
Abstract
Abstract
Introduction
Headaches associated with personal protective equipment were reported in health-care workers in previous epidemiological studies.
Methods
National web-based survey advertised by the Portuguese Headache Society and National Headache and Migraine patient´s organization between September-December 2020 screening for personal protective equipment usage pattern, pre-existing and de novo headaches after the onset of the COVID-19 pandemic, and its relation to personal protective equipment use.
Results
Of 5064 participants, 90.6% (4562/5034) were women, mean age was 37.2 ± 11 years. Most questions had a completion rate above 87% (non-completion rate ranging from 0–12.7%). Twenty percent were health-care professionals (993/5046). Surgical and cloth masks were the most common personal protective equipment type, whereas protective eyewear and FFP2/FFP3 masks were mostly used by health-care professionals. About 97% (1814/1870) of migraine and headache participants reported aggravation of pre-existing headaches with personal protective equipment use, and 56% (2476/4420) had de novo headaches. Participants with de novo headaches had a higher frequency of pre-existing migraine (1118/1226, 91.2% vs 1408/1600, 88%, P = .042), and wore personal protective equipment for longer periods of time (7 ± 2 h 42 vs 6 ± 2 h 54 min per day, P < .001). In multivariate analysis longer mean duration of personal protective equipment use (OR of 1.1, 95% CI 1–1.2) and previous migraine (OR of 1.2, 95% CI 1–1.4) were predictors of developing de novo headaches.
Conclusions
Almost all participants with pre-existing headache reported worsening of their headaches, and more than half of the study population developed de novo headaches following personal protective equipment use. Duration of personal protective equipment usage and pre-existing migraine were the strongest predictors of de novo headaches.
Introduction
Coronavirus disease 2019 (COVID-19) greatly impacted individual health, healthcare systems, politics, economics, and society on a global scale. Due to the escalation of the outbreak, not only frontline health care workers but also the population was recommended, and then required to wear personal protective equipment (PPE), which involve face masks and protective eyewear, amongst others (1). Healthcare and other workers (such as police officers and supermarket staff) are bound to use PPE for prolonged periods of the day, even in the absence of respiratory symptomatology. In the authors’ experience, many patients have spontaneously reported the occurrence of headaches in this setting, and headache patients reported worsening of their headaches, both in outpatient visits and patients’ forums.
Headaches related to wearing PPE at work have been described in certain populations (such as construction workers, military personnel, and swimmers) due to prolonged use of headwear or helmets, which may relate to compression headaches (2–4). The use of face masks has been associated, in previous outbreaks, with the development of different headaches among healthcare providers, attributed to several mechanisms such as hypoxemia, hypercapnia, mechanical factors, and psychological stress (2,3,5).
Available information regarding PPE-associated headaches is scarce, and most studies are limited to specific occupational hazards, including healthcare providers. The authors hypothesized that increased PPE use in the present pandemic may lead to development of headaches. Thus in this study, we aimed to evaluate PPE-associated headaches during COVID-19 pandemic in the general population, in Portugal.
The first confirmed cases of COVID-19 in Portugal were reported on 2 March 2020. A State of Emergency was declared on 18 March. Since 13 March the use of masks and/or face shields has been mandatory for all people aged 10 or older in all indoor public spaces, workspaces, schools, and public transports. From October 2020 it also became mandatory to wear face protection outdoors, whenever it was impossible to maintain a distance of at least 2 meters from others, excluding family members (6).
Methods
In this cross-sectional cohort study a self-administered questionnaire was made available for 12 weeks, from 12 September to 5 December 2020. This survey targeted individuals over 14 years of age using at least one PPE due to the COVID-19 pandemic, and who voluntarily decided to participate in the study. Thus, we targeted a large non-probabilistic convenience sample of the national population during the COVID-19 pandemic. The study and survey link were announced on websites and social media platforms of the Portuguese Headache Society and MiGRA Portugal, the Portuguese headache and migraine patient’s organization; some traditional media (on-line health sites and newspapers) also participated voluntarily in advertising the study and sharing the survey link. The collected data was anonymous, and the link was hosted in a secure domain. The survey was developed by the authors considering the investigation question, experience in clinical practice and feedback received from patients in medical visits and patient´s association. The main purpose of the survey – to assess the impact of headaches in the present pandemic and its potential association with PPE – was also announced with the survey. We followed CHERRIES checklist for web-based surveys and report more details about the nature of the survey, including the sampling methods in the Supplementary data (7).
Approvals from the Hospital Ethics Committee and data protection officer of Luz Saúde were previously obtained.
The survey questionnaire had five parts: (1) demographic data (age, gender, district of residency, and whether or not a healthcare worker); (2) PPE usage (type and duration of daily PPE use); (3) previous headache history (frequency, acute medication use, ID-Migraine in its Portuguese version which has a positive predictive value of 0.80 (95% CI 0.71–0.87) (8,9), and its modifications following COVID-19 pandemic; (4) new-onset headaches (de novo headaches, dnH) occurring after the beginning of COVID-19 pandemic (characteristics and associated symptoms of those headaches); and (5) individual strategies to minimize PPE associated headaches. Headaches were classified using the ID-Migraine score in Migraine (MH, scores 2 or 3) and Non-migraine headaches (NMH, scores 0 or 1) (8). Internal consistency of the questionnaire was validated by keeping a spectrum of discrete options, eliminating the scoring system, and having a simple multiple-choice format. The translated version is available in the supplementary data.
As there were no previous studies in similar populations available before study initiation, no formal sample size calculation was performed. However, considering the target population of all Portuguese aged 14 or older (around 9 million – 8.989.849), we estimated the need of at least 4158 participants (400 per week, over 12 weeks) to obtain a confidence level of 99% (for a confidence interval of 2) (10).
This is the first report regarding this data.
Statistical Analysis
The exploratory data analysis included descriptive statistics with absolute and relative frequencies, mean and standard deviation (SD), or median and interquartile range (IQR). Statistical tests for the comparison of mean or distributions included the Mann-Whitney Test, the Chi-square or Fisher's exact test, and the Kruskal-Wallis test as appropriate for variable type. Kolmogorov-Smirnov test was used to assess normality. Cases with missing values were excluded in each analysis. Significance was set at the two-tailed 5% level (p < 0.05). Multiple logistic regression model was constructed to determine the factors predicting dnH. In addition to age and gender, clinically relevant variables and/or variables with a value of p < 0.05 in intergroup comparisons were considered to include to the multiple logistic regression model. For comparison purposes we decided to use variables that combined all PPEs data (specifically average duration and frequency of PPE use).
Multicollinearity was tested using variance inflation factor (VIF). VIF of 1 to 5 was considered accepted enough to warrant corrective measures. IBM SPSS Statistics v25 (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
Data Availability
Unpublished data will be available (anonymized) to be shared by request from any qualified investigator.
Results
A total of 5064 responses were collected, which attained our goal of a confidence level of 99% for the Portuguese population. Most questions had a completion rate above 87% (non-responses rate ranging from 0–12.7%). Ninety-point six percent (4562/5034) of the respondents were women. Average age was 37.2 ± 11 years old (14–79) and most of the participants were from two of Portugal's high-risk districts for COVID-19 (Lisbon 1553/5064 31.2%; and Porto 858/5064–16.9%), which are the two most populated urban areas in our country. Almost 20% of the respondents were healthcare professionals (HCPs) (993/5046) and more than two-thirds (73.7%) were working in office (3442/4476), while 12.1% (566/4476) were teleworking at the time the survey was answered. No differences in age, gender and HCP status were found between respondents of different districts, except when working in office, that was less likely if the responders lived in Lisbon (1115/1553, 71.8%, P < .001) (Figure 1).

Geographical distribution of the participants and demographic data.
PPE usage patterns
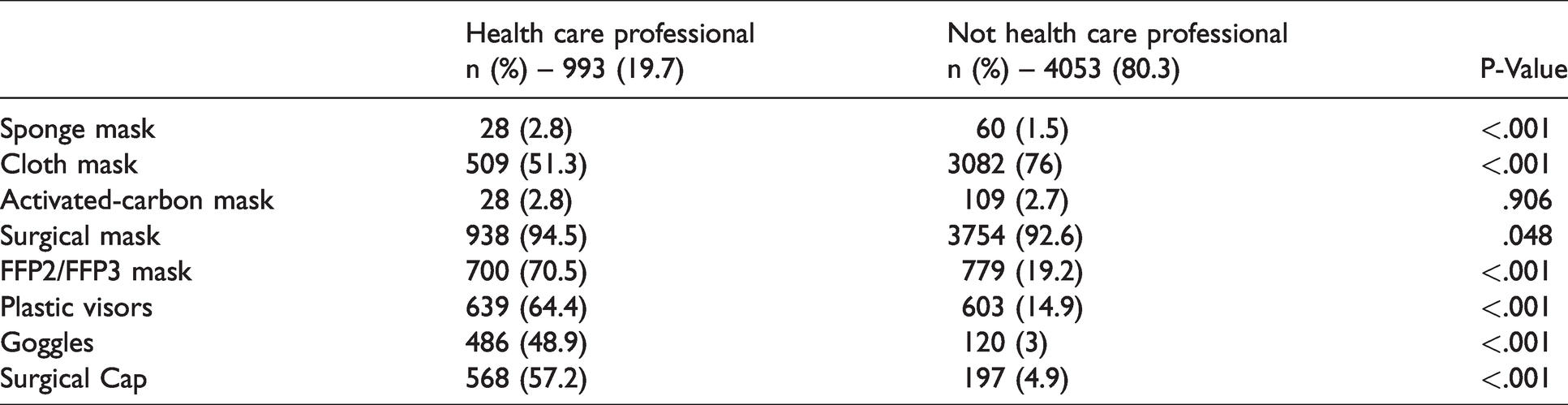
Face mask was the predominant PPE used: over 90% of the participants wore surgical masks (4707/5020) with around 71% wearing cloth/social masks (3603/5020). FFP2 and/or FFP3 masks were used less frequently (1699/5020–33.6%; P < .001) and mainly by HCPs (P < .001) (Figure 2 and Table 1). Regarding protective eyewear, 24.5% used plastic face visors (1240/5020) and 12% goggles (606/5020). Protective eyewear was also used more frequently by HCPs (P < .001). Most participants used two or more different PPEs (3899/5018–77.7%), either more than one type of face mask or a combination of face mask and eyewear. On average, participants used a face mask for 26.8 days over 30 days, with a mean of 9 h30 min per day. Protective eyewear was worn 18.6 days over 30 days, on average 5h12 min per day. The combined use of all PPE was worn on average of 24.1 days (1–30 days), with a mean of 6h36 min per day (10 minutes – 20 hours). Duration of PPE use was longer in HCP subgroup, with a mean of 7h20 min per day (P < .001).

PPE usage pattern.
PPE usage pattern between health care professionals and not health care professionals (percentage).
Course of pre-existing headaches during COVID-19 outbreak
Lifelong headache incidence was reported by 98.7% of the respondents (4595/4655–98.7%), while 72.2% reported having headaches regularly (2980/4125). Prevalence of migraine headache (MH) was 61.7% (2547/4125), while non-migraine headache (NMH) was 5.6% (233/4125). Comparing with NMH participants, respondents with MH were more frequently female (P < .001) and had more frequent, severe and longer lasting headache (P < .001).
More than 90% of these patients reported headache worsening following the onset of the COVID-19 pandemic. The negative impact was reported in all aspects, including headache frequency, intensity, duration, and medication efficacy with most participants considering it likely or very likely that such aggravation was related to PPE usage (Figure 3).

Modification in headache pattern with regular PPE use since the COVID-19 outbreak and personal impressions of its association with PPE.
Headaches arising during COVID-19 pandemic/following PPE use
More than half of the participants (2476/4420–56%) reported the onset of a different headache type following PPE use. Pre-existing headache was present in 58.5% (1226/2097) of these participants, mostly MH (1118/1226, 91.2%), but subjects were able to differentiate these from previous headaches. The majority described these dnH as moderate (1500/2193–68.4%), bilateral (1431/3266–43.8%) on the forehead (1549/2474–62.6%), mostly as a sensation of pressure at the affected sites (1377/3270–41.1%), and the majority had associated symptoms such as photophobia (1236/2477–49.9%), phonophobia (1128/2477–45.6%), and aggravation by routine physical activity (1027/2477–41.5%), neck tenderness (984/2477–38.3%), nausea (917/2477–37%), blurred vision (743/2477–30%), and osmophobia (549/2477–22.2%). Less frequent associated symptoms (n=322/3267, 9.9%) included anxiety, dizziness, somnolence, panic attacks, thirst, and attention deficits (Figure 4). Most of these subjects wore face masks (2152/2448–87.9%) and some of them used eyewear (637/2448–26%). Type of mask had no influence (Table 1 of Supplementary data). Headache characteristics among different PPE were similar (Table 2 of Supplementary data).

Characterization of de novo headaches following PPE use.
Selected baseline demographic and clinical characteristics of participants with and without de novo headache (dnH).
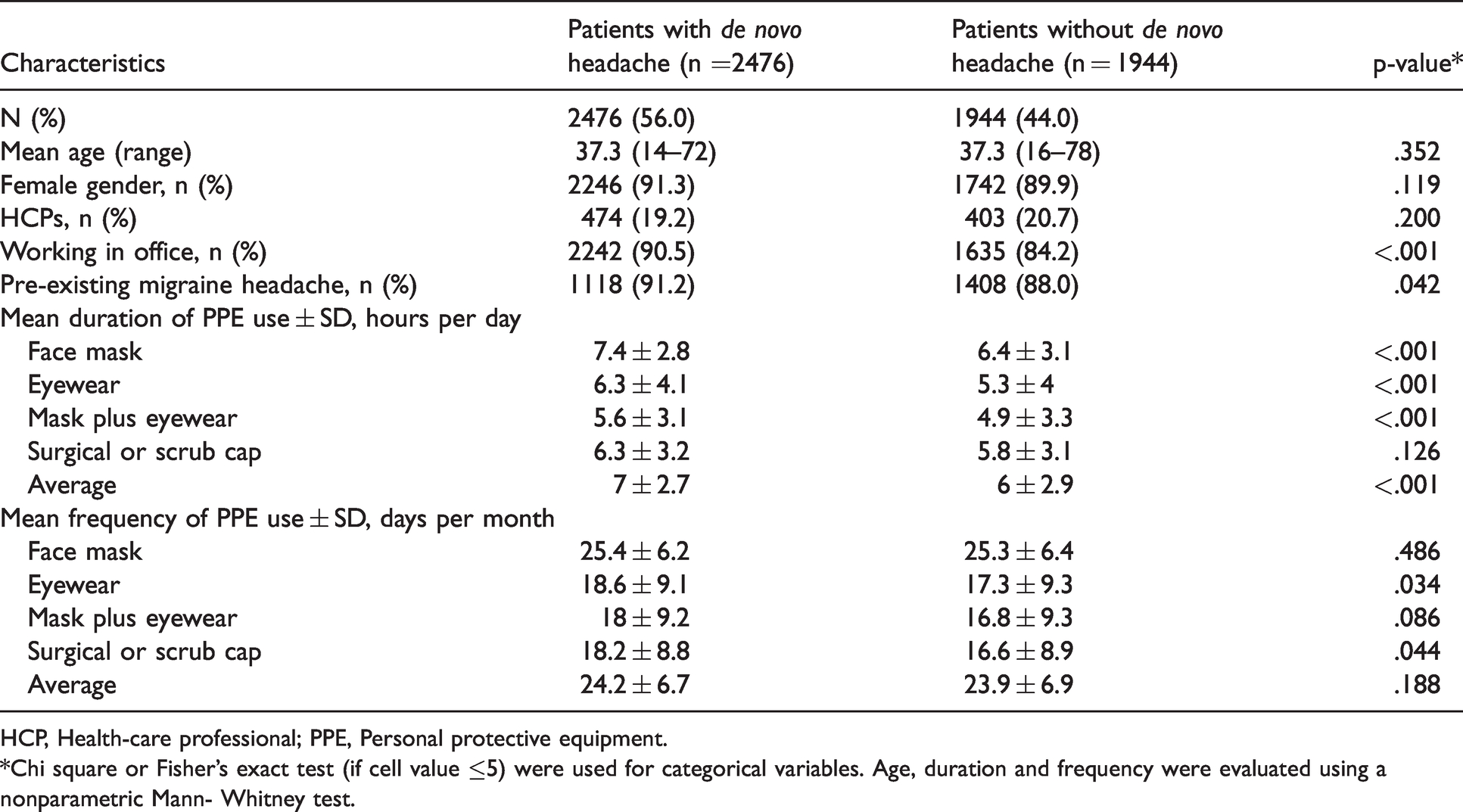
HCP, Health-care professional; PPE, Personal protective equipment.
*Chi square or Fisher’s exact test (if cell value ≤5) were used for categorical variables. Age, duration and frequency were evaluated using a nonparametric Mann- Whitney test.
Comparing the characteristics of dnH between migraine and non-migraine participants, individuals without history of migraine reported more frequently a mild to moderate headache (p < .005) with a sensation of pressure at the affected sites (p < .05). On the other hand, migrainous features were more frequently reported by the migraine group: vomiting (p < .005), photophobia (p < .005), sonophobia (p < 0.05), aggravation by exercise (p < .05) and throbbing quality (p<0.05). Bilateral headache was more frequent amongst non-migraine participants; however, pain location did not reach statistical differences between the two groups.
These headaches initiate on average of 3 h 24 min into PPE wearing and subside on average of 3 h 54 min after its removal irrespective of PPE type.
Most participants reported a dnH frequency between 4–15 days/month (1118/2183–51.2%) and needed acute drug treatment (1638/2178–75.2%) to control it. Most respondents considered it likely (1301/3273–39.7%) or very likely (1638/3273–50.1%) that dnH were PPE related.
While for most participants the ideal solution for alleviate PPE-associated headaches would be to not use it, due to the current pandemic they kept wearing PPE despite the headaches. However, spontaneous preventive measures and strategies to relieve dnH were undertaken by most of the study population (1651/2515–65.5%), such as regular breaks with PPE removal (1340/2515–53.3%), frequent PPE change during the day (952/2515–37.9%), use of ear saver plastic connectors on masks’ elastic loops (399/2515–15.9%), and skin moisturizing (417/2515–16.6%). The participants were also asked to suggest preventive measures through an open-ended question. Answers included: increasing awareness of migraine/headache in workplace, use of aromatherapy and essential oils, and limit the time spent engaging with COVID-19 news, removing anxiety-provoking information from social media feeds.
Comparison of participants with and without de novo headaches following PPE use
The group of participants with dnH had more individuals working in their office (2249/2476, 90.5% vs 1635/1944, 84.2%, P < .001), higher frequency of pre-existing migraine (1118/1226, 91.2% vs 1408/1600, 88%, P < 0.042), and longer periods of PPE wearing, on average an hour longer (7 ± 2h42 min per day vs 6 ± 2h54 min per day, P < 0.001). They also reported more frequent protective eyewear use (18.6 ± 9.1 days per month vs 17.3 ± 9.3 days per month, P = .034), having similar frequency of face mask use than those who did not report dnH (25.4 ± 6.2 vs 25.3 ± 6.4) (Table 2).
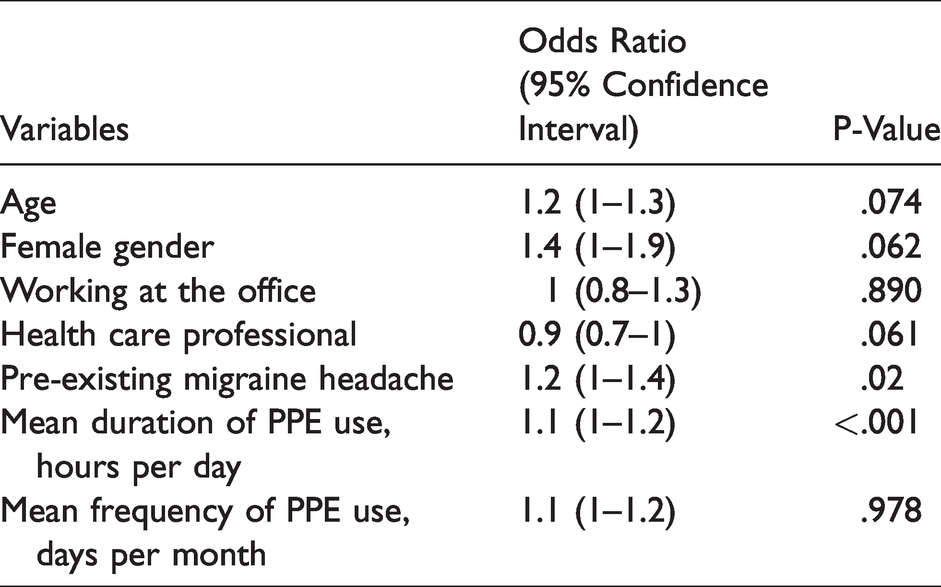
Multiple logistic regression analysis only found the mean duration of PPE use and pre-existing migraine headache to predict higher risk of dnH. More specifically, participants with previous history of migraine had 20% more risk of developing dnH (OR of 1.2, 95% CI 1–1.4), and for about each hour of PPE use the risk of dnH increased by 10% (OR of 1.1, 95% CI 1–1.2) (Table 3).
Multiple logistic regression analysis of independent factors and PPE usage factors associated with de novo headache.
Discussion
In this study, we investigated PPE-associated headaches among a large non-probabilistic convenience sample of the national population during the COVID-19 pandemic. Fifty-six percent of the participants (2476/4420) reported dnH, the majority attributing them to PPE usage. Additionally, 97% (1814/1870) of the participants with pre-existing headaches reported exacerbation of their headaches, having more frequent, more severe and longer headaches, that were more resistant to their usual acute medication. Duration of PPE usage was the strongest predictor of dnH. Most participants described dnH as moderate, bilateral with a pressure quality. As a significant part had migrainous symptoms and migraine was a risk factor for its development, some of these dnH may correspond to migraine headaches. However, more than half of the respondents did not have migrainous symptoms and 41.5% of the participants with dnH did not have previous migraine. Additionally, sub analysis of dnH characteristics between migraine and non-migraine participants showed that migrainous features were indeed more frequent among participants with previous migraine, while participants without migraine reported dnH as moderate with a pressure quality. A possible etiological explanation for dnH could be that it may be due to the compression of pericranial soft tissues (11).
Previously included on Cranial neuralgias and central causes of facial pain chapter of the ICHD-2 criteria (12), compression headaches are now classified as Other primary headache disorders in the ICHD-3 (13). Although significant overlap of this entity exists with both primary (tension-type headache) and secondary headaches (cervicogenic headache), in most cases headache attributed to external compression corresponds to a compression headache. The diagnosis of compression headache requires the existence of a sustained compression of the forehead or scalp and the close temporal association between external-pressure and headache (within 1 hour and resolving within 1 hour after external compression is relieved) (13).
The pathophysiological mechanisms of compression headaches are uncertain but thought to be related to the compression of nerve endings or branches of the trigeminal and occipital nerves (2).
Certain populations (such as construction workers and military personnel) may be at particular risk of developing this type of headache due to prolonged use of headwear or helmet (2,3). Interestingly, studies focusing on military personnel found that helmets with different designs influenced both the occurrence of headache and its characteristics, underlying the association between individuals’ comfort and the likelihood of headache (3). Additionally, these studies also documented primary headaches (migraine, tension-type headache, and occipital neuralgia) among these populations, with some helmet-triggered attacks, which were distinct from compression headache episodes. The authors suggested that if the stimulus causing the pain were prolonged enough, external compression could lead to a more severe migrainous headache in predisposed patients (2).
Regarding our sample using PPE, compression can be applied by eyewear, headgear and mask elastic loops. In our study, the participants mentioned spontaneous relief after PPE removal and spontaneously reported the use of ear savers to help, which supports this mechanical mechanism. There are reports of feeling tightness and experiencing discomfort on the ear lobes by nurses wearing N95 respirators during clinical procedure (11). These perceptions negatively influenced nurses’ appeal for proper mask use, directly affecting their compliance. However, timing to headache triggering and relief (average of 3.9 h) were longer than described in compression headache, which suggests the existence of additional interacting factors.
Apart from the mechanical effects, adverse effects of PPE such as breathing difficulties with periods of hypoxemia and hypercapnia have also been reported (14). It is proposed that mask-related carbon dioxide (CO2) retention may influence cerebral hemodynamics, increasing cerebral blood flow which can lead to headaches (14). However, several studies show that despite CO2 elevations, and lower O2 saturations these changes are not likely to be clinically relevant, as both CO2 and O2 levels are kept within healthy normal ranges (15,16). Another concern with prolonged mask use is that PPE may be an obstacle to drinking regularly and to maintaining adequate hydration, which can also contribute to headache (17).
Data from a past pandemic study, the 2003 SARS outbreak in Singapore, where healthcare workers mandatorily wore the protective N95 respirator, included the report of new-onset face mask-associated headaches in about a third of healthcare providers, from which 62.7% had no pre-existing headaches. In this study, pre-existing headaches and prolonged duration of N95 respirator use were also the most important risk factors for headache development (5).
Several studies have highlighted the association between headache and PPE, with a prevalence ranging between 28–81% (14,18–21). Particularly, one study showed that of the new-onset symptoms following PPE use, the headache was the most frequent one amongst HCPs (21). Several factors were associated with developing de novo headaches, including extended use of PPE (both frequency and duration), the combination of masks and protective eyewear, and pre-existing headaches (18,21,22). The authors concluded that increased PPE usage negatively influenced background headaches in those with previous primary headaches. All these studies findings are in line with our data supporting such association.
PPE reduces the risk of COVID-19 transmission and adequacy of PPE is a risk factor for COVID-19 infection (23), so avoiding PPE use is not at all advisable, regardless of its association with headaches. While, most participants reported strategies that relieve dnH associated with PPE, the impact of such strategies on headache severity and frequency is not established. Considering the consistency of the association of duration of PPE use as major risk factor for dnH in all observation studies, a reasonable strategy would be to recommend regular breaks for people in need of wearing PPE for long periods. Additional preventive strategies, when appropriate, could include choosing the type of mask with less impact, the use of ear savers and teleworking. Studies evaluating efficacy of the physical preventive measures and of acute or preventive drug treatment for such headaches are needed.
Most previous studies investigated PPE-associated headaches among small samples of health-care workers. Major strengths of our study include the large sample size and the wide target population, not limited to HCPs. Our sample was not representative of the general population, however, as it shows a clear female predominance and high migraine prevalence. Gender is a known risk factor for most headache disorders, but in this study a participation bias is very likely not only because women are generally more interested in health topics, exhibit more active information-seeking behavior, are more likely to volunteer to participate in health questionnaires, and seek medical attention more frequently (24), but also because the survey was promoted by the local headache and migraine patient’s association, which has a clear female preponderance. This and a motivation to answer bias also explains the higher prevalence of pre-existing headache in our study contrasted with other studies (18), also higher than expected for Portuguese population (61.7% vs 8.8%) (25). We also need to consider the existence of confounding factors such as psychological stress and sleep disturbances related to the pandemic context, that could contribute both to the development of dnH and to PPE maladaptation. Additionally, the subjectivity of the participants answers has to be considered, as pain perception is dependent on individual differences (26).
Somehow in contrast with our findings, previous studies showed an overall improvement of headache impact in migraine patients during the present pandemic (27). However there are several aspects that may contribute to this discrepancy. First, some of these studies were performed in the beginning of the pandemic and consequent lockdown which prevented the analysis of both lockdown and pandemic medium to long-term effects such as poor sleep quality and high levels of anxiety, known migraine-triggers (28). Second, they included only individuals staying at home during lockdown, while most of the participants of our study were working in office at the time of the survey. Lastly, these studies did not consider the effect of PPE use which is our main goal.
We acknowledge several additional limitations to this study: firstly, being an online questionnaire mainly spread by web and social media there is an additional sampling bias, missing out people who do not use the internet as much such as older people and socially isolated individuals (13). Secondly, a self-administered questionnaire could have been affected by the recall bias. However, the ongoing exposure to PPE and the magnitude of the COVID-19 pandemic would have reduced the effect of this bias. Thirdly, medical history other than pre-existing headaches was not explored, so we could not assess the impact of other risk factors associated with new-onset symptoms of PPE use, such as smoking and excessive body weight (21). Lastly, when considering the aggravation of pre-existing headaches, especially migraine, we also have to consider other trigger factors such as sleep deprivation, physical and emotional stress, anxiety and increase in drug use (anxiolytics, pain killers) also common during the present pandemics (29).
In conclusion, prolonged PPE use seems to be a risk factor for the development of dnH and exacerbation of pre-existing headaches, migraine in particular. While the benefit of PPE use is unquestionable, there are potential strategies to make wearing a mask more comfortable. Longitudinal controlled studies are needed to evaluate the natural history and treatment options of PPE-associated headaches.
Clinical Implications
Application of a self-administered questionnaire though an online survey available during the second semester of 2020. Main goal was to evaluate the development of PPE-associated headaches during COVID-19 pandemics in the general population. Of 5064 participants, 56% had de novo headaches (dnH). The strongest predictive factors for dnH were the duration of PPE usage and pre-existing migraine. Most migraine and headache patients reported aggravation of pre-existing headaches, with most patients attributing that augmentation to PPE. Strategic measures targeting PPE use may help preventing these headaches.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024211067787 - Supplemental material for Headaches and the use of personal protective equipment in the general population during the COVID-19 pandemic
Supplemental material, sj-pdf-1-cep-10.1177_03331024211067787 for Headaches and the use of personal protective equipment in the general population during the COVID-19 pandemic by Renato Oliveira, Madalena Plácido, Liliana Pereira, Sara Machado, Elsa Parreira and Raquel Gil-Gouveia in Cephalalgia
Footnotes
Acknowledgments
We thank Joaquim Gil for drafting and editing Figures 2 and ![]() .
.
Conflicts of interest/competing interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.