
Abstract
Background
Headache is a frequent symptoms of coronavirus disease 2019 (COVID-19). Its long-term evolution remains unknown. We aim to evaluate the long-term duration of headache in patients that presented headache during the acute phase of COVID-19.
Methods
This is a post-hoc multicenter ambisective study including patients from six different third-level hospitals between 1 March and 27 April 2020. Patients completed 9 months of neurological follow-up.
Results
We included 905 patients. Their median age was 51 (IQR 45–65), 66.5% were female, and 52.7% had a prior history of primary headache. The median duration of headache was 14 (6–39) days; however, the headache persisted after 3 months in 19.0% (95% CI: 16.5–21.8%) and after 9 months in 16.0% (95% confidence interval: 13.7–18.7%). Headache intensity during the acute phase was associated with a more prolonged duration of headache (Hazard ratio 0.655; 95% confidence interval: 0.582–0.737).
Conclusion
The median duration of headache was 2 weeks, but in approximately a fifth of patients it became persistent and followed a chronic daily pattern.
Introduction
Headache is one of the most frequent symptoms of coronavirus disease 2019 (COVID-19). Different studies have characterised the clinical phenotype and evolution (1–6), reporting that a group of patients have persistent headache (5).
To date, just a few studies have reported data about headache after the acute phase of COVID-19 (7–10), with inconsistent results, unreported prevalence of headache during the acute phase of the disease, underrepresentation of non-hospitalised patients and usually, cross-sectional evaluation at a pre-defined time (7–11). In all of these studies, headache was one of the many studied symptoms, with limited headache-specific information and no long-term follow-up.
To evaluate the long-term duration of headache, we combined data from six cohorts that studied patients with headache during the first wave of the pandemic.
Methods
The present study is a post-hoc secondary analysis of six studies with ambisective (retro and prospective) cohort design. The study was done according to the Strengthening the Reporting of Observational Studies in Epidemiology (12). The study population was composed of adult patients that had been included in studies that specifically analysed headache in COVID-19 in Spain, whose methods and main results have already been published (1–6). Briefly, all the studies systematically screened the presence of new-onset headache during the course of COVID-19. Four studies assessed only hospitalised patients or patients that visited the emergency department (1,4–6), one study assessed only patients managed in an outpatient setting (2) and one study assessed both inpatients and outpatients (3). All studies were approved by local Ethic review boards and patients provided informed consent, either written or verbal depending on the site. The screening of patients was conducted between 1 March and 27 April 2020 and for the present study, all the participant sites completed at least 9 months’ follow-up in those patients in whom headache persisted at the time of the original study completion. The follow-up protocol was based on the local standard of care, but all participants were contacted 9 months after the headache onset to evaluate headache persistence.
To evaluate the headache phenotype, a headache expert administered an in-person or telephonic questionnaire, also collecting demographic and clinical variables. We harmonised the databases and combined a series of demographic variables, including age at the moment of COVID-19 infection, sex, and prior history of any headache disorder. As clinical variables, we assessed the time elapsed between the first COVID-19 symptom and the onset of headache. We assessed whether the patient was managed in an outpatient setting or was hospitalised. The severity of COVID-19 was categorised into mild disease, pneumonia, severe pneumonia, acute respiratory distress syndrome (ARDS) and death. We also evaluated headache-related variables evaluated during the acute phase, including the localisation, quality, intensity of headache (measured in a 1–10 verbal analogue scale) and the presence of associated symptoms, such as photophobia/phonophobia, nausea or worsening by physical activity.
Statistical analysis
The primary aim was to describe the duration of headache over time, and the proportion of patients in which headache persisted at 1, 2, 3, 6 and/or 9 months. The duration of headache was defined as the number of days that headache persisted after initial onset without headache-free intervals. We explored which variables were associated with a more prolonged duration of headache. For this, we compared a series of demographic and clinical variables between hospitalised and non-hospitalised patients, and we compared the data in patients that were hospitalised and those managed in an outpatient setting.
We present qualitative (sex, prior history of headache, presence of pneumonia, need of hospitalisation, quality of the headache, presence of photophobia, phonophobia, nausea or worsening by physical activity) and ordinal (COVID-19 severity) variables as frequency or proportion, indicating the differing denominators for the presence of missing data (i.e. patients that had died), and percentage. Continuous quantitative variables (age, days since onset of symptoms and headache, duration of headache, intensity of headache) are described as mean or median, depending on the normality of the distribution and standard deviation (SD) or inter-quartile range (IQR) respectively. Qualitative variables were evaluated by Fisher’s exact test. Quantitative variables were assessed by Student’s t-test or the Mann–Whitney U test. All hypothesis testing was two-tailed and the statistical signification threshold was set at 0.05. We used Kaplan–Meier survival curves to represent the duration of headache over time (Supplemental Figure 1). For the exploratory analysis of which variables were associated with a more prolonged duration, Cox regression was done, headache duration being the dependent variable. Those variables with a p-value <0.2 in the univariate analysis were included in a multivariable analysis. We present Hazard ratio (HR) and 95% confidence intervals (CI). Missing data were managed with complete case analysis. The statistical analysis was carried out with SPSS (version 26.0) for Mac (IBM Corp. Armonk, NY).
Results
We included data from five prior studies that systematically evaluated the presence of headache, being described in 821 out of 3698 patients (22.2%; 95% CI: 20.9–23.6%) and an additional sixth study that did not report the total number of screened patients and added 112 additional headache patients. Long-term follow-up data was available in 905/933 (97.0%) headache patients. Patients had been hospitalised in 457/905 (50.5%) cases and managed in outpatient setting in 448/905 (49.5%) cases. Hospitalised patients were older, more frequently male, had radiological diagnosis of pneumonia more frequently and a more severe disease. Table 1 and Supplementary Table 1 summarise the main demographic and clinical variables.
Demographic and clinical differences between patients with and without persistent headache after 9 months.

The differing denominators used indicate missing data. In bold, statistically significant differences.
IQR: Inter-quartile range.
Phenotype at baseline and prospective duration of headache
The most frequent headache phenotype was holocranial (67.8%), with pressing quality (57.3%), and severe intensity (50.6%). Table 1 summarises the phenotype and associated symptoms.
The precise headache duration was available in 874/905 (96.6%) cases and length of 14 (6–39) days median. The proportion of patients in which headache persisted after the first month was 272/874 (31.1%; 95% CI: 28.1–34.3%) patients, 188/874 (21.5%; 95% CI: 18.9–24.4%) after the second month, 166/874 (19.0%; 95% CI: 16.5–21.8%) after the third month, 147/874 (16.8%; 95% CI: 14.4–19.5%) after 6 months and 140/874 (16.0%; 95% CI: 13.7–18.7%) after 9 months. Figure 1 represents the survival curve of the headache duration in the entire study sample. We did not observe differences between patients with and without prior history of headache (Supplementary Table 2).
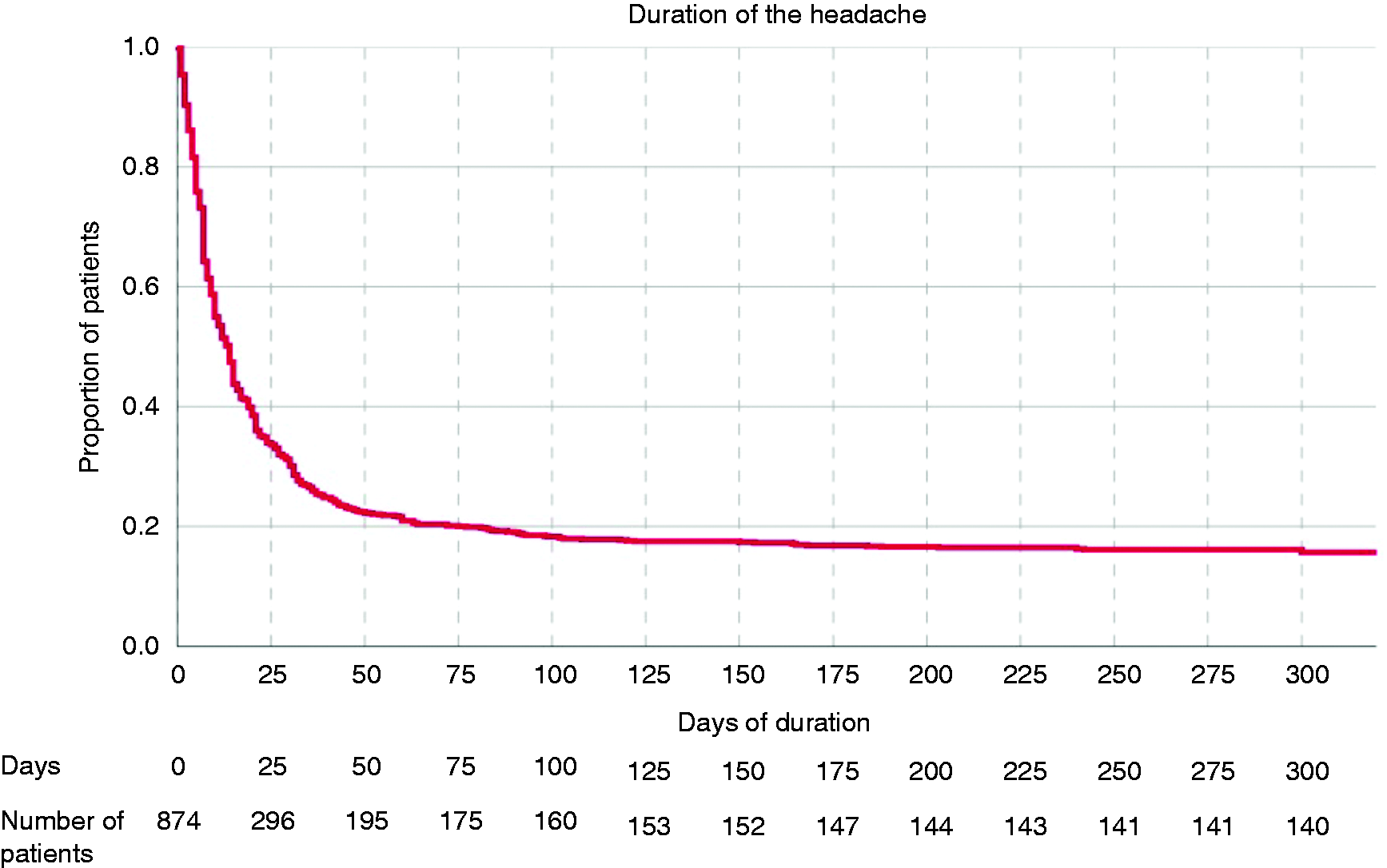
Survival curve of the headache duration in the entire study sample.
Patients with persistent headache after 9 months were older, more frequently female, had less frequency of pneumonia, milder intensity of the headache, and had higher frequency of throbbing quality of pain, photophobia or phonophobia and worsening by physical activity, but lower frequency of pressing headache (Table 1).
Predictors of headache duration
In the univariate analysis, age, female sex, intensity of the headache, pressing quality, throbbing quality, presence of photo/phonophobia and worsening with physical activity were associated with a more prolonged duration of headache over time. In the multivariate analysis, only headache intensity during the acute phase of the headache remained statistically significant (HR 0.655; 95% CI: 0.582–0.737, p < 0.001) (Table 2).
Cox-regression analysis of factors associated with persistent headache.

In bold, statistically significant differences. CI: Confidence interval.
Discussion
In the present study, we combined data from six of the largest headache-specific series that have been published (1–6). Headache is an early symptom of COVID-19, which in most cases lasts around 2 weeks but becomes persistent in 17% of patients, adopting a chronic pattern. We observed that in those cases in which headache persists after 2 months, it was quite likely to remain present over time for the follow-up period.
The survival curve flattened after 60 days; however, when headache persisted at month 1, there was about a 50% chance of it remaining at month 9, which emphasises the importance of the prompt evaluation of patients with persistent headache after COVID-19. To date, there are no specific therapies, and most clinicians treat post-COVID-19 headache based on the similarity of the clinical phenotype with other primary headache disorders (13). Considering the impact of headache, we need controlled studies of potential treatments.
Patients with persistent headache at 9 months had phenotypic features that resemble migraine more frequently than those without persistent headache, but the proportion of patients with tension-type-like headache and migraine-like headache was similar, as it has been described in series of New Daily Persistent Headache (14). The percentage of patients with persistent headache is also similar to the estimated prevalence of headache in the general population (15), which could suggest that COVID-19 infection could trigger a personal migrainous biology (13,16), or the onset of an NDPH (17).
Our study has important limitations. First, due the shortage of reagents during the first wave, not all the patients underwent a PCR or serum antibody test. Second, we did not account for the presence of other post-COVID-19 symptoms, and the role of other parameters related to the COVID-19 infection was not explored. We did not control for the presence of prophylactic medications, so the percentages described in our study could be underestimated. The non-use of headache diaries prevented us from properly assessing whether the improvement was progressive from a chronic, high-frequency episodic headache to a low-frequency episodic headache, and how the headache intensity and acute treatment response changed over time. The specific type of prior headache history was not analysed, and future studies should specifically assess it and evaluate the possibility of non-formally diagnosed primary headache disorders as well. The generalisability of the study is limited to adult population, from Spain, and mostly of Caucasian origin.
Conclusion
Headache is an early symptom in COVID-19 with a median duration of 2 weeks. In around a fifth of patients, it becomes persistent and follows a chronic pattern. The presence of phenotypic features of migraine at baseline were more frequent in patients with persistent headache after 9 months.
Clinical implications
In approximately a fifth of patients who present headache during the acute phase of COVID-19, it becomes persistent and adopts a chronic pattern. Nine months after the headache onset during COVID-19, 16% of patients still suffer from headache. Patients with migraine features at baseline more frequently had persistent headache after 9 months.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024211068074 - Supplemental material for Post-COVID-19 persistent headache: A multicentric 9-months follow-up study of 905 patients
Supplemental material, sj-pdf-1-cep-10.1177_03331024211068074 for Post-COVID-19 persistent headache: A multicentric 9-months follow-up study of 905 patients by David Garcia-Azorin, Almudena Layos-Romero, Jesús Porta-Etessam, Javier A Membrilla, Edoardo Caronna, Alicia Gonzalez-Martinez, Álvaro Sierra Mencia, Tomás Segura, Nuria Gonzalez-García, Javier Díaz-de-Terán, Victor J Gallardo, Ana Beatriz Gago-Veiga, Alejandro Ballvé, Javier Trigo López, María Sastre-Real, Arnau Llauradó, Ana Cornejo, Íñigo de Lorenzo, Ángel Guerrero-Peral and Patricia Pozo-Rosich in Cephalalgia
Supplemental Material
sj-pdf-2-cep-10.1177_03331024211068074 - Supplemental material for Post-COVID-19 persistent headache: A multicentric 9-months follow-up study of 905 patients
Supplemental material, sj-pdf-2-cep-10.1177_03331024211068074 for Post-COVID-19 persistent headache: A multicentric 9-months follow-up study of 905 patients by David Garcia-Azorin, Almudena Layos-Romero, Jesús Porta-Etessam, Javier A Membrilla, Edoardo Caronna, Alicia Gonzalez-Martinez, Álvaro Sierra Mencia, Tomás Segura, Nuria Gonzalez-García, Javier Díaz-de-Terán, Victor J Gallardo, Ana Beatriz Gago-Veiga, Alejandro Ballvé, Javier Trigo López, María Sastre-Real, Arnau Llauradó, Ana Cornejo, Íñigo de Lorenzo, Ángel Guerrero-Peral and Patricia Pozo-Rosich in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DGA received a research grant from the Regional Health Administration and an educational grant from the International Headache Society, and honoraria from the World Health Organization. PP-R has received honoraria as a consultant and speaker during the last 5 years from Allergan/AbbVie, Almirall, Biohaven, Chiesi, Corpus, Eli Lilly, Medscape, Neurodiem, Novartis and Teva. Her research group has received research grants from Novartis and Teva Pharmaceuticals and has received funding for clinical trials from Alder, electroCore, Eli Lilly, Lundbeck, Teva Pharmaceuticals, and Amgen/Novartis. She is a member of the Board of Trustees of the International Headache Society and a member of the Council of the European Headache Federation. She is on the editorial board of Revista de Neurologia. She is an associate editor for Cephalalgia, Headache, Neurologia, Frontiers of Neurology and The Journal of Headache and Pain. She is a member of the Clinical Trials Guidelines Committee of the International Headache Society. She has edited the Guidelines for the Diagnosis and Treatment of Headache of the Spanish Neurological Society. She does not own stocks from any pharmaceutical company. The rest of the authors declares no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data from one of the cohorts was funded by the regional health administration (Gerencia Regional de Salud (GRS) Castilla y Leon, grant number 2289/A/2020).
Data access,responsibility,and analysis
DGA had full access to all the data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
Data sharing statement
Datasheets are available for other researchers upon reasonable request to the corresponding author.
Information about prior presentation of the data
Part of the data of the present manuscript has been submitted as an abstract to the International Headache Congress (2021).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.