
Abstract
Objective
To explore the prevalence of poor social support and loneliness among people with chronic headache, and how these might be effect modifiers in the relationships between chronic headache and stress, medication overuse, and self-rated health.
Background
Poor social support and loneliness are consistently linked to worse health outcomes. There are few epidemiologic studies on their effect on headache.
Methods
The Danish Capital Region Health Survey, a cross-sectional survey, was conducted in 2017. Participants were asked about headache, pain medication use, social support, loneliness, perceived stress, and self-rated health. Data were accessed from sociodemographic registers. Logistic regression analyses were performed to test for effect modification.
Results
The response rate was 52.6% (55,185 respondents) and was representative of the target population. People with chronic headache were more likely to report poor social support and loneliness compared to those without chronic headache (p < 0.0001 for both). Odds ratios for the combination of chronic headache and poor social support were very high for stress (odds ratio 8.1), medication overuse (odds ratio 21.9), and poor self-rated health (odds ratio 10.2) compared to those without chronic headache and with good social support. Those who reported both chronic headache and loneliness had a very high odds ratio for stress (odds ratio 14.4), medication overuse (odds ratio 20.1), and poor self-rated health (odds ratio 15.9) compared to those without chronic headache and low loneliness score. When adjusted for sociodemographic factors, poor social support and loneliness were not significant effect modifiers in almost all these associations. Loneliness was a significant effect modifier in the association between chronic headache and medication overuse, but exerted greater effect among those who did not report they were lonely.
Conclusion
Poor social support and loneliness were prevalent among people with chronic headache. The combination of chronic headache and poor social support or loneliness showed higher odds ratios for stress, medication overuse, and poor self-rated health compared to those with good social support and low loneliness scores. The effect of loneliness in the relationship between chronic headache and medication overuse warrants further study.
Introduction
There is a well-established link between headache and stress, and the relationship seems bidirectional. Stress has been described as a trigger for headache and is associated with increased headache frequency (1,2). Functional neuroimaging in the premonitory phase of migraine shows brain activation in the hypothalamus, which may be interpreted as stress (3,4). The relationship also goes in the other direction: People who develop severe headaches seem more likely to view adverse events and crises as stressful (4).
The relationship between headache and pain medication use is expected, but the co-existence of chronic headache and medication overuse is worrisome. This is because regular and frequent pain medication use can lead to medication-overuse headache (MOH), a debilitating condition characterised by almost daily use of acute pain medications without relief (5).
The link between headache and poor health is clearly seen in the Global Burden of Disease studies (6). People with chronic headache tend to score poorly in self-ratings of overall health, even after controlling for possible confounders: Demographic variables, income, education, employment, unhealthy lifestyle, and comorbidity (7).
Good social support is well documented as a protective factor in the development and management of chronic disease (8–12), and likely also of chronic headache. While the causal evidence of consequences of loneliness is inadequate, there are strong associations between loneliness and non-communicable diseases, poor health behaviours, stress, and poor health in general (13). There is growing knowledge on the relationships between loneliness and chronic pain (14,15), but there are few studies focused on loneliness and headache (16–18).
Among those with chronic headache, poor social support and loneliness might affect perception of one’s own health, thus lowering scores on self-rated health. Hence, the relationships between headache and stress, headache and medication overuse, and headache and self-rated health could very well be influenced by poor social support and loneliness.
The objectives of this study were therefore to analyse the prevalence of poor social support and loneliness among people with chronic headache, and to analyse how social support or loneliness might act as effect modifiers in the relationships between chronic headache and stress, between chronic headache and medication overuse, and between chronic headache and self-rated health.
We hypothesised that the prevalence of poor social support and loneliness was high among people with chronic headache, and these factors act as effect modifiers in these relationships.
Methods
Definition of terms
Chronic headache is defined as headache 15–30 days per month in the last 3 months. “Chronic headache” is used in this paper as a descriptive term. It is not an independent diagnosis listed in the International Classification of Headache Disorders version 3 (ICHD-3) (19).
Respondents were asked: How many days on average did you have migraine or headache in the last 3 months? The options were 0 days/month; 1–7 days/month; 8–14 days/month, and 15–30 days/month. The ordinal scale was used to make encoding simpler, and to harmonise the 2017 and 2010 questionnaires (20).
Participants were asked about their intake of pain medications per month in the last 3 months: over-the-counter medications for pain, specific medications (paracetamol, ibuprofen, combination preparations, opioids, triptans), and pain medications in general. Several commonly purchased brand names were listed with the generic names. The options were 0 days, 1–9 days, 10–14 days, and 15–30 days/month.
Pain medication overuse is defined as intake of paracetamol or ibuprofen ≥15 days per month or combination preparations/opioids/triptans/unspecified pain medications ≥ 10 days per month in the last 3 months.
A case of MOH refers to a respondent with chronic headache who also fulfils the criteria for medication overuse. This case definition approximates Criteria A and B of the ICHD-3 diagnostic criteria for MOH. Previous analyses of the data used in this study showed that chronic headache prevalence was 3.0% (95% CI: 2.3–3.2) and MOH prevalence was 2.0% (95% CI: 1.8–2.1) (20) which are consistent with global data (5).
Social support is defined as “an exchange of resources between two individuals perceived by the provider or the recipient to be intended to enhance the well-being of the recipient” (21). The exchange can also occur between an individual and groups or organisations, leading to a transaction that meets the recipient’s basic social needs.
In this paper, social support is measured by the quantity (rather than the quality) of these exchanges. Poor social support is defined as a response of “less than once a month” or “never” for contacts with family or friends; or a response of “often” to the question “Are you alone even though you want to be with other people?”, or a response of “no, never or almost never” to the question “Do you have somebody to talk to if you have problems or need support?”.
Loneliness can be defined as unwanted solitude (22), “the discrepancy between a person’s preferred and actual level of social contact” (23), or “the subjective feeling of the absence of a social network or a companion” (12).
The University of California, Los Angeles Loneliness Scale (24) is the most widely used questionnaire on loneliness. The Three-Item Loneliness Scale (T-ILS) is a short version of this questionnaire (25) and has been translated into Danish (26).
The T-ILS focuses on these items: How often do you feel isolated from others? How often do you feel that you lack companionship? How often do you feel excluded? (22,26,27). The response options were seldom, sometimes, and often; each assigned a score of 1, 2, or 3, respectively. The responses generated a scale ranging from 3 to 9. A high score indicated a high degree of loneliness. Respondents should have answered at least two of the three questions to be included in the analyses (26–28). Respondents were categorised as lonely if the sum was ≥7; or the sum was 6 and one of the three answers was missing. Respondents were categorised as not lonely if the sum was <7 and all three questions were answered.
Stress has been defined in headache research as “a state of mental or emotional strain or tension resulting from the perception of adverse, demanding, threatening or dangerous circumstances” (4). Stress was assessed in this study using the Perceived Stress Scale (PSS), a 10-item questionnaire that quantifies “the degree to which situations in one’s life are appraised as stressful”. It measures how much a respondent experiences life as unpredictable, uncontrollable, and over-loaded during the past month (29). Responses were scored 0–4 on a Likert scale (range 0–40) with higher scores indicative of more stress. Earlier studies on the Danish population analysed stress data in terms of quintiles, with the highest 20% designated as being the most stressed. This group had a PSS score of ≥18 (30). In the current study, this score is used as the cut point for a high level of stress.
Self-rated health was measured as a single-item taken from the Short-Form 12: “In general, would you say your health is…”. The response options were excellent, very good, good, fair, or poor (31). Responses were dichotomised as either poor or fair to excellent.
The Danish Capital Region Health Survey
The Danish Capital Region Health Survey (DK-CRHS) of 2017 is a cross-sectional health survey conducted in 29 municipalities in the Capital Region of Denmark. The survey was conducted from February to May 2017 and was part of The Danish National Health Survey (DNHS) (30,32). Similar to the DNHS of 2010 and 2013, a core set of 50 questions was used in all five regions of Denmark. In 2017, the T-ILS, as well as questions on chronic headache and medication overuse, were added to the DK-CRHS.
The sampling frame included all adults ≥ 16 years residing in the Capital Region of Denmark as of 1 January 2017. Respondents were randomly drawn from the Civil Registration System, which contains demographic records on all Danish residents. Residents are allocated personal 10-digit Central Person Registry numbers, which were used to link data from all participants of the DK-CRHS with national registers at Statistics Denmark. These registers contain information on age, sex, ethnicity, educational attainment, employment status, and income (33,34).
Sampling and data collection methods have been previously described (20).
Statistical analyses
Responses to questions on social support, loneliness, stress, and self-rated health were summarised as proportions with standard errors. Missing responses were excluded in calculating proportions. Spearman correlation coefficients were calculated to examine relationships between continuous or ordinal variables.
Logistic regression analyses were used to test associations between (1) chronic headache and stress; (2) chronic headache and medication overuse; and (3) chronic headache and poor self-rated health. Interaction terms between the independent variable and poor social support or loneliness, respectively, were included in the models. Adjusted models included the following sociodemographic factors: Sex, age group, ethnicity, civil status, educational attainment, employment status, and income (Figure 1). All analyses were weighted for non-response and survey design. Survey procedures were used for the analyses. Survey weights were computed by Statistics Denmark based on information about sex, age, municipality, educational attainment, income, civil status, and hospitalisation.

Model of the relationships between chronic headache and three outcome variables, possible effect modifiers (poor social support or loneliness), and known confounders.
SAS software (v. 9.4 TS1M5; SAS Institute, Cary, NC) was used for all analyses. All p-values were two-sided with a level of significance at p < 0.05.
Results
A total of 104,950 questionnaires were distributed. The response rate was 52.6%. There were 55,185 respondents, among whom 54,318 answered the headache-related questions. There were 1491 respondents (2.7%) who reported chronic headache. Among those with chronic headache, 991 (66%) were classified as having MOH. Chronic headache and MOH prevalence by age, sex, and socioeconomic position, adjusted for sampling method and non-response, have been previously reported (20).
Descriptive analyses
Significantly more people with chronic headache had poor social support compared to those without chronic headache (36.7% vs. 20.5%, p < 0.0001, Table 1).
Reports of social contacts, unwanted solitude, loneliness, a high level of stress, poor social support, and poor self-rated health among respondents, classified according to headache type.

Note: Missing responses were excluded in calculating proportions.
SE: standard error of percent
1 Contact refers to being physically together, talking on the phone, or writing to each other.
2 Poor social support was defined as a response of “less than once a month or never” for contacts with family (A) or friends (B); or a response of “often” to question C; or a response of “no, never or almost never” to question D.
3Items E, F, and G comprise the Three-Item Loneliness Scale (T-ILS). Response options were assigned a score of 1 (seldom), 2 (sometimes), or 3 (often). Responses generated a scale ranging from 3 to 9. A high score indicates a high degree of loneliness. Respondents were categorised as lonely if the sum was ≥7, or the sum was 6 and one of the three answers was missing. Respondents were categorised as not lonely if the sum was < 7 and all three questions were answered.
4High level of stress: Perceived stress score ≥18
5Poor self-rated health: Response to a single item taken from Short-Form 12 referring to one’s assessment of overall health.
Based on overall T-ILS score, loneliness was more common among those with chronic headache compared to those without chronic headache (23.8% vs. 7.7%, p < 0.0001, Table 1).
Further analyses showed that the subgroup with MOH fared worse compared to those with chronic headache without medication overuse, particularly in their infrequent contact with friends, lack of people to talk to when they needed support, and in all T-ILS questions.
Although more people with MOH reported poor social support and loneliness compared to those with chronic headache without medication overuse, the differences were only significant for poor social support (39.1% vs. 32.2%, p = 0.0479); but not for loneliness (24.4% vs. 22.5%, p = 0.5374).
High stress scores were seen in the large majority of those with chronic headache (60.8%) compared to those without chronic headache (24.5%, p < 0.0001). The proportion was even higher among those with MOH (65.6%, compared to those with chronic headache without medication overuse, 51.4%, p < 0.0001).
Only 13.8% of those without chronic headache rated themselves as being in poor health, compared to 51.7% among those with chronic headache (p < 0.0001). The proportion was higher among those with MOH compared to those with chronic headache but no medication overuse (58.7% vs. 38.2, p < 0.0001).
Headache days, stress score, self-rated health, and loneliness score were all positively correlated. The highest correlations were found for stress score and loneliness score, and self-rated health and loneliness score (Table 2).
Spearman correlation coefficients for continuous and ordinal variables.

Logistic regression analyses
Respondents with chronic headache had more than three times higher OR for stress compared to those without chronic headache (OR 3.4, Table 3).
Odds ratios for stress with chronic headache as the independent variable, and with combinations of level of stress and social support, and level of stress and loneliness
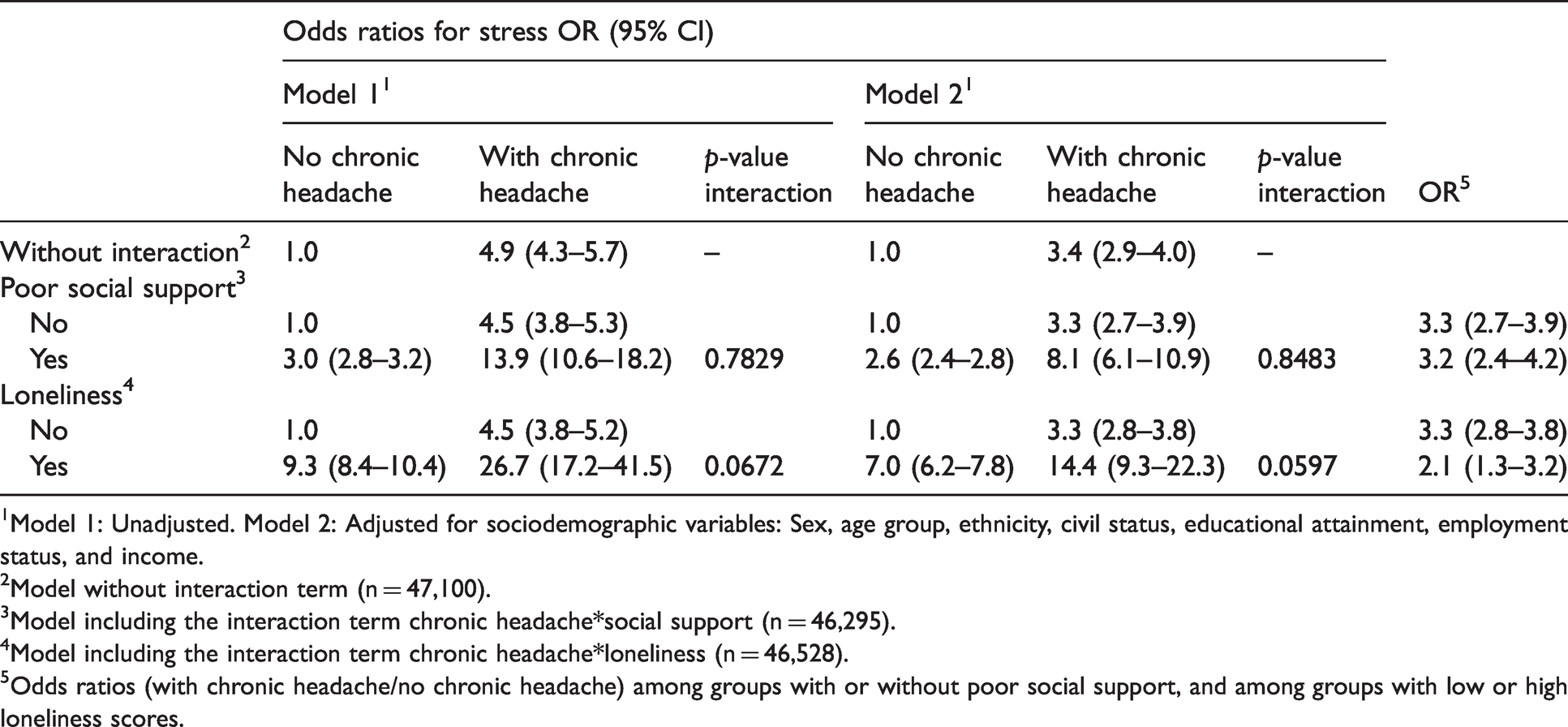
1Model 1: Unadjusted. Model 2: Adjusted for sociodemographic variables: Sex, age group, ethnicity, civil status, educational attainment, employment status, and income.
2Model without interaction term (n = 47,100).
3Model including the interaction term chronic headache*social support (n = 46,295).
4Model including the interaction term chronic headache*loneliness (n = 46,528).
5Odds ratios (with chronic headache/no chronic headache) among groups with or without poor social support, and among groups with low or high loneliness scores.
The combination of chronic headache and poor social support was associated with eight times higher OR for stress (OR 8.1, Table 3) compared to those without chronic headache and with good social support. Those who reported both chronic headache and loneliness had a very high OR for stress (OR 14.4, Table 3) compared to those without chronic headache and low loneliness score.
There was no statistically significant interaction between chronic headache and poor social support or loneliness in the association with stress after adjusting for socioeconomic factors.
Table 4 shows that the OR for medication overuse was very high among those with chronic headache compared to those without chronic headache in the fully adjusted model (OR 17.6). The combinations of chronic headache and poor social support, or chronic headache and loneliness, were associated with very high ORs for medication overuse (OR 21.9 and OR 20.1, respectively).
Odds ratios for medication overuse with chronic headache as the independent variable, and with combinations of headache status and social support, and headache status and loneliness.

1Model 1: Unadjusted. Model 2: Adjusted for sociodemographic variables: Sex, age group, ethnicity, civil status, educational attainment, employment status, and income.
2Model without interaction term (n = 48,531).
3Model including interaction term level of chronic headache*social support (n = 47,613).
4Model including the interaction term level of chronic headache*loneliness (n = 47,846).
5Odds ratios (with chronic headache/no chronic headache) among groups with or without poor social support, and among groups with low or high loneliness scores.
In the absence of chronic headache, the OR for medication overuse was relatively low among those with poor social support (OR 1.4), or those with high loneliness scores (OR 1.9).
There was no statistically significant interaction between chronic headache and poor social support in the association with medication overuse.
There was a statistically significant interaction between chronic headache and loneliness in both unadjusted and fully adjusted models (p = 0.0038 and p = 0.0156, respectively). Headache was more strongly associated with medication overuse among individuals who did not report that they were lonely (OR = 19.2) than among those who were lonely (OR = 10.8).
Respondents with chronic headache had almost six times higher OR for poor self-rated health compared to those without chronic headache in the fully adjusted model (OR 5.8, Table 5).
Odds ratios for poor self-rated health with chronic headache as the independent variable, and with combinations of headache status and social support, and headache status and loneliness.
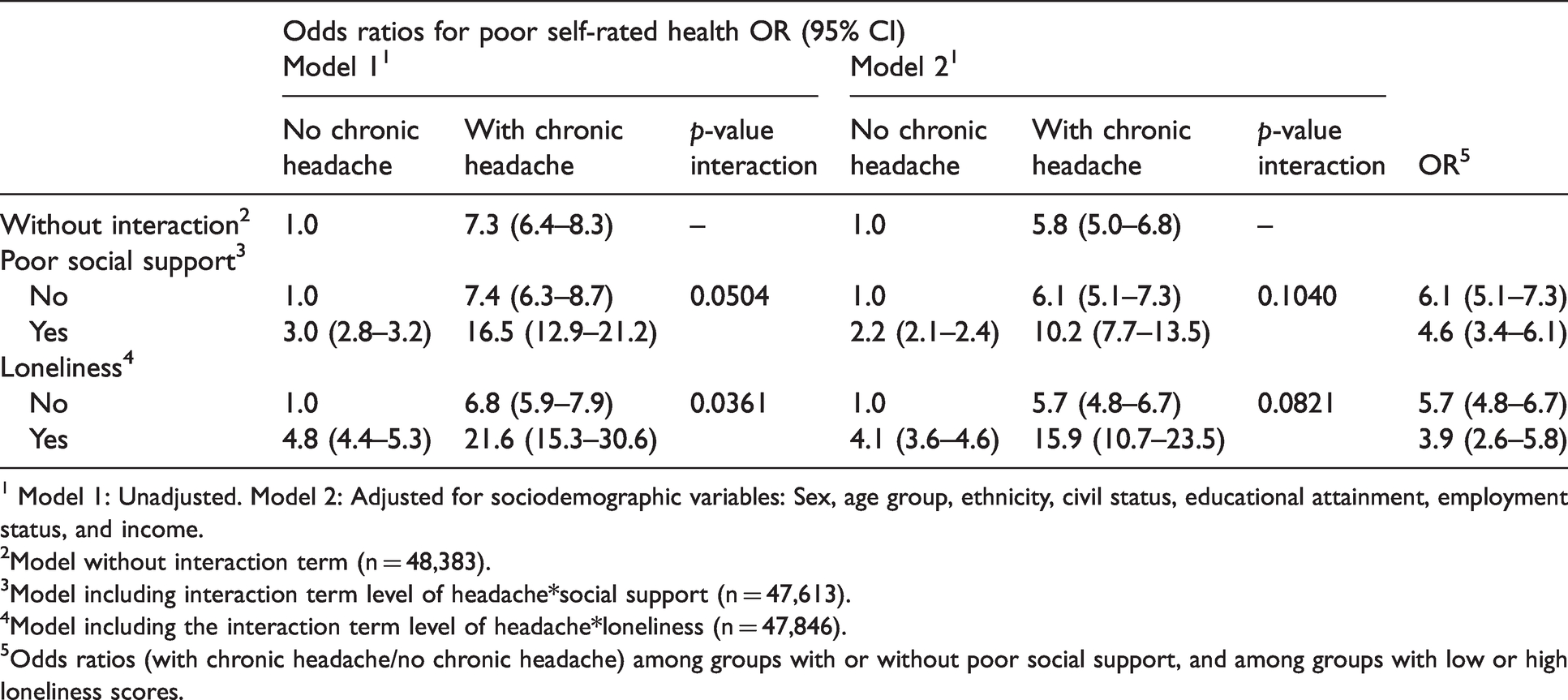
1 Model 1: Unadjusted. Model 2: Adjusted for sociodemographic variables: Sex, age group, ethnicity, civil status, educational attainment, employment status, and income.
2Model without interaction term (n = 48,383).
3Model including interaction term level of headache*social support (n = 47,613).
4Model including the interaction term level of headache*loneliness (n = 47,846).
5Odds ratios (with chronic headache/no chronic headache) among groups with or without poor social support, and among groups with low or high loneliness scores.
The combination of chronic headache and poor social support was associated with a high OR for poor self-rated health (OR 10.2) compared to those without chronic headache and good social support. The relationship was similar for those with chronic headache and high loneliness score (OR 15.9) compared to those without chronic headache and low loneliness score.
Tests for poor social support or loneliness as possible effect modifiers, were not significant in the fully adjusted model.
Discussion
Our analyses show that people with chronic headache were more likely to report poor social support and loneliness compared to those without chronic headache (p < 0.0001 for both variables). The associations between chronic headache and stress (OR 3.4), chronic headache and medication overuse (OR 17.6), and chronic headache and poor self-rated health (OR 5.8) were very strong even after adjustments. Odds ratios for the combination of chronic headache and poor social support were very high for stress (OR 8.1), medication overuse (OR 21.9), and poor self-rated health (OR 10.2) compared to those without chronic headache and with good social support. Those who reported both chronic headache and loneliness had a very high OR for stress (OR 14.4), medication overuse (OR 20.1), and poor self-rated health (OR 15.9) compared to those without chronic headache and low loneliness score. However, poor social support and loneliness were not significant effect modifiers in almost all these associations after adjusting for sociodemographic factors.
Lack of social relationships is considered a major risk factor for chronic illness, “rivalling the effects of well-established health risk factors such as cigarette smoking, blood pressure, blood lipids, obesity, and physical activity” (35). Longitudinal studies show how good social relationships moderate the impact of physical health problems and improve emotional well-being throughout the life course up to old age (36).
In the current study, poor social support and loneliness are clearly more common among those with chronic headache.
On headache and poor social support
The ways by which social support influences health have been described in terms of the direct effect model, wherein a person is integrated in a network of social relations that increases health-promoting behaviours and provides appropriate resources. The perception that help is available increases a person’s overall self-esteem, stability, and perception of control over one’s environment. These factors together decrease susceptibility to physical illness (37).
In the stress buffering model, the protective functions of social support appear at two points during a stressful event: Intervening between the event and the stress experience, or between the stress experience and the pathological outcome (37).
Social support can be described in terms of type, source, quantity, or quality. Support can come in the following forms: Emotional, instrumental, informational, and appraisal. These are influenced by the types of social relationships a person has, and the characteristics of this social network (such as size, density, reciprocity, frequency) (38).
The four questions used to describe social support in this study showed only quantity (contact with family or friends; being alone) and form of support (someone to talk to when one has problems). The assumption was that quantity influences wellbeing in a positive way; that is, the contacts were helpful to the recipient.
The earliest epidemiologic study on headache in Denmark showed that men with tension-type headache (TTH) more frequently reported having nobody (close relatives, friends, or others) to talk to about personal matters, compared to men with other headache types, although the difference was not significant (39). A later study with a larger sample size showed that not having a close friend was associated with higher incidence of migraine (40).
In Sweden, poor social support and being belittled has been associated with increased prevalence of recurrent headache or migraine (41). An earlier study found that not having a close friend was associated with analgesic use among men but not women (42).
Headache sufferers have a smaller network of close confidantes (43) or close social contacts (44,45), and those with few friends tend to have more severe symptoms (46).
Headache sufferers place importance on tangible support from a partner, and emotional support from other family, friends and acquaintances, although they tend to be less satisfied with the support that is available (47–49). Social support may not be related to headache reporting (50), but it can be a component of a range of management strategies (51).
On headache and loneliness
There are very few studies on loneliness and headache. Loneliness is associated with a range of somatic symptoms including headache in children (16) and adolescents (52). Loneliness seems to play a role in the complex relationship between interpersonal violence and headache (18,53). In a study specific for migraine, people with chronic migraine are more likely to report feeling lonely compared to those with episodic migraine, and are less likely to be satisfied with the quality of care they receive or their ability to self-manage their headaches (54).
A previous analysis of DNHS data shows that the prevalence of loneliness in Denmark is about 8%, as measured by T-ILS (55). Danish data also show that even after adjusting for sociodemographic factors, there is a higher prevalence of loneliness among those with a range of chronic illnesses, including migraine (OR > 1.50). For migraine, these findings are consistent in all age groups. Respondents report loneliness despite having regular contact with family and/or friends, suggesting that the quality of social contact is possibly more important than the quantity (55, 56).
In our analysis of respondents without chronic headache, 7.7% scored high in the T-ILS questions, which is consistent with the national average of 8% (55, 56). Of note, prevalence was much higher among those with chronic headache (23.8%) and MOH (24.4%).
On headache and stress
The current study mirrors the analysis of DNHS data from 2010, which showed strong associations between chronic headache, MOH, and stress (57).
Inadequate social support has been considered as a “setting antecedent” for headache because this increases vulnerability to stress, which is an “immediate antecedent” or precipitating factor for headache. If headache spoils social functions, it may lead to “a reduced social network and less social support, which makes headache sufferers more vulnerable to stress” (2). Headache sufferers might use ineffective coping strategies in dealing with stress (e.g. avoidance, social withdrawal), rather than tapping sources of social support (2).
Previous studies theorise that when a threshold of psychological wellbeing is breached, the resulting distress could increase the risk of persistent migraine or TTH (17,53,58,59). It is possible that the change in stress level (i.e. relaxation after stress, rather than stress itself) triggers migraine headaches (60,61). Persons with other types of secondary headaches are also more likely to report high psychological distress (62).
High stress is associated with poor lifestyle behaviours like alcohol abuse, smoking, overweight and physical inactivity (63). Both stress and poor lifestyle behaviours are likely to worsen or increase the frequency of headaches (57,64,65). A prospective study showed that two consecutive days of either high stress or low sleep were strongly predictive of headache (66).
It is possible that headache pain affects cognitive abilities and reduces problem-solving capacity, thereby generating stress (67), but the cause-effect relationship is unclear. Although the statistical analysis in this study modelled stress as a consequence of headache, the relationship is likely bidirectional and there is a “vicious cycle of stress-headache-stress” (2).
On poor social support and loneliness as effect modifiers
We looked at poor social support and loneliness as possible effect modifiers in the relationships under study, since it might be possible to intervene in these areas, and produce better outcomes under treatment. We found that the interaction terms included in the models were not significant after adjusting for sociodemographic factors, with the exception of the analysis involving loneliness and medication overuse. Contrary to what was expected, the effects were stronger among people who did not report they were lonely. This can be seen by calculating the ratio among individuals who did not report that they were lonely and among those who were lonely (Table 4, OR 19.2 versus 10.8).
We hypothesise that overuse of medication in people with chronic headache might be related to the need to participate in social interactions. This process was explored in a qualitative study conducted in Sweden, describing how participants with MOH held on to “indispensable medications” since these were perceived as the only thing that could prevent headaches from ruining their social interactions (68).
Implications for the treatment of chronic headache and MOH
Poor social support probably decreases self-efficacy, while loneliness limits use of active coping methods (69). In contrast, supportive social relationships may influence health via adoption and maintenance of healthy behavioural norms, allowing individuals to resist risky behaviour and maintain healthier choices.
Despite its importance, improving support among patients with headache is the least-used management strategy, trailing behind direct contact with health care providers (70,71). Nonetheless, it makes sense to study models of care that address loneliness and poor social support among patients with chronic headache (54). An example is the promising experience of youth camps for adolescents with chronic headache (72). Other examples are workplace accommodations to increase productivity in workers with migraine (73). Therapy delivered to groups of people with headache (focused on education, non-pharmacological treatment, psychotherapy, and self-management) show promise and may be more effective than individual delivery (74–77). There may, however, be negative effects of improving support, such as pain avoidance, over-dependence on others, and reinforcement of anxieties (78). Hopefully, high-quality randomised control trials such as the CHESS trial (79) can shed more light in this area.
Our results show that at the very least, in clinical practice, history taking should include questions on social support and loneliness, with the aim of delineating factors affecting morbidity, and pointing these out to patients as possible modifiable risk factors for poor outcomes.
Strengths and limitations
This study uses a large sample size that is representative of the target population (30,32). The questionnaires and method of data collection have been continually improved since the earlier studies in 2010 (7,20,57). Regression analyses were controlled for a range of sociodemographic factors using reliable register data.
The questions for perceived stress, loneliness, and self-rated health were validated (26,29,31). Measures of social support, however, were not validated.
The questions on social relationships have been part of the repeated survey questionnaire since 2010. These questions focused only on frequency of contact, and do not give an indication of quality or adequacy of support. The Interview Schedule for Social Interaction (ISSI), Interpersonal Support Evaluation List (ISEL), and Social Support Questionnaire (SSQ), have been used in headache research (80–82). These are too long to be included in this large population-based survey but could be the basis for future targeted studies.
A limitation of the T-ILS is that it does not specify a duration, and therefore it does not differentiate between long-term and short-term loneliness.
Psychological and behavioural characteristics like high social anxiety and poor social skills (59,62) were not explored in the questionnaire.
A headache diagnostic questionnaire; for example, from the Lifting The Burden studies (83) could not be implemented. It was therefore not possible to distinguish between headache types and point to possible differences between respondents with migraine, tension-type headache or other headache forms. On the positive side, the survey looked at a broad range of health variables and was not specific for headache.
No reliability study was conducted for headache reporting in our dataset. This limitation was studied in Norway and their results indicate good reliability (84).
Our cross-sectional study cannot establish causality or determine the directionality of associations. However, the data can be used to test a range of relationships between variables, and support future efforts toward longitudinal studies, which can clarify temporal relationships between social support, loneliness, and headache-related disability.
Data were collected in 2017 but this paper was written in the autumn-winter of 2020, at a time when COVID-19 was calling into question the standard definitions of social support and loneliness at the population level. Social distancing, remote work and schooling, limited access to elderly care homes and the seriously ill in hospitals, represent population-wide challenges. The effects of the pandemic on mental health are only beginning to be described (85), and are unlikely to be reflected in the data presented here.
Conclusion
Our data show that poor social support and loneliness are prevalent among people with chronic headache. There are strong associations between headache and stress, medication overuse, and poor self-rated health. The combination of chronic headache and poor social support or loneliness show higher ORs for stress, medication overuse, and poor self-rated health compared to those with good social support and low loneliness scores. These relationships are influenced by sociodemographic factors. The effect of loneliness in the relationship between chronic headache and medication overuse warrants further study.
Ethics approval and patient consent
Participation was voluntary. Information on the objectives of the Danish National Health Survey were stated on the questionnaire and on the project website https://danskernessundhed.dk/. The objectives of the survey were: i) to describe the prevalence and distribution of health and morbidity in the adult population in Denmark, ii) to gather data for use in health services planning, and for analysis of regional and municipal differences, and iii) to describe the development of health and morbidity in the adult population in Denmark from 2010 to 2017. Informed consent for use of the data was given upon return of the questionnaire. The questionnaire used and the main results of the survey are accessible to the general public via the website.
This study is part of the Sundhedsprofil (Health Profile) project (P-2020-110, CSU-FCFS-2016-016, I-suite: 05067). It was approved by the Danish Data Protection Agency according to the Danish Act on Processing of Personal Data. Approval from the Danish Health Research Ethics Committee System was not required according to The Act on Research Ethics Review of Health Research Projects, Section 14, because the project was based on data from questionnaires and registers and did not collect human biological samples.
Public health relevance
Lack of social relationships is a major risk factor for chronic illness. This appears to be true also for chronic headache. In this study, poor social support was more likely to be reported by people with chronic headache than those without. Loneliness prevalence among those without chronic headache (7.7%) was similar to national data, but prevalence was much higher among those with chronic headache (23.8%) and MOH (24.4%). The combination of chronic headache and poor social support, and the combination of chronic headache and loneliness, showed very high odds ratios for stress, medication overuse, and poor self-rated health compared to those without chronic headache and good social relations. In clinical practice, history taking should include questions on social support and loneliness, with the aim of delineating factors affecting morbidity.
Footnotes
Acknowledgements
Special thanks to Rennette Christine Mørkøv Jensen for summarising the findings of early headache studies related to social support and social networks, and to Signe Thorup Gjendal for the preliminary statistical analyses.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MLW, CJL, KA, and AHA declare no conflict of interest. RHJ received grants from Tryg Foundation during the conduct of the study and grants from Lundbeck Foundation and Novo Nordisk Foundation outside the submitted work; conducted clinical trials for Eli Lilly Company, ATI, Lundbeck Company and ElectroCore, Inc; gave lectures for ATI, TEVA Pharmaceutical Industries, Novartis International AG, and Allergan plc; and serves as director of Lifting The Burden and the Danish Headache Center.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported financially by Tryg Foundation. The Danish Capital Region Health Survey 2017 was funded by The Capital Region of Denmark.