
Abstract
Objective
To determine the natural course of cluster headache.
Methods
We screened patients with cluster headache who were diagnosed at Samsung Medical Center and lost to follow-up for ≥5 years. Eligible patients were interviewed by phone about the longitudinal changes in headache characteristics and disease course. Remission was defined as symptom-free 1) for longer than twice the longest between-bout period and 2) for ≥5 years.
Results
Forty-two patients lost to follow-up for mean 7.5 (range, 5.0–15.7) years were included. The length of the last bout did not differ from the first one, while the last between-bout period was longer than the first one (p = 0.012). Characteristics of cluster headache decreased over time: Side-locked unilaterality (from 92.9% to 78.9%), seasonal and circadian rhythmicity (from 63.9% to 60.9% and from 62.2 to 40.5%, respectively), and autonomic symptoms (from 95.2% to 75.0%). Remission occurred in 14 (33.3%) patients at a mean age of 42.3 (range, 27–65) years, which was not different from the age of last bouts in active patients (p = 0.623). There was a trend for more seasonal and circadian predilection at baseline in the active group (p = 0.056 and 0.063, respectively) and fewer lifetime bouts and shorter disease duration in patients in remission (p = 0.063 and 0.090).
Conclusions
This study first shows the natural courses of cluster headache. Features of cluster headache become less prominent over time. Remission occurred regardless of age. Although no single predictor of remission was found, our data suggest that remission of cluster headache might not be a consequence of more advanced age, longer duration of disease, or accumulation of lifetime bouts.
Introduction
Cluster headache (CH) is a rare primary headache disorder that has an estimated prevalence of about 0.1% in the general population (1). CH is characterized by excruciating and strictly unilateral headaches that are accompanied by cranial autonomic symptoms (2). Autonomic symptoms, which are essential for the diagnosis of CH, have been reported in about 97% of patients with CH (3,4). Circadian and circannual rhythmicity is also characteristic of episodic and, reportedly, chronic CH (2,5). With a great amount of headache-related disability, patients with CH are at increased risk of suicidal ideation and attempts, and psychiatric comorbidities (6–8).
To date, a limited number of studies exist that reveal the natural course and prognosis of cluster headache. Although two studies have suggested that prolonged remission occurs in some patients (9,10), questions remain, such as when these disabling headaches end; whether CH attacks change in frequency, severity, and/or characteristics; and what predicts the end of disease. A methodological limitation of clinic-based follow-up studies is that patients visit clinics only when they have active attacks. Furthermore, the characteristics of attacks might be modified by treatments. Therefore, untreated patients who were lost to follow-up are ideal subjects for investigations of the natural changes of headache characteristics towards the end of the disease.
In this study, we aimed to identify the longitudinal changes in the headache characteristics of CH, the characteristics and predictors of remission, and the pattern of remission in CH patients who were lost to follow-up.
Methods
Patients
This study is part of a prospective observational study of a retrospective CH cohort (ClinicalTrials.gov Identifier: NCT02895256). We screened patients who were diagnosed with CH at the Samsung Medical Center between 1997 and 2010. Within this retrospective cohort, patients who 1) signed to the agreement on the collection and use of personal information and 2) who had not visited the outpatient clinic for at least five years were considered eligible for the study. Eligible patients were contacted by phone. After informed consent was obtained by phone interview, the patients were recruited for the study. After the interview, the patients who had preventive treatments since the last attack were excluded from the analysis. The Samsung Medical Center Institutional Review Board approved this study.
Evaluations
We designed a semi-structured questionnaire on the headache characteristics, autonomic symptoms, circadian and circannual predilection of the first and last bouts, and temporal changes during the disease course. In this study, the term ‘between-bout period’ referred to the time interval between bouts. Time after the last bout was not considered as a between-bout period. Total disease duration was defined as the time from the first bout to the last bout. The number of total lifetime bouts was determined. The mean number of bouts per year was calculated as the number of total lifetime bouts divided by the total disease duration. All the interviews were performed by two headache neurologists (MJL and HAC) using this questionnaire. To minimize the inaccuracy of recall, we compared patients’ responses regarding the earlier bouts to their medical records. When a disparity was noted, we informed patients and facilitated their recall based on the records.
Based on the interview, the current disease status of each patient was classified as active, in remission, or converted to chronic CH. Remission was operationally defined if the patients were 1) symptom-free for longer than twice the longest between-bout period and 2) symptom-free for the past five years. The remainder were classified as having an active disease. Conversion to chronic CH was determined by using the International Classification of Headache Disorders-3 beta (ICHD-3 beta) criteria of chronic CH (3.1.2) (4).
Statistical assessments
All the descriptive data are presented as number (percentage) or median (interquartile range), unless otherwise specified. For the group comparisons, categorical variables were analyzed with Chi-square tests or Fisher’s exact tests, while continuous variables were compared with Student’s t-tests or Mann-Whitney tests according to the normal distribution of the variable. The statistical analyses were performed with SPSS software, version 18.0 (IBM Corporation, Armonk, NY, USA). Two-tailed p values less than 0.05 were considered statistically significant.
Results
Patients
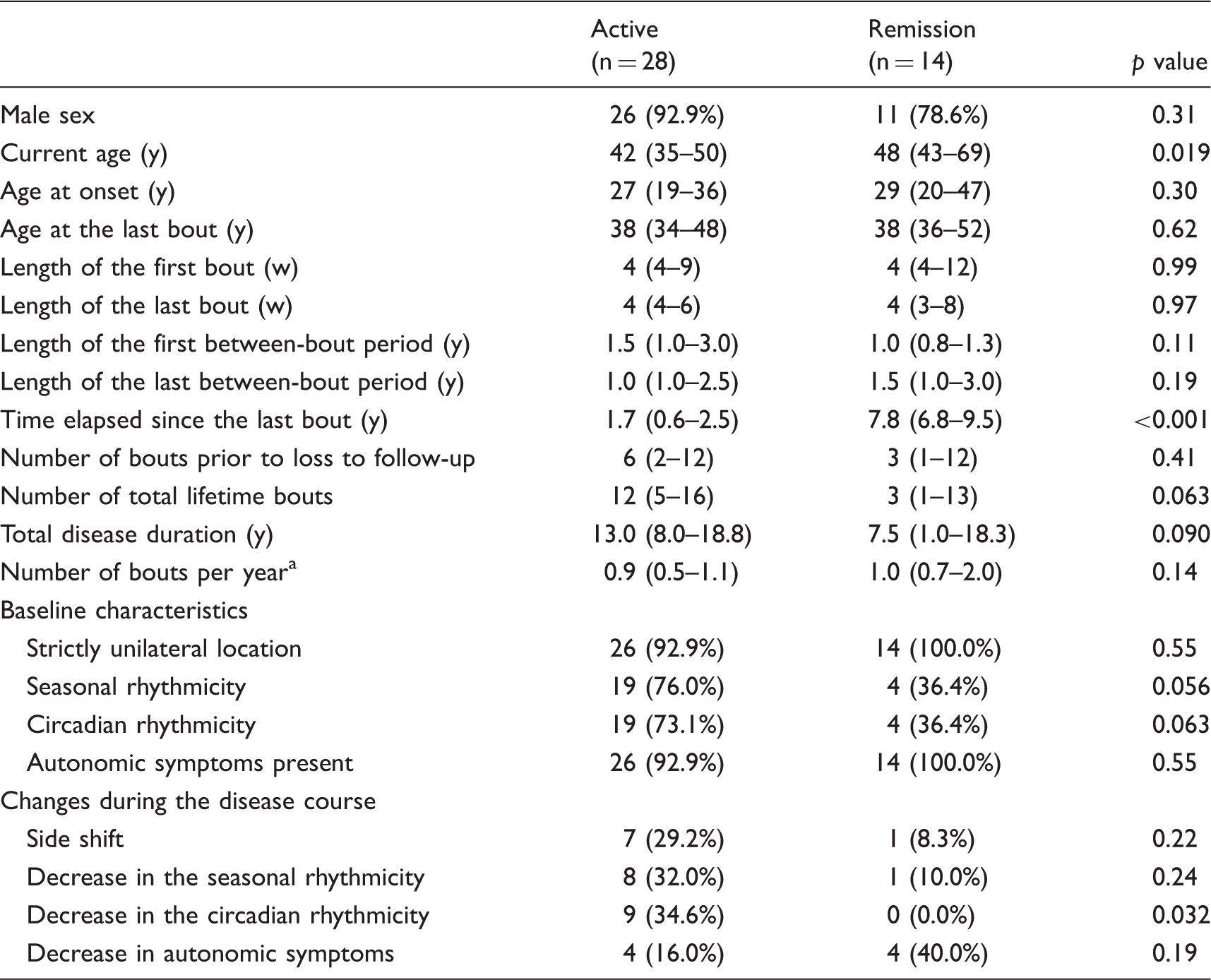
The study flow chart is shown in Figure 1. A total of 42 patients (current age, mean 45.8 years; range 29–82) were included in the final analysis. The mean time elapsed since the patients’ last visit was 7.5 years (range, 5.0–15.7). The demographics and characteristics are summarized in Table 1. Patients were mostly men (88.1%) and currently aged from 29 to 82 (mean 45.8) years. The mean age of onset was 30.0 (range, 10–73) years. All patients were currently out of bouts, reporting their last bouts at 0.1 to 11.6 (mean 4.1) years before the interview. The age at the last bout was widely distributed, from 24 to 65 years (mean 40.1). The number of total lifetime bouts was a mean of 11.0 (range, 1–42). The mean number of bout per year was 1.1 (range, 0.1–3.0) during the disease duration. Three patients had only a single bout.
Flow diagram of the study. Demographics and characteristics of the study subjects. y, years. Data are presented as number (percentage) or mean (range). Calculated as the number of total lifetime bout divided by the disease duration; bAssessed in 36 patients; cAssessed in 37 patients.

Changes in the characteristics of CH
Length of the bouts and between-bout periods
Temporal changes of headache were assessed in 39 patients with more than two lifetime bouts. The mean lengths of their first and last bouts were 6.4 (range, 1–28) and 7.2 (range, 1–56) weeks, respectively (p = 0.664 by paired t-test). In 35 patients who qualitatively assessed the temporal changes of their lifetime bouts, lengths of bouts were unchanged in 21 (60.0%), decreased in 8 (22.9%), and increased in 6 (17.1%). The length of between-bout period was mean 1.4 ± 1.23 years for the first between-bout period and 1.9 ± 1.33 years for the last one (p = 0.012 by paired t-test).
Side-locked unilaterality
At baseline, 39 (92.9%) patients reported a side-locked headache. A total of 38 patients provided answers about the temporal change of laterality, after excluding four patients (three with only a single bout and one who could not recall the temporal changes of laterality at the last bout) (Figure 2(a)). Among the 38 patients, 35 had side-locked headaches at baseline. Of the 35 patients, 29 (82.9%) had headaches on the original side during the entire disease course, while six (17.1%) reported side shifting, including bilateral attacks (n = 1), side-alternating attacks between bouts (n = 3), and side-alternating attacks within bouts (n = 2). In three patients with bilateral or alternating headaches at baseline, one reported that their headache became side-locked over the disease course. Finally, 30 (78.9%) reported strictly unilateral headaches without any side shifting.
Changes in characteristics of cluster headache. During the disease course, characteristics of cluster headache become less prominent in (a) side-locked unilaterality (from 92.8% to 78.9%), (b) seasonal rhythmicity (from 63.9% to 38.9%), (c) circadian rhythmicity (from 62.2% to 40.5%), and (d) autonomic symptoms (from 95.2% to 75.0%). Proportions were derived from responders only.
Seasonal rhythmicity
At baseline, six patients could not determine their seasonal rhythmicity because of the infrequency of their bouts and difficulty in recalling. Among the remaining 36 patients, 23 (63.9%) had a seasonal predilection of bouts. Among them, six (26.1%) lost their seasonal rhythmicity, three (13.0%) reported a shift in the season of predilection, and only 14 (60.9%) maintained the same seasonal predilection. All 13 (36.1%) who lacked a seasonal rhythmicity at baseline still had no seasonal predilection at follow-up. Finally, only 14 (38.9%) reported a constant pattern of seasonal recurrence during the disease course (Figure 2(b)).
Circadian rhythmicity
After excluding the five patients who could not recall the timing of attacks, 23 of the 37 (62.2%) patients had a circadian rhythmicity at baseline. Among them, five (21.7%) lost their circadian pattern, three (13.0%) had a shift in their circadian predilection, and only 15 (65.2%) maintained their original circadian rhythmicity. All 14 (37.8%) lacking a circadian rhythmicity at baseline did not develop any circadian rhythmicity at follow-up. Finally, only 15 (40.5%) showed a consistent circadian rhythmicity during the entire disease course (Figure 2(c)).
Autonomic symptoms
At baseline, 40 (95.2%) patients had prominent autonomic symptoms accompanying their attacks. Temporal changes of autonomic symptoms were assessed in 36 patients (three with a single bout and three having a difficulty in their recall). Among the remaining 36 patients, 27 (75.0%) had unchanged autonomic symptoms, while eight (25.0%) reported significant regression of their autonomic features (Figure 2(d)). Among these eight patients, seven did not use any acute treatment because they found it ineffective. Thus, treatment was not the reason for their loss of autonomic symptoms.
Disease course of the CH
Disease courses of total patients are summarized in Figure 3. At the follow-up evaluation, 14 patients (33.3%) showed remission, while 28 (66.7%) had active disease. No patients were converted to chronic CH. None of the baseline characteristics, such as age at onset or average lengths of bouts and out-of-bout periods, predicted the remission (Table 2). Current age was older in the remission group (median, 48 years; interquartile range, 43–69). The remission group reported their last bouts at a mean age of 42.3 years (median 38 years; interquartile range 36–52; range, 27–65), which did not differ from the age at the last bout in the active group (p = 0.623). Compared to the active group, patients in remission showed a trend toward fewer lifetime bouts (median 3 vs. 12 bouts, p = 0.063) and shorter disease duration (median 7.5 vs. 13.0 years, p = 0.090). Seasonal and circadian rhythmicities were frequently reported at baseline in the active group (76.0% and 73.1%), but the frequency decreased over time to 32.0% and 34.6%, respectively. On the contrary, patients in remission had fewer seasonal and circadian patterns at baseline (36.4% and 36.4%; p = 0.056 and 0.063 vs. the active group, respectively). Although not statistically significant, side shifting was more common in the active group (29.2% vs. 8.3% in the remission group, p = 0.224), while the disappearance of autonomic symptoms was frequent in the remission group (40.0% vs. 16.0% in the active group, p = 0.186). The other CH features did not differ between the two groups.
Disease courses of total patients. Disease courses of all 42 patients are displayed as black bars, indicating a duration between the onset age and the age of the last bout. Remission of cluster headache (see the Methods section for the operational definition) is marked with a yellow bow. Characteristics according to the clinical course. y, years; w, weeks. The data are presented as number (percentage) or median (interquartile range). Calculated as the number of total lifetime bouts divided by the disease duration. Three patients with single bouts were excluded.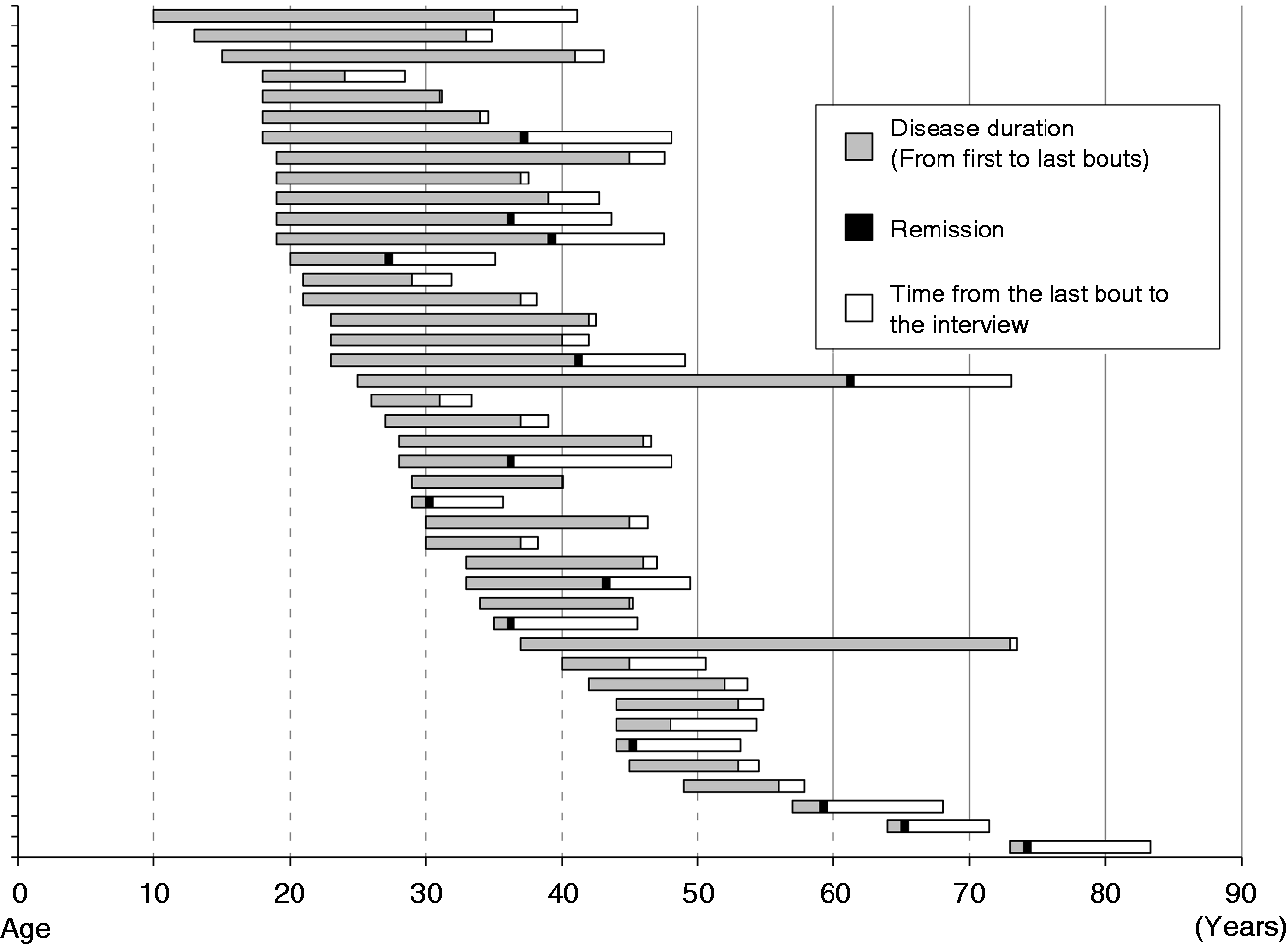
Pattern of CH remission
When we surveyed the 14 patients in remission about the change of CH features before the remission, diverse patterns of remission were observed (Figure 4). The lengths of the bouts and between-bout periods were either decreased, consistent, or increased during the disease course (Figure 4). Both the intensity and frequency of headache attacks were unchanged in most patients (64.3% and 57.1%, respectively), while other patients showed a reduction in either the intensity or frequency of attacks before the remission.
Pattern of remission. In 14 patients in remission, the length of bouts and out-of-bout periods was either increased, decreased, or unchanged before the remission. Intensity and frequency of headache were either unchanged or decreased.
Discussion
The main findings of this study are as follows:
The characteristics of CH including strictly unilateral location, seasonal and circadian rhythmicity, and autonomic symptoms becoming less prominent over time. Remission occurred at different ages with various patterns. There was a trend toward less circannual and circadian rhythmicity at baseline and fewer lifetime bouts and shorter disease duration during disease courses in remitted patients.
This is the first comprehensive study on the natural course of multiple features of CH. Our study subjects comprised two extreme subgroups of patients. Patients with active CH still had excruciating attacks but did not visit a clinic because of unsatisfying treatment effects or incorrect understanding of the disease. This enabled our survey on the natural course of the active cluster headache. A smaller group of patients did not visit because their CHs were remitted. The survey of patterns of remission was thus possible. Our ‘active but untreated’ patients show a need for further prospective assessments on treatment experiences to reveal the unmet need in patients with cluster headache.
Our data showed that characteristics of CH become less prominent over time. In particular, side-locked unilaterality, seasonal and circadian rhythmicity, and associated autonomic symptoms changed over the disease course. However, the clustering pattern remained. The length of between-bout periods generally increased, although some patients reported reduced or unchanged lengths of remission periods. Our comparative analysis showed that longitudinal changes in the CH characteristics were more common in active patients than in patients in remission. Patients in remission already have less seasonal and circadian rhythmicity at baseline. Our hypothesis is that loss of seasonal and circadian rhythmicity may be a sign toward disease remission. To test our hypothesis, active patients should be investigated in a further longitudinal follow-up (ClinicalTrials.gov Identifier: NCT02895256).
In our study, one-third of the patients who were lost to follow-up showed remission. Three studies reported different remission rates using different definitions. After Kudrow first reported prolonged remission in one-third of patients lost to follow-up (10), Pearce and Krabbe reported remission rates of about 10% in separate studies (9,11). Although the number of patients was small in our study, the rate of remission was similar to that in the Kudrow study (10). In our patients in remission, the last bout occurred at a wide range of ages, from 27 to 65 years. Our data were not in line with the concept that CH is a life-long disease (11). To confirm our findings, we will further follow up our cohort in a prospective setting (ClinicalTrials.gov Identifier: NCT02895256), because some exceptional cases can show CH recurrence after a long between-bout period (e.g. 15 years) (11).
Patients in remission had a tendency towards shorter disease duration and fewer lifetime bouts than active patients. The age of the last bout did not differ between remitted and active patients. There was no unique pattern of remission. Taken together, remission was not a consequence of more advanced age, longer duration of disease, or an accumulation of lifetime bouts. Alternatively, there might be a subgroup of patients having a more benign disease course. Increasing reports on patients who have only a single bout during their lifetime might represent an extreme form of benign CH (12). A multicenter, prospective, and longitudinal follow-up study is currently ongoing in Korean centers to elucidate the determinants of different disease courses in a large number of patients.
The major strength of our study was the detailed descriptions of the disease courses, which were directly obtained from patients by board-certified neurologists who specialize in headache disorders. This study has limitations. First, we only recruited specific patients lost to follow-up, who might not represent the whole cohort. Although some of our study subjects still had active attacks, our study subjects might have less severe disease compared to those who regularly visit the clinic. The clinical features, lengths of bouts or out-of-bout periods, and remission rate cannot be generalized to all patients with cluster headache. Second, the number of our study subjects was small, which was a result of the enhanced privacy protection policy in Korea. In addition, telephone interview harbors a risk of recall bias. Although we believe that patients showed a relatively good memory of their excruciating attacks, specific values such as lengths or frequencies may be inevitably incorrect. Third, our study subjects had a single ethnicity (i.e. Korean). The prevalence of chronic CH is generally low in the Asian population (13,14). There were no patients who showed a conversion to chronic CH in our study, which might be attributed to both the ethnicity and selection bias. Our study results warrant future studies in other ethnic groups before generalization. Finally, we operationally defined remission in this study. To date, a consensus definition for the remission of cluster headache is lacking. Longer observation from a large number of patients would be helpful for future studies.
In conclusion, distinct features of CH decrease over time. Remission occurs at different ages with diverse patterns. Patients in remission had less prominent circadian and circannual rhythmicities, fewer lifetime bouts and shorter disease duration. Remission might not be a consequence of more advanced age, longer duration of disease, or an accumulation of lifetime bouts. Our study warrants a larger prospective study to investigate the determinants of different disease courses and the disease-modifying effects of treatments.
Clinical implications
Distinct features of cluster headache decrease over time, while the pattern of clustering remains. Remission of cluster headache occurs at different ages with diverse patterns. Advanced age is not a predictor of remission, while patients in remission have a trend toward less prominent circadian and circannual rhythmicity at baseline, fewer lifetime bouts and shorter disease durations.
Footnotes
Acknowledgment
The authors thank Ms. Miran Jung for her help with data management.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.