
Abstract
Objective
The objective is to summarize the knowledge on the epidemiology, pathophysiology and management of secondary headache attributed to SARS-CoV-2 infection and vaccination; as well as to delineate their impact on primary headache disorders.
Methods
This is a narrative review of the literature regarding primary and secondary headache disorders in the setting of COVID-19 pandemic. We conducted a literature search in 2022 on PubMed, with the keywords “COVID 19” or “vaccine” and “headache” to assess the appropriateness of all published articles for their inclusion in the review.
Results
Headache is a common and sometimes difficult-to-treat symptom of both the acute and post-acute phase of SARS-CoV-2 infection. Different pathophysiological mechanisms may be involved, with the trigeminovascular system as a plausible target. Specific evidence-based effective therapeutic options are lacking at present. Headache attributed to SARS-CoV-2 vaccinations is also common, its pathophysiology being unclear. People with primary headache disorders experience headache in the acute phase of COVID-19 and after vaccination more commonly than the general population. Pandemic measures, forcing lifestyle changes, seemed to have had a positive impact on migraine, and changes in headache care (telemedicine) have been effectively introduced.
Conclusions
The ongoing COVID-19 pandemic is a global challenge, having an impact on the development of secondary headaches, both in people with or without primary headaches. This has created opportunities to better understand and treat headache and to potentiate strategies to manage patients and ensure care.
Introduction
Coronavirus disease 2019 (COVID-19) is the symptomatic presentation of the infection of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)(1). Since its beginning, the COVID-19 pandemic has made headache unprecedentedly relevant for the global population. Headache is a common characteristic and disabling symptom of COVID-19 that has affected almost 500,000,000 people to date (2). Headache may present with a chronic pattern in what is known as long-COVID syndrome. It has been also described in relation to SARS-CoV-2 vaccinations. The COVID-19 pandemic has also impacted the care of people suffering from headache disorders.
With this review, we aim to analyze available evidence in order to transform the lessons learned during the pandemic into an opportunity for the headache field. We will first focus on secondary headaches: headache attributed to SARS-CoV-2 infection, both during the acute and post-acute phase of COVID-19, headache attributed to SARS-CoV-2 vaccinations and other secondary headache disorders in this setting. We will then address primary headache disorders and the effect of SARS-CoV-2 infection, vaccination and pandemic measures developed to handle them (Figure 1).

Primary and secondary headache disorders in the setting of COVID-19 pandemic.
Secondary headaches & COVID-19
Headache attributed to SARS-CoV-2 infection
SARS-CoV-2 is a new ribonucleic acid (RNA) virus belonging to the genus Coronavirus. In this review, we refer to Headache attributed to SARS-CoV-2 infection as the headache caused by systemic SARS-CoV-2 infection that cannot be accounted for by any other International Classification of Headache Disorders-3rd edition (ICHD-3) diagnosis (3). Headache can be observed in two phases of COVID-19: the acute (from symptoms onset to week 4) and post-acute (from week 5 onward), that is when the initial infection has resolved but patients still report persisting symptoms or experience new ones that have no other explained cause (4–6). Definitions are fully reported in Table 1.
Epidemiology, characteristics, pathophysiology, prognosis, treatment and differential diagnosis of headache attributed to SARS-CoV-2 infection and vaccination.
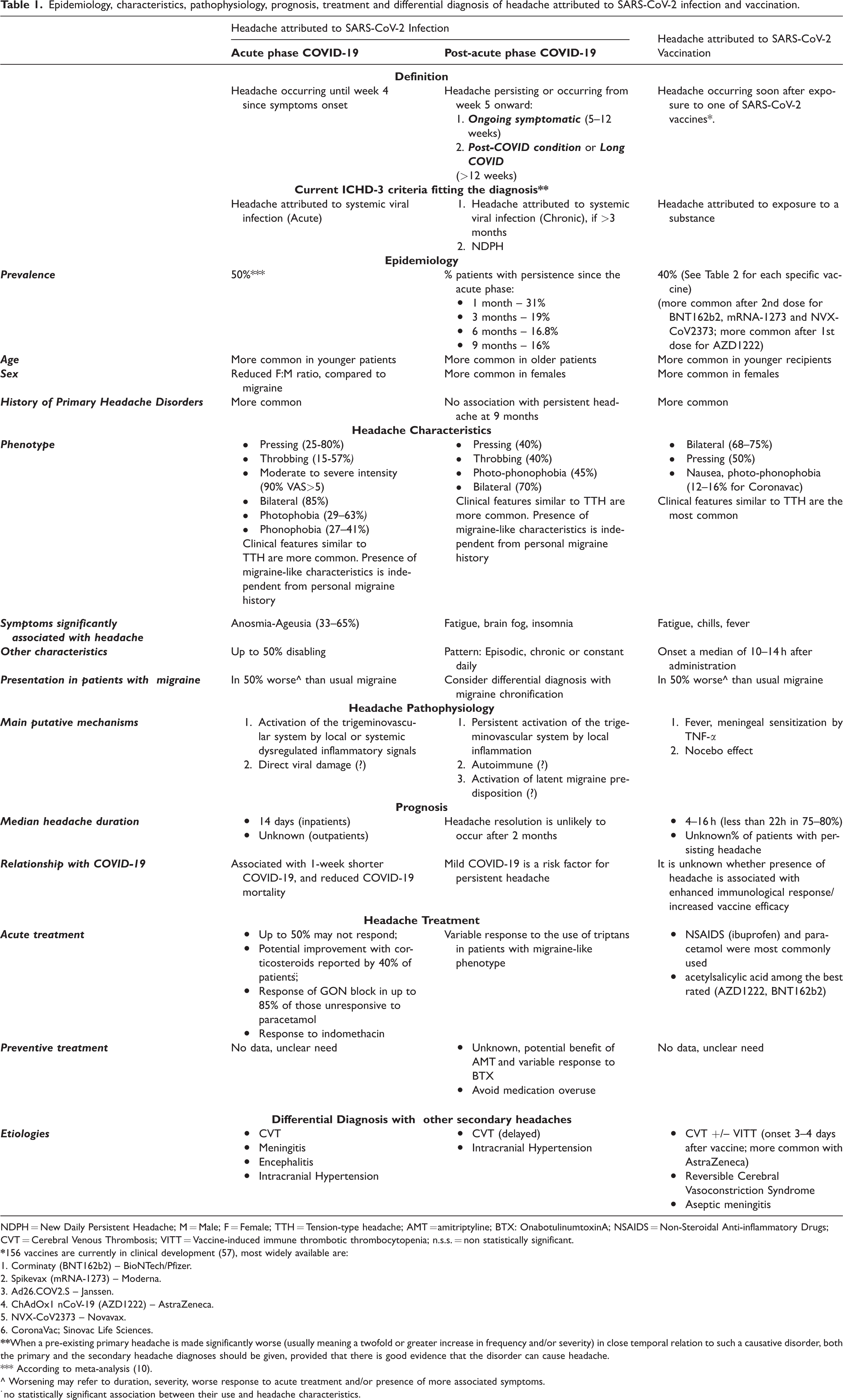
NDPH = New Daily Persistent Headache; M = Male; F = Female; TTH = Tension-type headache; AMT = amitriptyline; BTX: OnabotulinumtoxinA; NSAIDS = Non-Steroidal Anti-inflammatory Drugs; CVT = Cerebral Venous Thrombosis; VITT = Vaccine-induced immune thrombotic thrombocytopenia; n.s.s. = non statistically significant.
1. Corminaty (BNT162b2) – BioNTech/Pfizer.
2. Spikevax (mRNA-1273) – Moderna.
3. Ad26.COV2.S – Janssen.
4. ChAdOx1 nCoV-19 (AZD1222) – AstraZeneca.
5. NVX-CoV2373 – Novavax.
6. CoronaVac; Sinovac Life Sciences.
*** According to meta-analysis (10).
^ Worsening may refer to duration, severity, worse response to acute treatment and/or presence of more associated symptoms.
The pandemic provided a global opportunity to study millions of patients and to understand the distinct features and relevance of headache manifestations secondary to this RNA virus. The majority of clinical studies were conducted during the first wave of the pandemic, included mainly inpatients and focused on headache frequency and COVID death or survival. Therefore, data on the presentation of headache in the outpatient population and in the setting of new SARS-CoV-2 variants and treatments that emerged over the course of pandemic, are still limited. However, available studies had the advantage of reflecting the natural course of SARS-CoV-2 original strain only, without any vaccine related interactions.
Acute phase of COVID-19
Epidemiology
Reported prevalence of headache during the acute phase of COVID-19 is extremely variable ranging from 10% to 74% (7,8), even meta-analyses yielded different results such as 10% vs 50% (9,10). This is mainly due to differences in design (retrospective vs. prospective), main focus (headache vs. general COVID-19 symptoms), researchers (neurologists vs. non-neurologists), data collection (surveys vs. in-person interviews), study population (outpatients vs. inpatients) and ethnicity among studies. One study observed similar prevalence of headache between COVID-19 inpatients and outpatients (11). Patients with headache are younger than those without it (8,12,13), while controversies still exist in regards to sex, specifically, whether women may be more likely to experience headache in the acute phase or not (8,13–15). History of primary headache disorders, specifically migraine, is more common in patients reporting headache as an acute symptom of COVID-19 (8,12) (Table 1).
Clinical Characteristics
Most of COVID-19 patients with headache fulfill the 9.2.2 definition “Headache attributed to systemic viral infection” in ICHD-3 (16). Headache usually presents concomitantly with other COVID-19 symptoms, although in 25% of patients it may be the presenting sign (8,13,14,17) and it may occur also in the absence of other symptoms (18). The most common clinical presentation of headache in the acute phase is as a diffuse, moderate to severe, pressing pain although throbbing quality, pain worsening with movement, photophobia/phonophobia, and nausea/vomiting may be seen additionally (8,12–14,18). In up to 50% of cases, headache is severe, constant and responds poorly to acute pain medications (8,13,19), thus correlating with a relevant disability. The phenotype of headache associated with COVID-19 meets criteria for migraine in 25% of patients and for tension-type headache in 54% of patients (16). These two phenotypes have been described in several studies (8,13,20–22). Interestingly, a migraine phenotype may also be present in patients without a personal history of migraine (8,16). The presence of red flags (e.g. sudden onset, etc.) may be commonly reported and may indicate the need for further investigations (17). Regarding other neurological symptoms, co-existence of myalgia, anosmia and/or ageusia seem highly associated with COVID-19 headache (8,13,14,20,23) (Table 1).
Pathophysiology
Headache as a symptom frequently denotes the activation of the trigeminovascular system. Headache in the context of COVID-19 reflects specific pathophysiological mechanisms induced by the interaction of SARS-CoV-2 with the host (8,24). This RNA respiratory transmitted virus enters the host cell using the membrane angiotensin-converting enzyme 2 (ACE2) receptor, initiating a cascade of pathogenic and dysregulated inflammatory events, involving, amongst others, the innate immune system, NOD-like Receptor Protein 3 (NLRP3) inflammasomes and pro-inflammatory molecules such as IL-6, with a local and remote impact on the vasculature and different tissues (25). This activated immune response can lead to an exaggerated systemic inflammation known as cytokine storm, which has a central role in COVID-19 pathogenesis and severity (26). Some of these mechanisms may be relevant for COVID-19-related headache, although inflammatory cytokine levels were inconsistent (8,12,27,28). It is worth mentioning that only one study compared CGRP levels between COVID-19 patients with and without headache, observing unchanged serum levels, which may suggest a minor role for circulating CGRP in COVID-19 headache (27).
Among other pathophysiological mechanisms, direct invasion of neuronal tissues by SARS-CoV-2 in the upper respiratory system seems unlikely (29), as transmembrane ACE2 is not expressed in olfactory receptor neurons and its expression in the trigeminal nerve has not been clearly demonstrated. In line with this concept, in a post-mortem study of 33 cases, ACE2 immunoreactivity was not seen in brain specimens (30) and neuropathological evaluations of 438 cases did not prove a direct brain invasion of the virus (29). Nevertheless, direct viral nervous system invasion is still an unresolved issue as RNA copies were detected with polymerase chain reaction (PCR) in the trigeminal ganglia of three patients (30).
The most likely hypothesis is that SARS-CoV-2 infection of the epithelium in the nasal-oral cavity mediates the release of inflammatory mediators that, in addition to causing anosmia/ageusia, may also sensitize/activate mucosal and meningeal trigeminal nociceptors, leading to headache (25,31). Additionally, viral infection of brain vascular cells and endothelium, its inflammation (endothelitis), lymphocytic infiltration, and disrupted vascular integrity may play a role in perivascular trigeminal nociceptor activation in the cephalic structures (24) (Table 1).
Prognosis and Treatment
The median duration of headache in the inpatient population is about two weeks (8,32), while it is still unclear in the outpatient cohorts. Some studies have observed that the presence of headache is associated with better COVID-19 evolution in terms of shorter COVID-19 disease duration (8), less severity (33) and lower in-hospital mortality (12,34). A recent meta-analysis of survival of 43,169 inpatients with COVID-19 has also found that headache is a marker of enhanced COVID-19 survival (35). However, not all studies have found these results (36). Future research should further investigate this matter, dealing with the possible bias that more severe cases will likely be hospitalized and intubated (and thus likely unable to report headache) (Table 1).
No specific acute treatment exists for headache in the acute phase of COVID-19. Paracetamol/acetaminophen and nonsteroidal anti-inflammatory medications (NSAIDs) are the most commonly used (8,12,19) drugs, but, as previously mentioned, up to 50% of patients are unresponsive to painkillers (Table 1). Initial concerns on the use of NSAIDs and corticosteroids during the acute phase have been resolved (37). Although any statistically significant relationship between the use of steroids and frequency, duration or intensity of COVID-19 related headache was found, one study observed headache improvement with corticosteroids in around 40% of patients (38). Headache relief was provided by greater occipital nerve blocks in 85% of 34 patients unresponsive to paracetamol (19). A retrospective case series evaluated indomethacin, showing >50% pain relief in almost all 37 treated patients within three days (39).
Post-acute phase of COVID-19 (beyond 4 weeks)
Epidemiology
Neurologic symptoms are common also during the post-acute phase and headache is no exception (40). According to the UK National Office for Statistics, an estimated 1.3 million people living in private households (2.0% of the UK population) were experiencing self-reported long-COVID as of December 2021, around 306,000 of them reporting headache (0.47% of UK population) (41). A small prospective study of 130 patients, recruited at the emergency department during the first wave of the pandemic, showed that 37.8% of patients reported ongoing headache at a six-week follow-up (8). Another large, multicentre study, pooling data from several other studies, followed 905 selected patients with headache during and after SARS-CoV-2 infection (32). After one month, 31% of patients still complained of headache, at three months 19%, at six months 16.8% and at nine months 16% (32) (Table 1).
Clinical characteristics
Similar to the headache described in the COVID-19 acute phase, most post-acute phase headaches bear features of tension-type headache or migraine. In fact, in the above-mentioned study of 905 patients, around 40% of subjects showed migraine-like features such as throbbing pain and 45% had photo-phonophobia (32). Surprisingly, in small case-series some patients without acute-phase headache developed migraine-like headaches at a later stage (42). The migraine-like phenotype seems to occur also independently on the presence of a prior personal or family migraine history (42). Concerning frequency patterns of headache in the post-acute phase, studies have not clarified the proportion of patients with an episodic or chronic course. However, persistent daily headaches is a common presentation (8). Finally, headache in the post-acute phase has been often reported in combination with other (neurologic) symptoms, mainly including fatigue and cognitive impairment (4) (Table 1).
Pathophysiology
A variety of reasons for the persistence of headache in the post-acute phase have been hypothesized (4). Nonspecific mechanisms include unresolved inflammation or even brain damage (43). The sensitization of second (nucleus caudalis) or third order (thalamic) neurons triggered by the trigeminovascular system activation are a plausible explanation especially for those who suffer from headaches that phenotypically resemble migraine attacks. Persistent inflammation of meninges (44) or central processes in the brain (45) may be due to the activation of microglia and release of inflammatory mediators, such as glutamate, quinolinic acid, interleukins, complement proteins, and tumor necrosis factor-α (TNF-α) (31,46,47). Increased quinolinic acid can also lead to higher glutamate levels and upregulation of NMDA receptors, causing altered neurotransmission and neuronal damage (46), that could be also responsible for other neurological symptoms (brain fog, cognitive impairment etc), often reported in combination with headache in the post-acute phase.
Other mechanisms might also be involved in the persistence of headache after the resolution of the SARS-CoV-2 infection and underscore differences in headache onset (acute phase vs. post-acute phase) or differential expression of concomitant symptoms (insomnia, anosmia and ageusia, cognitive impairment, fatigue) (42).
Recently, some authors have postulated that the persistence of symptoms after COVID-19 may be related to a constant immune activation (48), a phenomenon that may be favored by the persistence of SARs-CoV-2 antigens in some tissues despite the fact that the virus is not being isolated by PCR at a nasopharyngeal level (49). Other authors support the existence of autoimmune mechanisms generated against host epitopes in the acute phase of infection (50) as responsible for post-COVID condition.
Finally, migraine is a complex primary headache disorder which involves genetic and environmental (epigenetic) factors all having impact on intrinsic migraine thresholds. It could be possible that an acute infection might trigger migraine attacks in those with an underlying biological predisposition (32,42).
Prognosis and Treatment
Most studies report a decrease of headache incidence after the initial acute phase. Overall, based on current reports the estimation is that after 12 weeks <20% will still suffer from any kind of headache (32). Nevertheless, according to a Spanish study, after two months patients that are still reporting headache are unlikely to see a remission in the following months (32). In this study, risk factors for persistent headache after nine months were advanced age, female sex and, surprisingly, a milder COVID-19 infection (32) (Table 1).
For a successful treatment, in general, it seems important to consider the phenotype of the headache, whether there is an underlying (former) primary headache, overuse of acute pain medications and comorbid post-COVID condition. It has been suggested that up to 30% of patients may suffer from difficult-to-treat headaches (8), however limited data is available on the best preventive treatments. Amitriptyline could be potentially beneficial according to a recent study (51). One case series reported variable response to amitriptyline and onabotulinumtoxinA (42) (Table 1). Furthermore, medication overuse headache (MOH) might develop as secondary headache if patients are not treated and educated properly.
Other secondary headaches in the setting of SARS-CoV-2 infection
In the acute phase, cases of meningitis and encephalitis presenting with headache have been described (52) as well as delayed headache attributed to intracranial hypertension (53) and to cerebral venous sinus thrombosis (CVT) (54). CVT may also occur during the post-acute phase (55,56) (Table 1). Although uncommon, a careful clinical evaluation of patients with headache is fundamental to rule out all these possible secondary causes (56).
Headache attributed to SARS-CoV-2 vaccinations
Several vaccines have been developed against SARS-CoV-2 (57). Their main platforms are reported in Table 2. Headache represents the most frequently reported neurological adverse event (58), which usually lasts a few hours to a few days. Headache developing in relation to a vaccination is not a new phenomenon, being commonly reported in the setting of well-known vaccines, such as influenza (59). At present, no specific diagnostic criteria exist for this headache type but the 8.1.11 ICHD-3 criteria for “Headache attributed to use of or exposure to other substance” could be used (3). Here we summarize data on headache following vaccination with the most frequently used SARS-CoV-2 vaccines.
Headache incidence in pivotal randomized multicentre phase-3 studies on SARS-CoV-2 vaccinations.

*estimated according histogram.
Epidemiology: Headache in placebo-controlled vaccination trials
The headache incidences found in the pivotal randomized multicenter phase-3 studies on Corminaty (BNT162b2) from BioNTech/Pfizer (60), Spikevax (mRNA-1273) from Moderna (61), AZD1222 (ChAdOx1 nCoV-19) from AstraZeneca (62,63), Ad26.COV2.S vaccine from Janssen (64), NVX-CoV2373 from Novavax (65), and CoronaVac from Sinovac (66) are shown in Table 2. A meta-analysis of four vaccination phase 3 trials found headache in 29.5% of participants, compared to 21.0% in the control group (p<0.001) (67). Interestingly, headache is more frequent in younger recipients. Among vaccinations that have to be performed two times, there usually is a higher incidence of headache after the second dose compared to the first dose, except for AZD1222 which has higher incidence after the first dose compared to the second dose (Table 2).
Clinical characteristics
Göbel et al. (68) used online questionnaires in multicenter observational vaccinated cohorts. A total of 2464 participants reporting headache after vaccination with the AZD1222 vaccine was included. Headache was reported to occur 14.5 ± 21.6 hours after vaccination and lasted 16.3 ± 30.4 hours. A bilateral localization was described by 75.8% of participants, 50.4% reported a pressing quality and 37.7% a dull-pain character. Headache intensity was severe in 38.7% of patients, moderate in 35.2%, or very severe in 15.5%. The most frequent symptoms accompanying headache were fatigue (44.8% of subjects), chills (36.1%) fever (30.4%) and weakness (28.2%). Symptoms reminiscent of migraine occurred sometimes in form of aggravation of pain during physical activity and sensitivity to noise and light. The same group of researchers analyzed headache after vaccination with BNT162b2 mRNA vaccine (69) and observed similar headache characteristics. Sekiguchi et al. also investigated headache following vaccination with the BNT162b2 mRNA vaccine (70). Headache started at a median of 10 hours after the first dose of the vaccine and 12 hours after the second one. The median duration of headache was 4.5h after the first and 8h after the second dose of the vaccine. Bilateral headache was reported by 68.6% and 74.4% participants after the first and second shot, respectively. Altogether, 71.2% of the post-vaccine headache attacks exhibited clinical features of tension-type headache based on ICHD-3 (3) (70). Ekizoglu et al. (71) collected data from 1819 healthcare personnel, mostly vaccinated with inactivated virus (CoronaVac; Sinovac Life Sciences). Headache was reported with significant female predominance (36.1% vs. 19.3%), accompanied by symptoms of nausea, photo- and phonophobia in 12.1–16.9% (71) (Table 1).
Pathophysiology
The pathophysiological mechanisms of vaccination-associated headache are unclear. It can be speculated that headache and the accompanying symptoms like fever, chills, fatigue, weakness and joint pain may be related to the development of the immune response to the produced spike protein after mRNA vaccination (68). Indeed, fever has been found correlated with the number of SARS-Cov-2-neutralizing antibodies in the patients’ plasma (72). Especially after the second vaccination with mRNA vaccines, where fever and headache were more frequent, CD4+ T-cell responses with expression of Th1 cytokines like TNF-α and IL-2 have been seen (73). TNF-α may sensitize meningeal nociceptors (74) and stimulate the synthesis of the migraine-associated calcitonin gene-related peptide (75), while IL-2 is rather antinociceptive according to preclinical headache models (76). The involvement of cytokines in headaches associated with SARS-CoV-2 vaccination cannot be explained by high levels of pronociceptive cytokines like interleukin 6 (IL-6) as found in COVID-19 infections (77). In controlled studies, adjuvants based on water-in-oil emulsions such as ISA 51 have been reported to cause headache, myalgia, fever and fatigue in nearly 10% of participants (78) but the pivotal studies have all used saline as placebo. Another aspect is a potential nocebo effect caused by the injection and the expectancy of vaccinated persons (Table 1). Amanzio et al. compared three vaccines (BNT162b2, mRNA-1273, Ad26.COV2.S) and discussed the high rates of adverse side events such as fatigue, headache and myalgia in SARS-CoV-2 vaccine randomized trials under the aspects of expectations and learning (79).
Prognosis and Treatment
Headache lasted <22 hours in 75–80% of patients after vaccinations with AZD1222 and BNT162b2 mRNA vaccines (68,69). Among all patients, 25.9% experienced headache lasting ≥3 days after vaccination with the inactivated virus (CoronaVac; Sinovac Life Sciences) (71). Data on persistent headache after SARS-CoV-2 vaccinations has not yet been published; however, the authors of this review paper have seen patients who have had it. In this setting, it cannot be ruled out that, in some patients, central sensitization may occur after an initial vaccine-induced trigeminovascular system activation, being responsible for the persistence of headache. In regards to treatment, ibuprofen was most commonly used after BNT162b2, and paracetamol was most commonly used after AZD1222 and inactivated virus (CoronaVac; Sinovac Life Sciences) vaccinations in different studied populations (68,69,71). Among multiple drugs used to treat headache, acetylsalicylic acid was rated the most effective after AZD1222 and BNT162b2 vaccination (68,69). Among those experiencing post-vaccine headache after BNT162b2, simple analgesics were used by 74.3% and 87.2% of patients after the first and second doses of the vaccine, respectively (70) (Table 1).
Other secondary headaches in the setting of SARS-CoV-2 vaccination
The most significant complication after COVID-19 vaccination is CVT. Headache, which starts a few days after vaccination and deteriorates with time, is the leading symptom. Vaccine-induced immune thrombotic thrombocytopenia (VITT) represents the main underlying mechanism of CVT after vaccination (80). The formation of anti-platelet factor-4 antibodies induces platelet activation, aggregation, and thrombosis on one side, but severe platelet consumption and thrombocytopenia on the other. A survey of all neurology hospitals in Germany conducted in April 2021 identified 62 cerebral vascular events occurring within 1 month of a COVID-19 vaccination (80). Of these, 45 patients had CVT and in 26 VITT was highly probable. The mean time interval from vaccination and neurological symptoms was nine days (range: 1–25). Most patients had been vaccinated with the AZD1222 (85.5%) and only a small number with the BNT162b2 vaccine (14.5%). No CVT were reported after vaccination with mRNA-1273 vaccine. The incidence rate ratio was higher: 9.68 (3.46-34.98) for AZD1222 vaccine compared with mRNA-based vaccines. Additional cases of CVT after AZD1222 vaccine have been reported in Scotland (81) and Scandinavia (82). These findings suggest that CVT and VITT should be considered especially following an adenovirus vector-based COVID-19 vaccine. Globally, according to data from EudraVigilance, the European system for managing and analyzing information on suspected adverse reactions to medicines, reporting rate for CVT was 1.9% for BNT162b2, 5.6% for mRNA-1273, 21.6% for AZD1222 and 11.5% for Ad26.COV2.S (83). One study including 77 cases of CVT also observed a median time interval between vaccination and CVT-related headache onset of eight days (interquartile range 7.0-9.7) (84). According to 41,700 Vaccine Adverse Events Reporting System (VAERS) reports, delayed headache three to four days after COVID-19 vaccination should be a red flag for vaccine-induced CVT or ischemic stroke (84,85). In addition, cases of Reversible Cerebral Vasoconstriction Syndrome after mRNA-1273 vaccine presenting with thunderclap headache and blurred vision (86); as well as, aseptic meningitis after BNT162b2 vaccine presenting with headache and meningeal irritation have been reported (87).
In conclusion, if a patient reports difficult to treat headache, delayed headache or associated symptoms with post-vaccine headache, a complete neurological exam is recommended, with an CTA or MRA/MRV.
Primary headache disorders and COVID-19
Effect of primary headache disorders on COVID-19
There is limited data on the presence of primary headache disorders as a possible increased risk factor for COVID-19 susceptibility, severity and/or mortality. A study on a cohort of migraine patients in Spain observed a similar prevalence of COVID-19 compared to the one of the general population (88). This preliminary finding does not seem to support an increased susceptibility to COVID-19 in people with migraine. In regards to migraine treatments, the initial concern about using renin-angiotensin system inhibitors during COVID-19 was unconfirmed (89) and anti-CGRP monoclonal antibodies also appear to be safe in a preliminary multicenter Spanish study (88).
In the future, information about susceptibility to SARS-CoV-2 infection and COVID-19 outcomes in people with a pre-existing primary headache disorder may come from genetics. Interestingly, the COVID-19 Host Genetics Initiative has found multiple genomic loci that are associated with SARS-CoV-2 infection or COVID-19 outcomes (90), and at least four of these have been described in relation to headache or migraine susceptibility: IFNAR2 (91), LINC02210-CRHR1 (92), TAC4 (93), and ICAM1 (94). A possible explanation is that migraine susceptibility genotypes may be associated with host responses to viral infections (35).
Effect of the COVID-19 pandemic on primary headache disorders
SARS-CoV-2 infection
As mentioned earlier in the review, headache in the acute COVID-19 phase is more common in people with previous history of primary headache disorders, in whom it often shows characteristics that reflect the pre-existing headache condition (95). However, currently published studies on headache in the setting of COVID-19 do not always make a clear distinction between patients with and without history of primary headache disorders, making the assessment of their relationship uncertain. Patients with a history of migraine experience longer and more severe headaches in the setting of COVID-19 which may often appear earlier than in patients without migraine (15). Headache in the acute phase is generally perceived as worse than the usual migraine in around 50% of patients (88). In the post-acute phase, higher proportions of patients with previous history of headache disorders have been observed among those with persisting headache compared to those with headache remission at short term (six weeks) (8), yet not at longer term (seven and nine months) (32,96). At seven months, around 60% of patients with previous migraine history report an increase in headache frequency and around 20% in intensity after suffering from COVID-19 (96). However, proportions of patients with worsening of their migraine were higher in those who had headache in the acute phase of the infection compared to those who did not (96). Moreover, personal migraine history seems to be associated with more fatigue as a post-COVID symptom at seven months (96).
SARS-CoV-2 vaccination
After BNT162b2 vaccination, the incidence of post-vaccination headache was almost two times higher (70), the duration longer and the pain more intense in patients with a history of primary headache compared to healthy controls (69). After AZD1222, headache duration was significantly longer in patients with a history of migraine than in those without any primary headache. Patients with migraine or tension-type headache reported significantly higher headache intensity after COVID-19 vaccination compared to participants without primary headache (68). Patients with cluster headache showed no difference compared to patients without primary headache in both studies of AZD1222 and BNT162b2 (68,69). Silvestro et al. (97) collected data about headache after four different vaccinations (BNT162b2 67.3%, AZD1222 19.5%, mRNA-1273 11.1%, Janssen 2.1%) from 841 patients with migraine. A total of 66.5% of patients reported headache after the first COVID-19 vaccine, and 57.6% reported different features compared to those usually experienced, 52.8% reported a longer duration and 50.6% higher pain intensity (97). Headache during COVID-19 or that following influenza vaccination also showed a significant association with headache following COVID-19 vaccination (ORs = 4.3 and 4.84).
COVID-19 pandemic measures (social impact)
Since the start of the global pandemic, society has been confronted with measures to prevent the SARS-CoV-2 virus from spreading. This has involved worldwide restrictions hampering daily life by closing schools, restaurants, shops and, to a certain extent, hospitals. In contrast the increase of COVID-19 related demand, postponed or swiftly transformed healthcare to online solutions. This was also the case for most patients with primary headache disorders.
Impact of lockdown on patients with migraine
The course of migraine attacks may be modified by lifestyle and behavioral factors. The COVID-19 pandemic led to extremely unusual circumstances with lockdown measures, altering people’s behavior. In a large Dutch study, almost 600 patients diagnosed with migraine filled in headache E-diaries for at least 28 baseline days before and the first 28 days of lockdown (98). This large longitudinal cohort study showed that short-term lockdown can positively impact migraine specific outcome measures and general well-being. This is presumably a combined result of working from home, scaling down demanding social lives and freedom to choose how to organize one’s time. Lockdown measures can lead to multiple changes, some of which can possibly decrease, while others can increase the susceptibility to a migraine attack. Lockdown may, for instance, increase feelings of stress, anxiety, and insecurity about health, (un)employment or the financial situation of patients. In the long term, these factors may worsen migraine.
Similarly to the mentioned study, an additional large cohort of users of a German headache app reported reduced stress levels during the first month of the COVID-19-related lockdown (99). Headache frequency and intensity remained unchanged, but the authors describe a reduction of acute headache medication days.
A small selective retrospective study (100) and a larger study (101) reported improvement of headache and decreased medication use compared to pre-lockdown, especially for those with low depressive symptoms scores. As observed by an Italian study, primary headache disorders generally improved during lockdown also in pediatric patients, whose lifestyle modifications, particularly reduction in school-related stress, represented the main factor impacting the course of their headache (102).
However, not all patients improve and other studies have reported no difference (103), or even worsening of the usual headache and an increase in medication intake, often related to sleep disturbances, anxiety and depression (104–106).
E-health and telemedicine
During the pandemic several changes had to be implemented for headache care. This offered an opportunity to utilize telemedicine solutions, including headache E-diaries, as a monitoring tool on a greater scale. A large US study analyzed self-reported migraine data of >1,500,000 patients and most of them were positively predisposed to use such an app in the future when combined with video consultations (107). Similar results were found in a survey conducted by the American Migraine Foundation. In a study of 1000 migraine patients, more than half reported some form of telemedicine by their treating physicians. The majority of patients (83%) rated their experience with telemedicine as (very) good, and almost all preferred to continue, at least partially, use of telemedicine for headache care (108). Willingness to use digital solutions among patients is high and prospective solutions are warranted to improve digital headache care. The use of E-diaries opens the opportunity for careful monitoring and improving insights in headache frequency and medication use, as observed in a study conducted in the Netherlands (109).
Conclusions
Headache in the setting of COVID-19 pandemic has emerged as a main health issue for the population, increasing the burden of headache disorders on a global scale. The reason is twofold: SARS-CoV-2 infection and/or SARS-CoV-2 vaccinations commonly induce headache as a secondary headache disorder and/or negatively impact primary headache disorders, already highly prevalent and disabling.
However, the pandemic has also disclosed some positive aspects: the management of primary headache disorders may benefit from certain lifestyle changes, as experimented during lockdown, and from the implementation of new healthcare strategies that include telemedicine and the use of a headache E-diary.
Despite the relevant impact of headache during the COVID-19 pandemic, our understanding of the role of SARS-CoV-2 and, in general, of viral infections and vaccinations in headache is still limited and the possibility of offering an optimal care to people with primary or secondary headache disorders in this setting, too. New research is therefore necessary as not only we are facing the emergence of new SARS-CoV-2 variants but also, we might need to deal with completely new viruses in the future.
Public health relevance
Headache is a common and difficult-to-treat symptom of both the acute and post-acute phase of SARS-CoV-2 infection. Different pathophysiological mechanisms may be involved, the trigeminovascular system being their plausible target, however specific evidence-based preventive treatment options are lacking. Headache attributed to SARS-CoV-2 vaccinations is also common, mainly resembles tension-type headache but its pathophysiology is still unclear. People with primary headache disorders more commonly experience headache in the acute phase of COVID-19 and after vaccination than the general population. Pandemic measures seemed to have had an initial positive impact on migraine patients and changes in headache care (telemedicine), forced by lockdown, have been welcomed.
Footnotes
Acknowledgements
We acknowledge all researchers and healthcare professionals whose efforts and work have been dedicated in fighting COVID-19. We also remember and honor all those people who suffered COVID-19 and its consequences.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EC has received honoraria as speaker from Novartis, Chiesi, Lundbeck, Medscape. He is a Junior Editor for Cephalalgia. He is a member of the Communication Committee of the European Academy of Neurology.
![]() . PP-R does not own stocks from any pharmaceutical company.
. PP-R does not own stocks from any pharmaceutical company.
Funding statement
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Tsubasa Takizawa has received funding from Keio University Global Research Institute (KGRI) Start-up grant. No funding was received for this study.