the questions relied on patients’ memories and are thus subject to recall bias. Furthermore, because of the limited genetic data, a proper regression analysis of the differing prevalence rates could not be performed and thus, the reasons behind the differences herein discussed remain purely speculative. Further studies addressing these issues are warranted. In addition, telephone line availability and household income might be related, and this could be considered as a source of bias. Indeed, it is possible that the indices of poverty and illiteracy that are presented in Table 1 are not adequate measures of regional income and/or education levels in countries with marked economic inequality, as is the case in Latin America. Therefore, no firm conclusions about how socioeconomic pressure impacts migraine prevalence rates can be drawn from our data. Finally, the criterion we used to define chronic migraine was the presence of headache on ≥ 15 days per month in a migraine patient. Although this criterion has been used in several studies in the past (25), it is not strictly adherent to the ICHD criteria and therefore the actual prevalence of chronic migraine in this region could differ if stricter criteria were used. Nonetheless, because of the overall improved methodology employed in our analysis, we are confident that the main findings of this study constitute an important advance in the study of migraine’s epidemiology in Argentina and in the region, particularly with respect to previous data.
Migraine prevalence and associated demographic features. Data taken from Avena et al.,(1)* temperature registries,(2)** and The Argentinian National Statistics and Census Institute.(3)‡

Headache Group of the Argentinian Neurological Society
Fiorella Martin Bertuzzi, Laura Davidow, Andrea Marengo, Beatriz Kinjo, Bibiana Saravia, Carla Buonanotte, Daniel Doctorovich, Daniel Gestro, Fabiana Rodríguez, Federico Buonanotte, Federico Pelli Noble, Fernanda Páez, Fernanda Soria, Gustavo Fishbein, Héctor Zavala, Helga Maria, Ingrid García Gómez, Isabel Rua, Jorge Alberto Giglio, Jorge Taconi, José Jesús de Paz, Juan Carlos Roma, Laura Aragó, Leonardo Ayala, Lourdes Molina, Lucas Bonamico, Lucía Zavala, María de Lourdes Figuerola, Maria Teresa Goicochea, Marina Olivier, Noemi Tinetti, Osvaldo Bruera, Pablo Schubaroff, Rosana Guerreros, Silvina Miranda, Soledad Oviedo, Soledad Smechow and Viviana Rocchi.
Public health relevance
The prevalence of migraine in Argentina is 9.5%. Approximated prevalence rates of high frequency and chronic migraine were estimated at around 1.89% and 1.5% respectively, with 1.7% of the adult population consuming analgesics or antimigraine drugs on 10 or more days per month. The burden of migraine in Argentina may have been previously underestimated.
Footnotes
Acknowledgements
The authors of this study wholeheartedly acknowledge the collaboration of Professor Miguel Láinez.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Novartis.