
Abstract
Background
Contrary to pre-attack symptoms before an individual cluster headache attack, little is known about the pre-cluster symptoms before the onset of cluster bouts. We previously described pre-attack symptoms before cluster headache attacks. The aim of this study was to investigate characteristics of pre-cluster symptoms in patients with episodic cluster headache.
Methods
In this multicentre study, 184 patients with episodic cluster headache were recruited between October 2018 and December 2020. They were interviewed by investigators and completed a structured questionnaire. To investigate pre-cluster and pre-attack symptoms, we assessed 20 symptoms and signs using the questionnaire.
Results
The upcoming cluster bout was predictable in 35.3% (n = 65/184) of the patients. When present, pre-cluster symptoms occurred at a median duration of 7 days (interquartile range, 2.3–14 days) before the onset of the cluster bout. Patients with pre-cluster symptoms showed a higher proportion of women, prevalence of pre-attack symptoms and seasonal rhythmicity, frequency of cluster headache attacks per day, and total number of cluster bouts compared to patients without pre-cluster symptoms. In univariable and multivariable logistic regression analyses, female sex was associated with the predictability of pre-cluster symptoms (odds ratio = 2.297, p = 0.016).
Conclusions
The upcoming cluster bout was predicted in approximately 35% of patients with episodic cluster headache, which may allow for an earlier preventive treatment and help understand the pathophysiology.
Introduction
Cluster headache (CH) is a disabling primary headache disorder characterised by recurrent unilateral severe headache accompanied by ipsilateral autonomic features (1,2). The term “cluster headache” is derived from the tendency of the attacks to cluster together into bouts that may last several weeks to months (3). During cluster bouts, pre-attack symptoms have been increasingly recognised before the onset of an individual headache attack (4,5). In addition to pre-attack symptoms, some patients with CH reported pre-cluster symptoms occurring days or weeks before the onset of a cluster bout. In two previous studies from England and Italy, 8% and 40% of patients, respectively, reported pre-cluster symptoms (6,7). In a recent Danish study, 86% of patients had experienced pre-cluster symptoms and based on the experience of pre-cluster symptoms, 57% of patients answered that they had predicted upcoming cluster bouts (8). However, compared to studies on pre-attack symptoms, those on pre-cluster symptoms are few and have involved only a small number of patients.
Together with pre-attack symptoms, pre-cluster symptoms could contribute to the understanding of the underlying pathophysiology of CH. Furthermore, recognition of these pre-cluster symptoms could allow early initiation of preventive treatment, potentially preventing the onset of a cluster bout.
Therefore, the aim of this study was to describe the predictability, characteristics, and latency of pre-cluster symptoms in episodic CH.
Methods
Patients and study setting
We screened patients with CH who had visited 12 hospitals in Korea from October 2018 to December 2020. Inclusion criteria were: a) an active cluster bout; b) more than one cluster bout in a lifetime; and c) completion of medical interviews and questionnaires. The diagnosis of CH was based on the criteria of the International Classification of Headache Disorders 3rd edition (ICHD-3) (1). We included patients with episodic CH. Patients with probable CH and chronic CH were excluded.
This multicentre, cross-sectional, and observational study used data from the Korean Cluster Headache Registry (KCHR) version 2. The protocol for the evaluation of CH using KCHR version 2 has been described previously (4). To summarise, patients who visited the participating hospitals were examined and interviewed by a headache specialist to confirm the diagnosis of CH. Subsequently, patients who had consented to enrolment in the registry completed a structured questionnaire on clinical characteristics before CH attacks and bouts. The institutional review board of each participating hospital approved this study. Written informed consent was obtained from all patients.
Clinical evaluation
We collected demographic data and clinical information including CH characteristics of attack during a current bout (attack frequency, severity and duration), diurnal and seasonal rhythmicity, the total number of cluster bouts, presence of comorbid migraine, smoking status and alcohol intake to compare patients with pre-cluster symptoms and those without pre-cluster symptoms. Investigators determined seasonal rhythmicity by asking patients if their cluster bouts tended to occur in the same month of each year. Diurnal rhythmicity was determined if CH attacks in the current bout tended to occur at the same time of each day.
We collected clinical characteristics of pre-cluster and pre-attack symptoms during the current bout. In this study, pre-cluster symptoms were defined as the presence of CH-related symptoms occurring days before the onset of the cluster bout, and pre-attack symptoms were defined as symptoms preceding and forewarning of a patient’s usual severe CH attacks by minutes or hours based on previous studies (4–8).
In the questionnaire, we asked patients the following questions in order: a) Were you able to predict an upcoming cluster bout? b) If yes, which symptoms helped predict an upcoming cluster bout? c) How many days after a prediction did a cluster bout occur? d) What was the basis to judge that symptoms were predictive of an upcoming cluster bout?
To investigate pre-cluster and pre-attack symptoms, we assessed 20 relevant symptoms and signs using a questionnaire. All pre-cluster and pre-attack symptoms were included in the questionnaire and grouped into four subtypes as follows: a) local and painful symptoms (pain in the same or another area of the CH attack and neck pain); b) local and painless sensory symptoms (sensory change in the same or another area of the CH attack); c) autonomic symptoms (conjunctival injection or lacrimation, rhinorrhea or nasal congestion, forehead and facial sweating, ptosis or miosis, and eyelid edema); and d) general symptoms (agitation, fatigue, concentration difficulty, yawning, mood changes, appetite changes, frequent urination, nausea, photophobia or phonophobia or osmophobia, and dizziness) (Table 1). Twenty symptoms and signs were selected based on previous studies (6,7) and those validated by the KCHR study group. In addition, patients could describe symptoms that were not included in the questionnaire in their own words.
Simplified 20 questionnaire items of pre-cluster and pre-attack symptoms.

Patients who reported more than one subtype of pre-cluster or pre-attack symptoms were defined as having multiple pre-cluster or pre-attack symptoms, respectively.
Statistical analyses
Data are presented as number (percentage) or median (interquartile ranges [IQR]). The Kolmogorov–Smirnov test was used to test for the normal distribution of variables. The chi-square or Fisher’s exact and Mann–Whitney U tests were used to compare categorical and continuous variables, respectively. Bonferroni’s correction was applied for multiple comparisons. Logistic regression analyses were performed to assess factors associated with the presence of pre-cluster symptoms. Variables with a univariable p-value of <0.20 were included in the multivariable logistic regression analysis, with covariates including the age, sex, disease duration, smoking status, alcohol intake, total number of bouts, diurnal and seasonal rhythmicity, presence of comorbid migraine, presence of pre-attack symptoms, and CH attack severity, duration, and frequency of the current bout. In patients with pre-cluster and pre-attack symptoms, a two-tailed paired test (i.e., Wilcoxon signed-rank test) was performed for intra-patient comparisons between pre-cluster and pre-attack symptoms in each subtype, such as local and painful, local and painless sensory, autonomic, and general symptoms. Statistical analyses were conducted using IBM SPSS (version 22.0; IBM Corporation, Armonk, NY, USA). A two-tailed p-value of <0.05 was considered to be statistically significant.
Results
Patients
We screened 243 patients with CH during the study period. After excluding 29 patients with the first episode of CH, 21 patients with probable CH, six patients with chronic CH and three patients who had not completed the structured questionnaire, a total of 184 patients with episodic CH were finally included in this study.
Table 2 shows demographics and characteristics of the included patients. The median age of patients was 35.5 (IQR, 29.0–41.0) years, with a male predominance (n = 126, 68.5%). Approximately 63% and 59% of patients had diurnal and seasonal rhythmicity, respectively. The median disease duration was 7.1 (IQR, 3.0–11.4) years. The median total number of bouts was seven (IQR, 4.0–11.0), and 112 of 184 (60.9%) patients experienced more than five cluster bouts.
Demographics and characteristics of patients with episodic cluster headache according to an ability to predict an upcoming cluster bout.

Data are presented as median (IQR) or number (percent).
*Comparison between patients with and without pre-cluster symptoms.
NRS: numeric rating scale.
When patients with and without pre-cluster symptoms were compared, patients with pre-cluster symptoms showed a higher proportion of women (43.1% vs. 25.2%, p = 0.013), a higher frequency of CH attacks per day (1.5 vs. 1.0, p = 0.049), and a higher total number of cluster bouts (8.0 vs. 6.0, p = 0.003) compared to those without pre-cluster symptoms. In addition, a higher prevalence of pre-attack symptoms (89.2% vs. 70.8%, p = 0.011) and seasonal rhythmicity (70.8% vs. 52.1%, p = 0.019) were observed in patients with pre-cluster symptoms than in those without pre-cluster symptoms. No significant differences were observed in the age, smoking status, alcohol intake, disease duration, diurnal rhythmicity, or CH attack duration or severity during the bout between the two groups.
Predictability of an upcoming cluster bout and characteristics of pre-cluster symptoms
Table 3 shows the distribution of pre-cluster symptoms in patients. A total of 65 (35.3%) patients reported that they were able to predict an upcoming cluster bout by pre-cluster symptoms. The median time interval from the pre-cluster symptom to the initiation of a cluster bout was 7 days (IQR, 2.3–14 days; range, 1–30 days). The most frequent pre-cluster symptom was pain in the same area as the CH attack (15.8%), followed by neck pain (9.8%), fatigue (8.7%), and mood changes (7.1%). Based on the stratification into four subtypes, the prevalence of local and painful, local and painless sensory, autonomic, and general symptoms was 24.5%, 6.0%, 3.3%, and 16.8%, respectively. Patients recognised these symptoms as pre-cluster symptoms for the following reasons: a) Symptoms were similar to their usual CH attack symptoms (47.7%, n = 31/65), b) patients experienced symptoms at those times of the year when cluster bouts usually occurred (26.2%, n = 17/65), c) these symptoms occurred with previous CH precipitating factors, such as excessive physical stress (18.5%, n = 12/65), excessive emotional stress (13.8%, n = 9/65), or alcohol-induced headache (10.8%, n = 7/65). The mean number of pre-cluster symptoms per patient was 2.7 ± 3.2 (range, 1–16). Forty (21.7%) patients reported a single pre-cluster symptom, and 25 (13.5%) patients reported multiple pre-cluster symptoms (Table 4). Among the single pre-cluster symptoms, local and painful symptoms were the most frequent (14.1%), and no patients reported any autonomic symptoms as a single symptom. Among multiple pre-cluster symptoms, local and painful symptoms plus general symptoms were the most frequent (7.1%).
Characteristics of pre-cluster symptoms of patients.
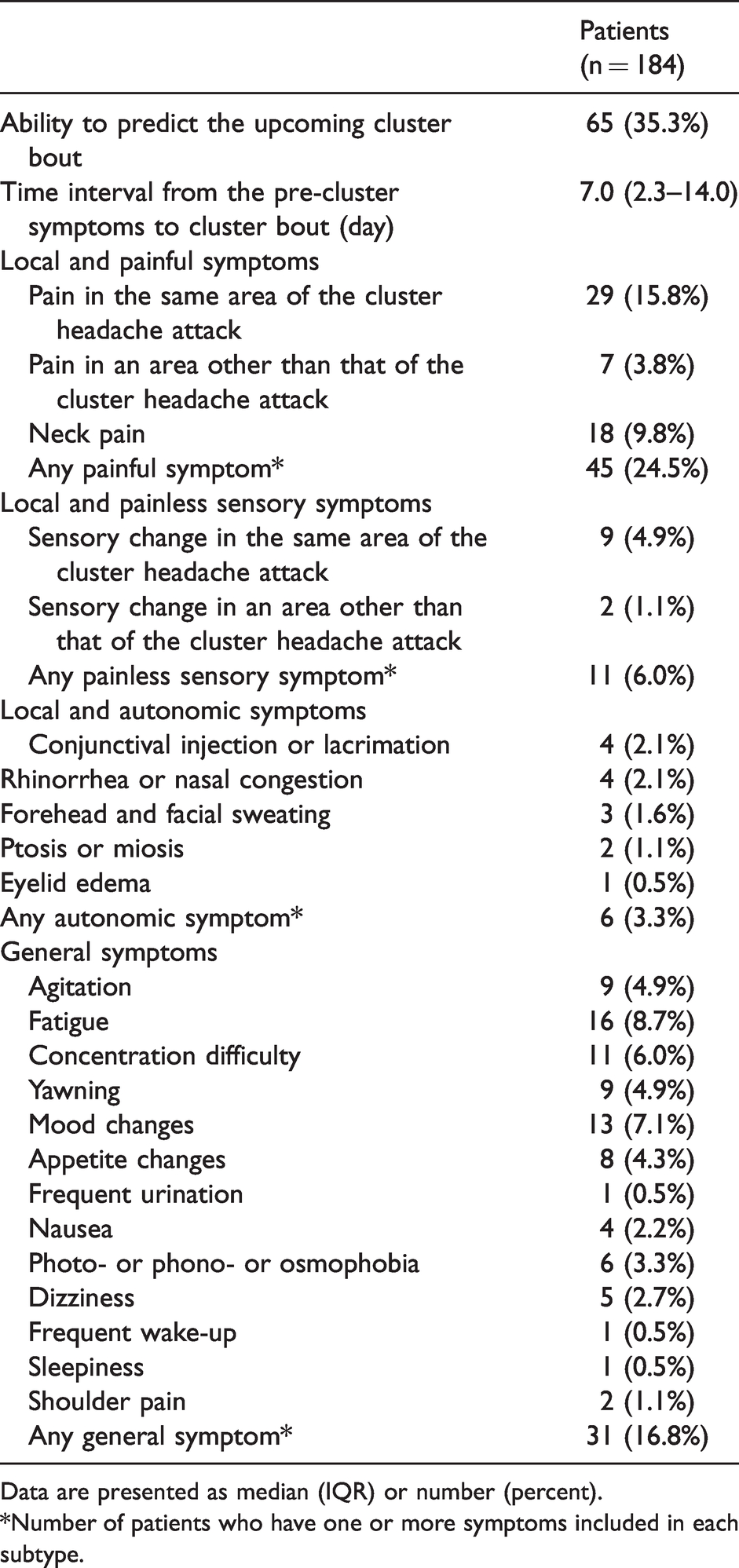
Data are presented as median (IQR) or number (percent).
*Number of patients who have one or more symptoms included in each subtype.
Prevalence of pre-cluster symptoms according to types.

Association between pre-cluster and pre-attack symptoms
Higher prevalence of pre-attack symptoms and more general symptoms were observed in patients with pre-cluster symptoms than in those without pre-cluster symptoms (73.1% vs. 89.2%, p = 0.011; 27.6% vs. 51.6%, p = 0.001, respectively; Table 5). The median interval from pre-attack symptoms to the attack did not differ between the groups. In patients with both pre-cluster and pre-attack symptoms, the subtypes of symptoms were similar in individual patients. The Wilcoxon signed-rank test showed no significant differences between pre-cluster and pre-attack symptoms in any subtype (p = 0.248 for local and painful symptoms, p = 0.480 for local and sensory symptoms, p = 0.206 for autonomic symptoms, and p = 0.405 for general symptoms).
Characteristics of pre-attack symptoms according to an ability to predict an upcoming cluster bout

Factors associated with the predictability of an upcoming cluster bout
In the univariable logistic analysis, female sex (odds ratio [OR], 2.245; 95% confidence interval [CI], 1.181–4.266; p = 0.014), seasonal rhythmicity (OR, 2.148; 95% CI, 1.126–4.098; p = 0.020), and presence of pre-attack symptoms (OR, 3.048; 95% CI, 1.261–7.368; p = 0.013) were associated with the predictability of an upcoming cluster bout. In the multivariable logistic regression analysis, only female sex (OR, 2.297; 95% CI, 1.166–4.527; p = 0.016) was associated with the predictability of an upcoming cluster bout (Table 6).
Univariable and multivariable logistic regression analyses to assess associated factors with the predictability of pre-cluster symptoms.

*Variables (p < 0.2 in univariable analysis) were included.
CI: confidence interval; OR: odds ratio.
Discussion
To the best of our knowledge, this cross-sectional observational study is the first in Asia to investigate the predictability of an upcoming cluster bout and the characteristics of pre-cluster symptoms. Our main findings were as follows: a) Cluster bouts were predicted in approximately 35% of patients with episodic CH; b) pre-cluster symptoms of pain were the most frequent, followed by general symptoms, which showed a similar pattern as pre-attack symptoms; and c) female sex was independently associated with the predictability of an upcoming cluster bout.
Predictability and prevalence of pre-cluster symptoms
In our study, 35.3% of patients with CH reported that they could predict their upcoming cluster bouts. To the best of our knowledge, only three studies have evaluated the predictability of upcoming cluster bouts (8) and/or prevalence of pre-cluster symptoms (6–8). In a recent Danish study, Pedersen et al. reported that 57% (n = 53/93) of patients with a CH history of more than one bout answered that they could predict an upcoming bout with a mean duration of 4.6 (IQR, 2–7) days (8). The difference from our study in terms of predictability may be attributed to methodological, demographic, and ethnic differences. It was reported that 91% and 60% of patients had experienced more than five bouts in groups of patients with and without the ability to predict an upcoming cluster bout, respectively (8). Similar to the Danish study, the total number of bouts in our study was statistically higher among patients who were able to predict pre-cluster symptoms. The smaller percentage of patients with more than five CHs in our study (60%), compared to the 75% in the Danish study, may have contributed to the lower predictability compared to the Danish study. However, contrary to the Danish study population, our patients had active cluster bouts, which could be an advantage of this study owing to the minimised recall bias. The higher predictability in patients who have experienced more cluster bouts could be because patients who have experienced more bouts are more likely to identify symptoms as pre-cluster symptoms, where they would otherwise chalk it up to random symptoms. A recent study has shown that Asian and European/North American countries have regional differences in the presentation of CH (9). Compared to patients with CH in European and North American countries, those in Asian countries have a stronger male predominance and lower headache burden, such as a lower attack frequency per day, bout frequency and bout duration (9). Patients in this study had a lower attack frequency per day than those in the Danish study (1.0 [IQR, 1–2] vs. 2.7 [IQR, 2–4]) (8).
In previous studies, the prevalence of pre-cluster symptoms was 8–86% of the Western CH population (6–8). From England, Blau et al. reported that 12 of 150 (8%) patients experienced pre-cluster symptoms (6). From Italy, Torelli et al. reported that 17 of 42 (41%) patients experienced pre-cluster symptoms (7). It was reported that 86 of 100 (86%) patients experienced pre-cluster symptoms, showing the highest prevalence among all studies (8). Demographic and methodological differences may have influenced the prevalence of pre-cluster symptoms among these studies. In an English study (6), the lowest prevalence among studies included 17% of patients with chronic CH, while Italian and Danish studies (7,8) and our study included only episodic CH. In addition, all studies used different questionnaires. The English study used only open-ended questionnaires; the Italian study used only a self-reported 65-item questionnaire; and Danish studies collected data through a semi-structured interview with a predetermined 25-question list and open questions. More questionnaire items might have made it easier for patients to recall pre-cluster symptoms. However, patients are more likely to choose symptoms irrelevant to CH if many questionnaire items are provided.
In our study, female sex was independently associated with better predictability of an upcoming cluster bout (OR, 20.026; p = 0.039). CH was initially considered to be a male disorder, but recent studies have shown a trend toward a decreasing male predominance (10–12). Although many previous studies have analysed the clinical characteristics of CH between sexes, CH features showed no significant differences (13,14). Our finding, female sex as an independent factor of better predictability, might be a characteristic of female CH. However, in our study, a much smaller sample size of women than that of men might have exaggerated the statistical association. Future studies with a larger sample size are necessary to validate our results.
Characteristics of pre-cluster symptoms
The presence of pre-cluster symptoms may suggest that the cluster bout is not limited to the period in which recurrent typical CH attacks occur. Based on previous studies and our study, pre-cluster symptoms were reported as various symptoms occurring days before the onset of the cluster bout. In this study, patients reported that pre-cluster symptoms started a median duration of 7 days before the onset of the cluster bout. In an English study, patients had pre-cluster symptoms at an interval of 1 day to 8 weeks (6). In an Italian and a Danish study, pre-cluster symptoms with an average latency of 23.5 and 4.6 days before onset of cluster bout occurred, respectively (7,8). Patients were able to predict an upcoming cluster bout because characteristics of pre-cluster symptoms were similar to their usual cluster attacks. Interestingly, some patients were able to recognise an upcoming cluster bout by the occurrence of mild cluster-like headache after drinking alcohol several days before a cluster bout. Alcohol is a well-known trigger of CH attacks during CH bouts (2), and occurrence of mild cluster-like attacks induced by alcohol intake in the pre-cluster period might indicate that a change of threshold is taking place.
Characteristics of pre-cluster symptoms in our study were similar to those in previous Western studies (7,8). In our study, local and painful symptoms were the most prevalent pre-cluster symptoms. Of 65 patients with pre-cluster symptoms, 29 (45%) reported pain on the ipsilateral side of the CH attack, and 18 (28%) reported neck pain. These pain symptoms may tend to be milder than those of usual CH attacks and increase gradually before the onset of the cluster bout. Previous studies also reported that painful symptoms were very frequent (7,8). In a Danish study, dull and aching sensation (62%) and a shadow attack (60%) of pre-cluster symptoms were observed as the most frequent symptoms (8). Neck pain (41%) was the third most common symptom in that study. In an Italian study, most patients (26%) reported a shadow attack as a pre-cluster symptom (7). In addition to pre-cluster symptoms, pain symptoms, such as shadow attack and neck pain, are frequent pre-attack symptoms of CH (4,5). The perspective that they have similar characteristics may imply that a common structural link exists between pre-cluster or pre-attack symptoms and CH attacks. In this study, general symptoms were frequently observed, followed by painful symptoms. Among them, mood change, fatigue, and concentration difficulty were the most frequent symptoms, consistent with findings from the recent Danish study (8).
Pathophysiological implication
Pre-cluster symptoms were of different qualities, such as pain, sensory, autonomic, and general symptoms, possibly implying involvement of trigeminovascular pathway, trigeminal autonomic reflex and hypothalamus. These structures are involved in the pathogenesis of CH (15). The hypothalamus has been suggested to play a pivotal role in integrating pain, cranial autonomic features, and unique diurnal and circadian rhythmicity of CH (16). From this perspective, we speculate that the hypothalamus plays a prominent role in initiation of cluster bouts by affecting pre-cluster symptoms, although how it contributes to modulating susceptibility to initiation of cluster bouts from a pain-free state remains unclear. In recent studies, the hypothalamus has been suggested to play a central role in the pre-attack symptoms of CH (4,5). Our study showed a high prevalence of pre-attack symptoms in patients with pre-cluster symptoms. In addition, pre-cluster and pre-attack symptoms were similar in individual patients despite different pre-attack and pre-cluster symptom prevalence. Compared to our previous study on pre-attack symptoms in CH (4), some characteristics of pre-attack and pre-cluster symptoms were similar. For example, the most common pre-attack symptoms in order of frequency were local and painful symptoms and general symptoms, consistent with this study. These results suggest that pre-cluster and pre-attack symptoms belong to the same spectrum from the perspective of initiation of a CH attack. However, the longer interval between pre-cluster symptoms and initiation of CH may imply a more complex mechanism for initiation of CH than a direct facilitating or inhibiting effect on the hypothalamus depending on the individual’s susceptibility.
Treatment implication
Approximately 35% of patients with CH experienced pre-cluster symptoms, suggesting the significant potential of an early intervention. The early and timely preventive management of CH is necessary to shorten therapeutic latency during CH. However, the early treatment of CH is challenging because its efficacy has not been demonstrated. Based on the speculation that the hypothalamus plays a central role in pre-cluster symptoms, verapamil, which is widely accepted as the first-line preventive management in CH, can be used in the pre-cluster phase (17). Although the exact mode of action of verapamil in CH is unknown, its effect on activated calcium channels in the hypothalamus (18) modulates the activity of the central neurons and inhibits the presynaptic receptors on the hypothalamic noradrenergic neurons, thereby increasing norepinephrine levels in the hypothalamus (19). It may also be worthwhile to administer an anti-CGRP antibody, recently approved for preventing episodic CH, in the pre-cluster phase (20). Future studies are required to evaluate the efficacy of preventive drugs for CH when they are used for pre-cluster symptoms.
Strengths and limitations
To the best of our knowledge, this is the largest study to investigate pre-cluster symptoms in patients with CH. The strength of our study is that the diagnosis of CH and interviews were conducted by a headache specialist. Nevertheless, this study had several limitations. First, only Korean patients were included, which may compromise the generalisability of our study results. However, characteristics of pre-cluster symptoms were similar between our cohort and the others. In addition, it has an advantage in that it was the first study involving Asians. Second, because there was no standardised questionnaire, we used our own semi-structured questionnaire with fewer items compared to previous studies. Heterogeneous questionnaires can make it difficult to accurately compare the demographics and characteristics of pre-cluster symptoms among studies. Third, this study did not investigate the consistency of predictability. The presence of pre-cluster symptoms may be inconsistent across cluster bouts. Third, a recall bias may exist. We tried to minimise the recall bias by including patients in the active period of CH. However, future prospective longitudinal studies using a diary are warranted to validate our results. Fourth, because pre-cluster and cluster bouts may occur in succession, a grey zone may exist in which patients cannot accurately differentiate between cluster and pre-cluster bouts. To minimise this possibility, we recruited patients who had experienced more than one cluster bout, because they could recognise their usual cluster bouts. Lastly, since there has been no definition of the time interval from the onset of pre-attack symptoms to cluster attack and from pre-cluster symptoms to cluster bout, it was difficult to define time criteria in the methods. We expect that the results of this study will serve as a basis for determining the future definition.
Conclusion
The upcoming cluster bout was predicted in approximately 35% of Korean patients with episodic CH, in which characteristics were similar to those of previous studies. Further research of pre-cluster symptoms may allow for an earlier preventive treatment and help understand the pathophysiology.
Clinical implications
The upcoming cluster bout was predicted in 35.3% of episodic CH patients. Local and painful symptoms of pre-cluster symptoms were most frequent, followed by general symptoms, which showed a similar pattern similar as pre-attack symptoms. Female sex was independently associated with the predictability of an upcoming cluster bout.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.