
Abstract
The classification subcommittee of the International Headache Society (IHS) has recently suggested revised criteria for medication overuse headache (MOH) and chronic migraine (CM). We field tested these revised criteria by applying them to the headache population at the Danish Headache Centre and compared the results with those using the current criteria. For CM we also tested two alternative criteria, one requiring ≥ 4 migraine days/month and ≥ 15 headache days/month, the second requiring ≥ 15 headache days/month and ≥ 50% migraine days. We included 969 patients with migraine or tension-type headache (TTH) among 1326 patients treated and dismissed in a 2-year period. Two hundred and eighty-five patients (30%) had TTH, 265 (27%) had migraine and 419 (43%) had mixed migraine and TTH. The current criteria for MOH classified 86 patients (9%) as MOH, 98 (10%) as probable MOH and 785 (81%) as not having MOH after a 2-month drug-free period. Using the appendix criteria, 284 patients (29%) were now classified as MOH, no patients as probable MOH and 685 (71%) as not having MOH. For CM only 16 patients (3%) fulfilled the current diagnostic criteria. This increased to 42 patients (7%) when we applied the appendix criteria. Using the less restrictive criteria of ≥ 4 migraine days and ≥ 15 headache days, 88 patients (14%) had CM, whereas the more restrictive criteria of ≥ 15 headache days and ≥ 50% migraine days resulted in 24 patients (4%) with CM. Our data suggest that the IHS has succeeded in choosing new criteria for CM which are neither too strict, nor too loose. For MOH, a shift to the appendix criteria will increase the number of MOH patients, but take into account the possibility of permanent changes in pain perception due to medication overuse and the possibility of a renewed effect of prophylactic drugs due to medication withdrawal. We therefore recommend the implementation of the appendix criteria for both MOH and CM into the main body of the International Classification of Headache Disorders.
Introduction
The International Classification of Headache Disorders, 2nd edn (ICHD-II) introduced a new diagnostic category: the probable headache diagnosis (1). For primary headaches the term ‘probable’ is used when headache characteristics fulfil all but one of the criteria for the primary headache in question and thus is just a new name for the term used in ICHD-I (2). For the secondary headaches there is often a criterion requesting improvement or resolution within a specified timeframe or following treatment of the presumed causative disorder. In this case the term probable is used if sufficient follow-up is not available or a diagnosis has to be made before the expected time needed for remission. In order to be classified as medication overuse headache (MOH), headache must resolve or revert to its previous pattern within 2 months after discontinuation of the overused drug. The diagnosis of probable MOH is therefore used only as a temporary diagnosis until medication withdrawal is completed and—based on the outcome—a final diagnosis of MOH can be applied or rejected. The criterion of resolution or reversion to previous pattern is very difficult to determine and thus leaves considerable room for interpretation. In consideration of these problems, the classification subcommittee of the International Headache Society (IHS) has recently presented revised research criteria for MOH in the appendix section, where the criterion regarding resolution or reversion has been removed (3). To be diagnosed as MOH according to the appendix criteria, it suffices to have a required minimum monthly frequency of drug intake and ≥ 15 days/month with headache. The required frequency of drug intake is identical to the current criteria.
Also introduced in ICHD-II was the concept of chronic migraine (CM). This diagnosis requests that patients fulfil criteria for migraine without aura on ≥15 days/month and do not fulfil the criteria for MOH. Since most attacks of migraine without aura start with a phase where they phenomenologically fulfil the criteria for tension-type headache (TTH), early treatment with a triptan may abort the attack before the typical migraine characteristics develop. Almost all patients with frequent migraine also suffer from TTH in addition, so misclassification may be very prevalent. As a consequence of the difficulty in distinguishing between which episodes are migraine and which are TTH, these patients have generally been excluded from drug trials, resulting in very little evidence-based medicine concerning this severely affected group of patients. In order to amend this situation, the classification subcommittee of the IHS has suggested less restrictive criteria for CM to be included in the appendix section. It still requires ≥ 15 days/month with headache and no medication overuse, but now it suffices to have 8 days/month fulfilling the criteria for migraine without aura or days where attacks are treated and relieved by triptans or ergots before the expected development of the typical migraine characteristics (3).
The purpose of the present study was to field test the suggested appendix criteria for MOH and CM by applying these new criteria to the headache population at the Danish Headache Centre (DHC) and compare the results with those using the current criteria. For CM we also describe the outcome using two alternative criteria. The first includes patients with ≥ 4 migraine days/month and ≥ 15 headache days/month, the second includes patients with ≥ 15 headache days/month and ≥ 50% of the headache days fulfilling criteria for migraine without aura.
Materials and methods
DHC is a tertiary out-patient referral Headache Centre. It functions as the only national referral centre for severely affected headache patients in Denmark (5.4 million inhabitants). At the time this study was done, only referrals made by neurologists were accepted. After a restricted period of time patients were discharged and treatment responsibility transferred to either the referring neurologist or their general practitioner.
All patients discharged from DHC in 2002 and 2003 had prospectively filled out a diagnostic headache diary on a daily basis. Diagnoses, headache frequency and medication use were determined from these prospective recordings. The patients were primarily diagnosed according to ICHD-I, but data allowed subsequent reclassification according to ICHD-II.
After establishment of a diagnosis of probable MOH (1), all acute headache medication was discontinued abruptly and patients were kept medication free for 2 months as part of the general treatment program in DHC (4). In case of severe opioid overuse, phenobarbital substitution was used for a short period to avoid abstinence syndromes. Overuse of barbiturates or benzodiazepines must be tapered slowly, but marked overuse of these substances was not documented among our patients. Levomepromazine or promethazin was allowed as the only rescue medication during withdrawal, primarily to be used for the first week. After withdrawal, headache frequency was reassessed and diagnoses were revised. All presented diagnoses for patients with medication overuse are thus based on headache characteristics after withdrawal. The arbitrarily selected cut-off for diagnosing MOH according to the current criteria was for migraine, mixed migraine and TTH a 50% reduction in headache frequency (days/month) after withdrawal, whereas for pure TTH a 50% reduction in either frequency or intensity sufficed (0–3 scale). The latter was based on the clinical experience that a modest reduction in headache intensity and duration, measured in hours per day, is usually considered highly relevant and a major improvement for patients with chronic TTH. Consequently, most clinical trials involving TTH make use of a headache index as efficacy measure, where intensity and duration are also taken into account. We have discussed this issue in a previous study (5). A final diagnosis of probable MOH was given if the patients did not complete withdrawal from overused medication or if the necessary information about frequency/intensity was incomplete.
All patients with a diagnosis of migraine, TTH or the combination of migraine and TTH were included in the study, regardless of headache frequency and medication use.
Statistics
Data were summarized using frequency tables and descriptive statistics in SAS version 8.2 (SAS Institute Inc., Cary, NC, USA).
Results
Among 1326 patients treated and dismissed from DHC in 2002 and 2003, we identified 969 (73%) with a diagnosis of TTH, migraine or the combination of migraine and TTH. There were 222 men (23%) and 747 women (77%). Mean age was 43 years (range 13–92 years) and mean headache frequency at first visit was 18 days/month (range 0–30 days/month). Among the 969 patients, 285 (30%) had TTH, 265 (27%) had migraine and 419 (43%) had a combination of migraine and TTH. Their demographics are presented in Table 1.
Demographics of all patients
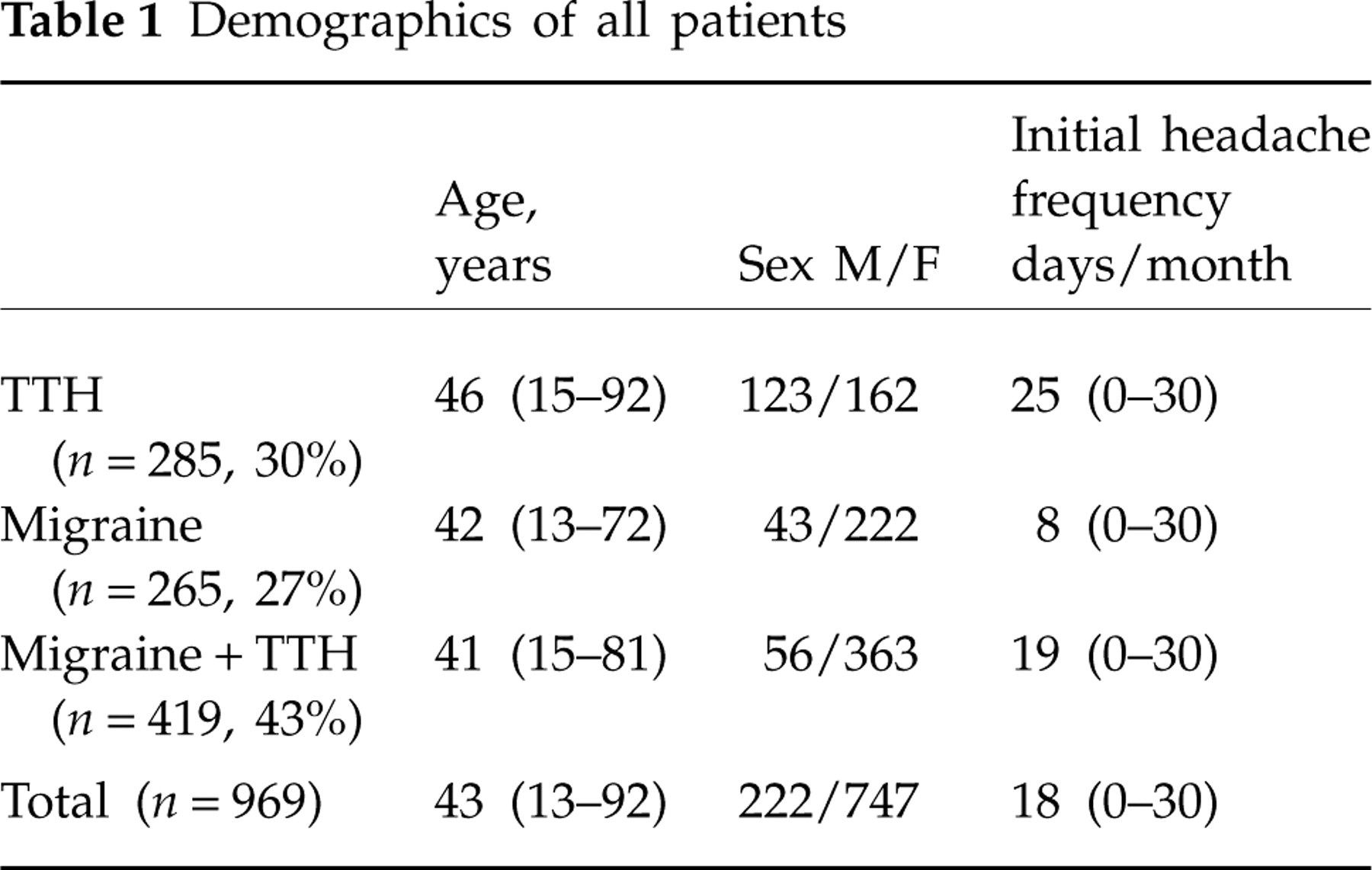
Mean values with range in parentheses.
TTH, tension-type headache.
According to the current ICHD-II criteria for MOH, 86 patients (9%) were classified as MOH, 98 (10%) as probable MOH and 785 (81%) as not having MOH after a 2-month drug-free period. Applying the appendix criteria for MOH changed this distribution to 284 patients (29%) classified as MOH, no patient as probable MOH and 685 (71%) as not having MOH (Table 2). The reason for there being more MOH patients according to the appendix criteria than to the ICHD-II criteria is that all patients with an overuse fulfil the appendix criteria for MOH. In contrast, the ICHD-II MOH diagnosis was given after a 2-month drug-free period, where those who did not improve received no MOH diagnosis and those who did not discontinue the overuse received the probable MOH diagnosis. The inclusion of patients who did not improve following withdrawal accounted for 51% of the increased number of MOH patients, and the inclusion of those classified as probable MOH accounted for 49% of the increase.
Number of patients classified according to the current criteria for MOH and according to the appendix criteria
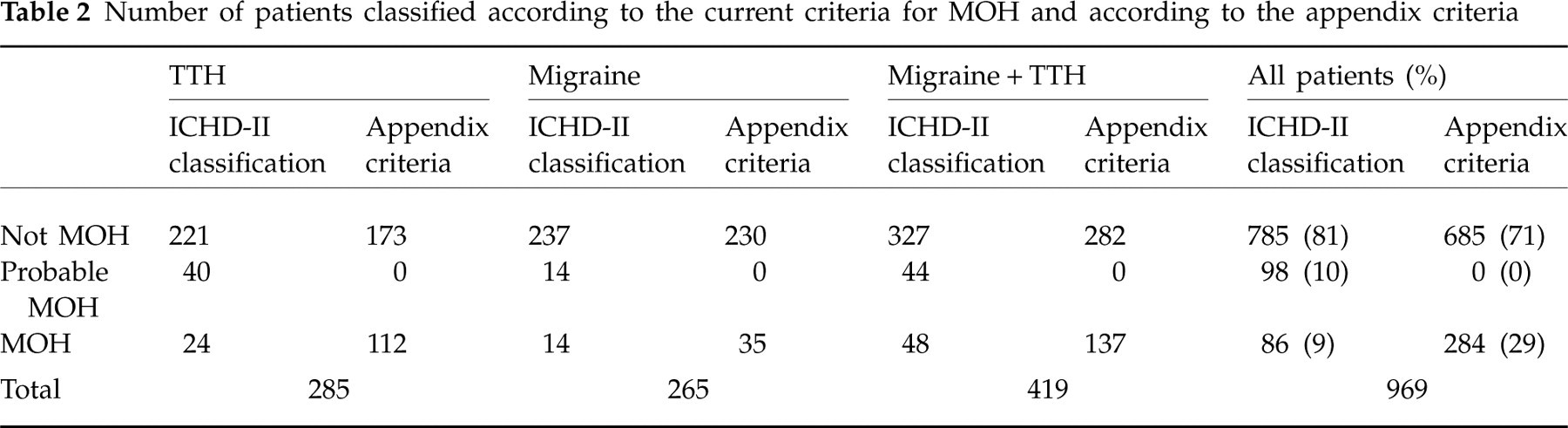
MOH, medication overuse headache; ICHD-II, International Classification of Headache Disorders, 2nd edn.
Looking at the primary headache diagnoses, TTH accounted for 44% of the increased number of MOH patients when we applied the appendix criteria, migraine accounted for 11% and the combination of migraine and TTH for the remaining 45%.
In order to compare the current and the appendix criteria for CM, we divided all patients with a diagnosis of migraine or the combination of migraine and TTH into two groups based on whether or not they had medication overuse at first visit. Of the 684 eligible patients, 512 (75%) had no medication overuse and 172 (25%) overused drugs at first visit. Among the 172 patients with medication overuse, 58 (34%) did not complete withdrawal. Because the CM diagnosis requires no medication overuse, these 58 patients were excluded, leaving 626 patients eligible for analysis. Overall, 16 patients (3%) fulfilled the current ICHD-II diagnostic criteria for CM. This increased to 42 patients (7%) when the appendix criteria were applied. Of patients without medication overuse, 1% fulfilled the current CM criteria and 4% the appendix criteria (Table 3). Of patients with medication overuse, 10% had CM after withdrawal according to the current criteria, whereas 18% had CM after withdrawal according to the appendix criteria (Table 4).
Number of patients with chronic migraine and no medication overuse at initial visit

TTH, tension-type headache; ICHD-II, International Classification of Headache Disorders, 2nd edn.
Number of patients with chronic migraine after withdrawal from a medication overuse at initial visit

TTH, tension-type headache.
We also tested two alternative criteria for CM. Using the less restrictive criteria of ≥ 4 migraine days and ≥ 15 headache days, 56 patients (11%) had CM in the group without medication overuse (Table 3) and 32 (28%) had CM following withdrawal in the group with medication overuse (Table 4). When we applied the more restrictive criteria of ≥ 15 headache days and ≥ 50% migraine days, nine patients (2%) had CM in the group without medication overuse (Table 3) and 15 (13%) had CM following withdrawal in the group with medication overuse (Table 4). The percentages of patients classified as CM according to the four different criteria are summarized in Fig. 1.
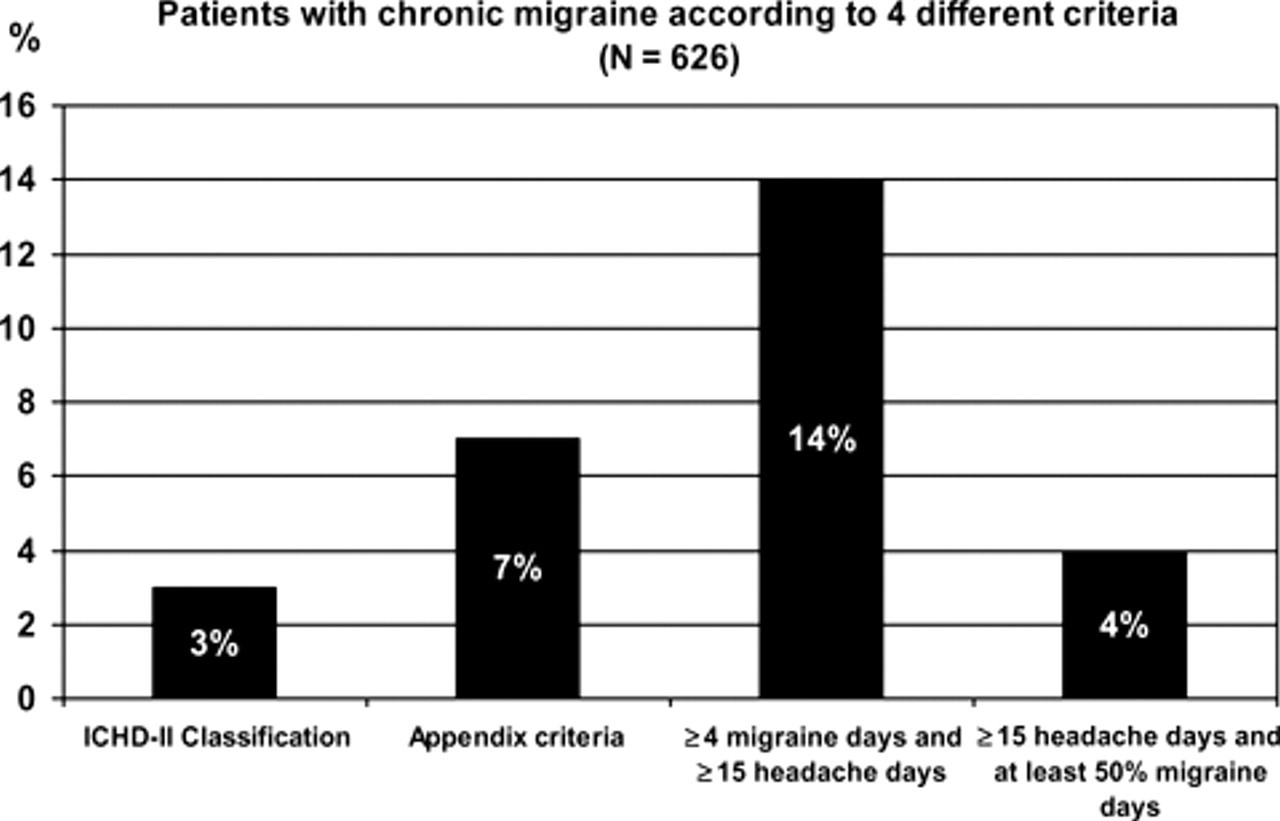
Patients with chronic migraine according to four different criteria (n = 626).
Discussion
The present study has shown that a change from the current criteria for MOH to the appendix criteria will increase the number of MOH diagnoses in specialized headache centres from 9 to 29% of the referred patients with a diagnosis of TTH, migraine or the combination of TTH and migraine. Half of this increase is because the appendix criteria include patients who do not improve following withdrawal and half is because the appendix criteria include patients who do not discontinue their overuse. According to the current criteria, these two groups are diagnosed as either no MOH or as probable MOH.
We have previously shown that the relative reduction in headache frequency by mere discontinuation of overused drugs differs between the primary headaches, with a 67% median reduction in migraine, 37% in the combination of migraine and TTH, and 0% in pure TTH (5). Because the appendix criteria include those patients who do not improve, TTH and the combination of TTH and migraine accounted for 89% of the increase in MOH diagnoses, whereas pure migraine accounted for only 11%. This is consistent with the expected reduction in headache frequency following withdrawal and our arbitrarily selected cut-off (50% reduction in headache frequency after withdrawal) for diagnosing MOH according to the current criteria.
Interpreting our data, one has to take into account that the study was conducted in a tertiary referral headache centre and is therefore not necessarily applicable to other populations. Furthermore, the diagnostic distribution differs from that usually seen in tertiary headache centres, with larger proportions of pure TTH and mixed migraine and TTH. These variations are probably due to our systematic prospective use of diagnostic diaries. Episodic TTH is usually underdiagnosed in a diagnostic interview compared with a diagnostic diary, and nausea, photophobia and phonophobia tend to be more pronounced at the clinical interview (6).
One of the major improvements in ICHD-II was the revised and more specific criteria for MOH. However, at the same time this part of ICHD-II has become more complicated, even for headache specialists. With an estimated prevalence of medication overuse in the general population of 1–2% (7, 8) and an occurrence of MOH in general practice as the third most common headache diagnosis next to TTH and migraine (9), this is a major problem. The main problem with the MOH diagnosis in ICHD-II is that the diagnosis can be made only after withdrawal. The first time a patient consults because of medication overuse, one has to give the diagnosis probable MOH. If there is improvement following withdrawal then the diagnosis of MOH can be applied, but at this time the patient no longer has MOH. Furthermore, even in the absence of improvement after withdrawal it is possible that previous medication overuse has caused enduring changes in pain perception that persist after discontinuation of medication overuse. Furthermore, successful withdrawal without improvement may change a previously refractory headache into a headache susceptible for prophylactic treatment (10). This previous study from our group showed that half the patients with medication overuse did not improve in headache frequency by mere discontinuation of the overused drug. However, the same patients subsequently became responsive to therapeutic intervention in the time period after drug withdrawal (10), and at least part of the improvement could be explained by a renewed effect of prophylactic drugs due to medication withdrawal.
We therefore believe that changing the current criteria for MOH to the appendix criteria is supported by data. In addition, the appendix criteria are easier to understand for both patients and doctors because they highlight what must be done in any overusing patient—withdrawal from overused drugs.
Few topics in ICHD-II have been subject to more debate than CM. Since Silberstein et al. in 1996 proposed new diagnostic criteria for chronic daily headache (CDH) including revised criteria for transformed migraine (TM) (11), it has been debated whether or not these diagnoses should be included in ICHD-II. This has not happened, but CDH is still widely used in the literature despite strong arguments against using it as a diagnosis (12). In ICHD-II it was intended that the CM diagnosis could cover a significant proportion of patients fulfilling criteria for CDH and TM. However, since CM requires migraine features for ≥ 15 days/month it is obviously a more restrictive diagnosis than TM, which only requires ≥ 15 days/month with headache and a link to migraine, i.e. an evolution from episodic migraine to daily or near-daily headache (11).
In the absence of a gold standard, one way to evaluate alternative criteria for CM is to calculate the proportion of TM patients who fulfil different CM criteria. In a recent article based on a CDH population, Bigal et al. (13) showed that only 5.6% of TM patients without medication overuse fulfilled the ICHD-II criteria for CM. Of TM patients with medication overuse, 10.2% could be classified as probable CM with probable MOH. In our study only 3% of the eligible patients fulfilled current criteria for CM. For patients without medication overuse the proportion was 1%, whereas 10% of the patients with medication overuse could be classified as CM after withdrawal. These numbers are not directly comparable, since we have included an entire headache population and not only CDH patients with TM. However, the 10.2% classified as probable CM with probable MOH are fairly close to the 10% CM patients we found after withdrawal from drug overuse. The same study also tested several proposals for alternative CM criteria (13). One of the proposals was very close to the suggested appendix criteria for CM (≥ 15 days/month with headache and ≥ 8 days/month with migraine), yet they allowed headache to fulfil either IHS criteria for migraine or probable migraine, whereas the appendix criteria only include IHS criteria for migraine without aura. Using their alternative criteria increased the number of CM patients, as 94.9% of TM patients without medication overuse were now classified as CM, whereas 91% of TM patients with medication overuse were classified as probable CM with probable MOH (13). This contrasts with our findings, since only 7% of our patients could be classified as CM according to the appendix criteria, 4% of the patients without medication overuse and—following withdrawal—18% of the patients with medication overuse. Again, caution is needed, since not all our patients had TM, but the 91% classified as probable CM with probable MOH are far from our proportion of 18% CM patients following withdrawal from overuse. The difference is probably due to the inclusion of patients with probable migraine in the American study. This inclusion is problematic, since the criterion of duration has already been removed in CM. It therefore becomes meaningless to delete one out of the remaining two criteria—pain characteristics and accompanying symptoms. Furthermore, probable migraine cannot be used if headache fulfils criteria for TTH. This aspect was not discussed in the paper by Bigal et al. (13). Thus, we maintain that our results reflect the true diagnostic distribution of CM using the appendix criteria.
We also tested two alternative criteria for CM. The criteria requiring ≥ 15 headache days and ≥ 50% migraine days was almost as restrictive as the current classification criteria for CM, as only 4% had CM compared with 3% using the current criteria. Applying the less restrictive criteria of ≥ 4 migraine days and ≥ 15 headache days, in contrast, increased the percentage of CM to 14%, almost a fivefold increase compared with ICHD-II criteria (3%) and twice as many compared with the suggested appendix criteria (7%).
According to the classification subcommittee of the IHS, one of the objectives for suggesting revised, less restrictive criteria for CM was to classify a severely affected subgroup of migraine patients in order to encourage research and allow these patients to participate in drug trials. Our data suggest that the subcommittee has succeeded in choosing CM criteria that are neither too strict, nor too loose. A shift to the appendix criteria will increase the number of CM patients seen in tertiary headache centres, but the diagnosis is still restricted to a severely affected subgroup of migraine patients. Whether or not the appendix criteria are suited to classify TM patients with a single ICHD-II diagnosis—i.e. CM—remains to be tested in future studies.
In conclusion, we therefore recommend the implementation of the appendix criteria for both MOH and CM into the main body of the International Classification of Headache Disorders.
Footnotes
Competing interests
None to declare.
Acknowledgements
The authors thank Mrs Hanne Andresen for technical assistance during data collection. The study was supported by grants from ‘IMK Almene Fond’. The funding source was not involved in any stage of the study.