
Abstract
The majority of people with primary headache disorders live in the developing world. The contribution of low and middle income (LAMI) countries to headache research has not been previously characterized. A search was performed for clinical research publications between the years 1997 and 2006, using the search terms ‘headache’ OR ‘headache disorders’ AND ‘primary’ OR ‘migraine’ AND ‘each of the LAMI countries’ in 67 databases. Articles in English or with abstracts in English translation were included. These publications were scrutinized for study characteristics. Two hundred and twenty-seven publications from 32 LAMI countries were found. Half (50.2±) of these were from three middle-income countries (Brazil, Turkey and Iran), whereas 24 (10.6±) came from low-income countries. Most of the research focused on migraine. Only 29.5± of the articles involved treatment of headache. The understanding of headache disorders in LAMI countries is derived from a limited number of publications from relatively few countries. Identifying gaps in headache research in the developing world is strategic for targeting research policy.
Introduction
Headache is a painful and common symptom. A number of primary headache disorders have been characterized, including tension-type headache, migraine and cluster headache, and overall these disorders account for approximately 95% of all headache complaints (1). Headache also occurs as a typical symptom of a range of other health conditions, the so-called ‘secondary headaches’(2).
Primary headache disorders are a significant, largely unaddressed burden of ill health and disability everywhere (3). Where studied, primary headache disorders have a lifetime prevalence of 90% (4). Migraine on its own ranks among the top 20 causes of years of life lived with disability (YLD) (5). Tension-type headache afflicts 80% of women and two-thirds of men living in developed countries (3).
The epidemiology and experiences of patients with headache disorders in the developing world are uncertain, because the majority of research on headache disorders comes from a limited number of high-income countries. Where sought, regional variation in the incidence, prevalence and economic burden of headache disorders has been found (3). Social, financial and cultural factors can all influence the experience of the individual headache sufferer, and patients in resource-poor settings could presumably experience an even greater impact of these influences. Yet the contribution of low- and middle-income (LAMI) countries to the understanding of headache disorders has not been characterized. It is vital to recognize the scientific outputs from these countries to establish new knowledge and adapt and benefit from research conducted globally. Research done locally is a much better tool to generate awareness, shape policy and encourage service development. Moreover, some countries may have higher than expected numbers of headache sufferers than experts could predict based on data found in high-income countries. Treatment strategies and programmes based on data from wealthier settings may not be generally applicable when they are introduced globally.
This study set out to determine the types and amount of research on primary headache disorders in LAMI countries over the past decade. With characterization of the existing research output and capacity in LAMI countries, future priorities can be more readily established.
Methods
Country classification by income level was based on World Bank categorization (6) into four groups according to 2005 gross national income per capita: low [≤ $875 (≤ £437)], lower middle [$876–3465 (£438–1732)], upper middle [$3466–10 725 (£1733–5362)] or high [≥ $10 726 (≥ £5363)]. World regions (Africa, the Americas, the Eastern Mediterranean, Europe, South-East Asia and the Western Pacific) were determined by the World Health Organization (WHO) distribution of member states (7).
Essential to this search was a list of international databases for medical and allied health publications that have been collected by the WHO library over recent years, recording special interest and country-specific search engines. PubMed, as well as 66 other internationally accessible databases including Embase, Literatura Latino-Americana e do Caribe em Ciências da Saúde, African Index Medicus, Eastern Mediterranean Regional Index Medicus, IndMed and others, were searched using the keywords ‘headache’ OR ‘headache disorders’ AND ‘primary’ OR ‘migraine’ for the years 1997–2006 inclusive. Appendix 1 provides the list of databases searched. The other common primary headache disorders, namely tension-type headache and cluster headache, were not used as keywords since both terms include ‘headache’, which itself was a keyword in the search strategy. Each LAMI country name, as listed by the World Bank in 2006 (6), was an additional search term, with appropriate substitutions for country name changes as necessary (e.g. ‘Laos’ for ‘People's Democratic Republic of Lao’, ‘Atlantic Islands’ for ‘Solomon Islands’, or ‘Yugoslavia’ for ‘Bosnia-Herzegovina’ and/or ‘Serbia and Montenegro’). When a country was not a Medical Subject Heading term or keyword, and a substitution could not be used (e.g. ‘Faeroe Islands’), abstracts were reviewed by looking at the institutional affiliation of the corresponding author and geographic region where the work was conducted.
All types of clinical research, including case series, clinical trials and retrospective studies in any language, were included provided that the article or an abstract of it was available in English. Basic science articles and animal studies, when found, were excluded. Also excluded were single case reports and publications that did not present new clinical research data such as commentaries, biographies, historical articles, reviews, conference summaries, viewpoints, editorials, interviews and guidelines.
Each abstract was evaluated by two authors (F.J.M., T.D.) to ensure that it was (i) derived from that particular country and not about relocated migrants from that country, and (ii) pertained to primary headache as defined by the International Classification of Headache Disorders, 2nd edn (2). Articles that discussed headache as a symptom rather than as a disorder were excluded. Upon careful review of each abstract and/or article, all work pertaining to secondary headache (e.g. oral contraceptive use, Dengue fever, trauma, hypertension) was also excluded.
Abstracts and/or articles were scrutinized and categorized according to age of population studied (paediatric vs. adult or both), type of research (medication/drug-related study, non-medication/drug-related clinical study, epidemiological study or health services/economic study), location of study (community vs. hospital or clinic), journal of publication, country of residence of corresponding author and type of headache disorder studied (migraine vs. other primary headache disorder or both).
Studies were also classified as single or multicentred; those studies with data contributions from centres in different countries were counted once for each LAMI country that participated. In this way, a single article was counted twice if two LAMI countries participated in the finished product and five times if five LAMI countries participated in the finished product.
For comparison, high-income countries were searched individually in PubMed and Embase for the presence or absence of research publications in the time period studied.
Results
Although a few countries were prolific, most LAMI countries published nothing. A total of 227 research publications pertaining to primary headache disorders were found, with more than half coming from three middle-income countries: Brazil (n = 57), Turkey (n = 31) and Iran (n = 26). A full list of reviewed papers is available from the corresponding author on request. Thirty-two of a possible 151 LAMI countries were represented (Table 1). Most articles were found via PubMed (62.5%), but significant proportions were indexed only in Embase (15.0%) or other databases (22.5%).
Research in the primary headache disorders by World Bank income group (6), 1997–2006

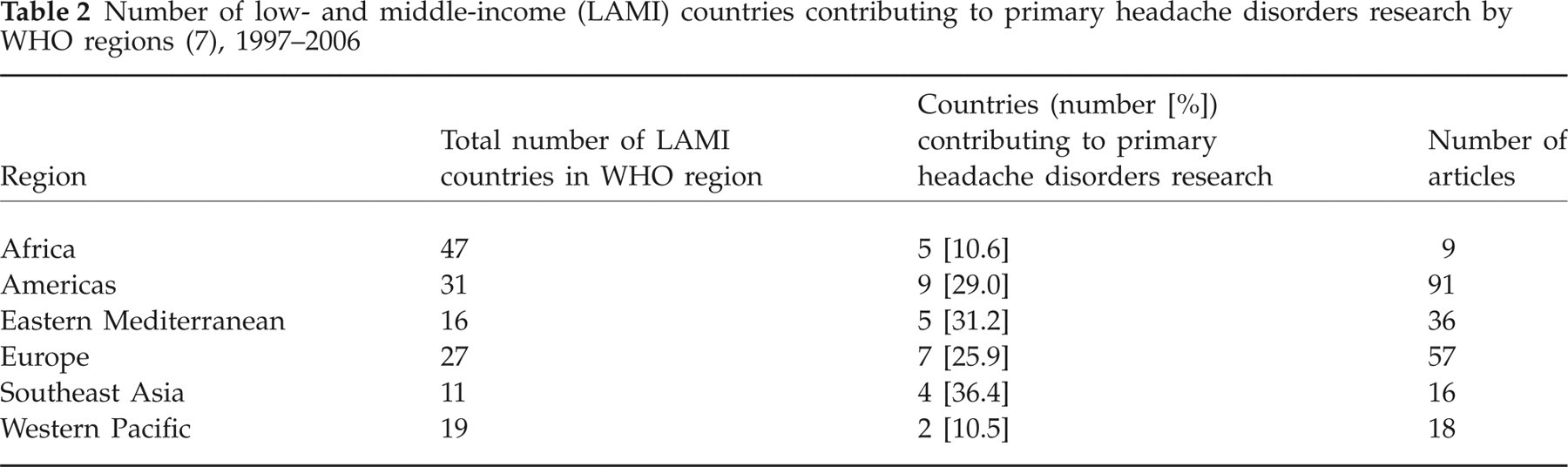
Eight out of a possible 54 low-income countries produced research in the primary headache disorders. Of a total of 24 publications from these countries, two had primary authors from institutions in high-income countries. Amongst WHO regions, Africa published the least number of articles overall and the lowest percentage of articles per number of LAMI countries in a region (Table 2). The number of publications per year in the African region did not show signs of increase in later years.
Number of low- and middle-income (LAMI) countries contributing to primary headache disorders research by WHO regions (7), 1997–2006
In general, there was a trend towards greater participation in research as the income level of countries increased from low to middle to high income. This had a gradient effect, with low-income countries producing the least numbers of manuscripts. Nevertheless, only two-thirds of high-income countries produced research in the headache disorders in the past decade (Table 1).
Migraine was the focus of 111 articles (48.9%). Non-migraine primary headache disorders were the subject of 60 articles (26.4%), whereas 56 articles (24.7%) focused on both. Paediatric populations were studied exclusively in 15.0% of the total publications. Approximately one-third (29.5%) were concerned with treatment of headache, including pharmacological management (14.5%), acupuncture and/or lifestyle changes (15.0%). Nearly half (44.5%) of the work was conducted at the community level, in schools, workplaces or by door-to-door personal interviews and telephone surveys. Few publications (19.4%) were multicentred, and multicentred studies were least likely to be found from the poorest nations.
Medication-related studies, clinical research involving a drug treatment, its efficacy, or side-effects, accounted for 15% of all LAMI research, whereas clinical studies not involving drugs made up the largest proportion (40%; Fig. 1). Epidemiological studies, including those concerned with prevalence and patterns of headache disorders at a population level, accounted for 37.0% of all LAMI research. Economic or health services capacity research, including articles involving cost, expenditure and healthcare workers, made up only 7.9%.

Theme of publications on primary headache disorders from low- and middle-income countries, 1997–2006.
Journals publishing ≥ 10% of the literature on primary headache disorders from LAMI countries included Cephalalgia and Headache amongst the headache-specific journals and Arquivos de Neuro-Psiquiatria among the general medical and neurological journals.
Discussion
The burden of neurological illness has been underestimated (4), and this burden is largest in LAMI countries, where 85% of the world's population live (3). The paucity of research from the most populous areas of the world is not surprising. An imbalance in research contributions between high-income countries and the rest of the world has been found in multiple medical specialties, confirming that LAMI countries, although accounting for the majority of the world's population, receive < 10% of the world's research funding and contribute approximately 10% of the existing clinical and scientific literature (8). Where recognized, this has been described as ‘the 10–90 divide’ (8).
When evaluated formally, however, various disciplines show the 10–90 divide to be an overestimation of the contribution from LAMI countries, including mental health disorders (6%) (9), ophthalmology (5%) (10), gerontology (< 5%) (11), virology (‘very low’) (12) and general surgery (13). Where studied, the trend is for this to remain undiminished (9–12). In the case of dementia, it has been found that < 10% of all population-based research has been dedicated to the two-thirds or more cases of dementia that exist in the developing world (14).
To establish whether the 10–90 divide applies to the headache literature is difficult. Many ‘international’ medical databases are developed in the USA. Whereas a country name is a keyword for publications when the work is derived from LAMI countries, this is not the case for high-income country publications. Thus, keyword searches for ‘headache’ and ‘United States’ or ‘United Kingdom’ reveal only a fraction of the articles that exist from these countries. In this study, the total number of publications from high-income countries was not determined, but a search to confirm the output of each high-income country revealed that 68% have published research in the time period of study (Table 2).
One limitation was our language criteria. An unknown proportion of articles are produced and found in non-English databases, although approximately 90–96% of the world's scientific literature is now published in English (15, 16). It is possible that country-specific databases exist that have not been included in this search. Countries that have their own databases (e.g. Nepal, the Philippines, India and Iran) have a resultant stronger representation than those countries that do not. Some articles may have been published in non-indexed journals that were not included in this search. In some cases, the research that is being done in LAMI countries may not be adequately represented by counting publications, as indicated by interviews with researchers in Pakistan (15).
Certain LAMI studies (17) were multicentred and evaluated the prevalence and characteristics of headache in multiple countries, comparatively, within a single publication. Such an article was counted multiple times, once for each country that contributed to the final article. Thus, in spite of the paucity of literature discovered, this study overestimated the absolute number of publications coming from LAMI countries. Additionally, articles performed by authors from high-income countries about LAMI countries, with or without collaboration from authors or resources in that country, were attributed to the LAMI country (18, 19). This also led to an overestimation of the resources available in LAMI countries.
LAMI countries may falter in the publication of clinical literature for a number of reasons that apply for many health conditions. At outset, a person in a low-income country usually faces a lack of resources, lack of formal training in research methods and advice, and lack of access to medical information and published literature, including the internet (8, 9, 20). In clinical fields, a professional brain drain on health and science personnel in the developing world leaves less time for academic pursuits (21). There is an inverse linear correlation between the income of the country and the number of randomized controlled trials produced (22). What is intellectually difficult can become technically difficult also; for example, studies of prevalence in low-income countries are sometimes performed via time-consuming door-to-door surveys, as demonstrated in Tanzania (18). Finally, when research data are produced, authors may face language barriers, publication bias and even racism (23). Limited appreciation by the reviewers and editors of the realities of doing research in LAMI countries may constitute publication barriers. LAMI country research is rare if not absent in high-impact journals (13, 24) and, where present, is frequently performed by high-income country authors. This under-representation in high-impact journals is greater than can be explained by underfunding of research (25). The small amount of published literature from LAMI countries that does exist tends to be found (or not found) in journals that are not cited in prominent international databases (15), and a published paper may therefore have no tangible effect on real life in the developing world (26). Headache disorders, in particular, may be a low priority for funding agencies and researchers as well as editors and reviewers of general medical journals. Thus, sizeable challenges are extant in the research and management of headache disorders in LAMI countries.
Classification by WHO regions demonstrates that LAMI countries are more likely to produce research in headache disorders if they are in certain regions of the world. LAMI countries of the Western Pacific and African regions were least likely to produce research, but LAMI countries in the European and American regions also had very little output considering the numbers of participating countries. Although having high-income country neighbours appears to help a LAMI country's research output, encouraging participation in multicentred studies by an otherwise unpublished country, the benefit appears not to be widespread. The research output of countries neighbouring Brazil was increased through participation in multicentred studies that also included Brazil, but otherwise there was no increase in research publication output by countries that neighboured highly productive countries.
The reasons why certain LAMI countries are successful at performing and publishing research is worthy of further study. In this review, Brazil, Turkey and Iran published by far the most manuscripts. Together, they accounted for half of the total amount of LAMI research in the past decade. Notably, all three countries are of middle-income categorization. In these countries, isolated academic centres may have a prolific researcher or group of researchers increasing the number of research publications for the entire country. Also, local journals with a priority for local data, indexed in a country-specific database, allowed Iran to have a more visible output of research than its neighbouring countries. More than 80% of the articles from Iran were published in local or national medical journals. Thus, strengthening country-specific journal publications may provide the opportunity to share local epidemiological data that might otherwise go unpublished in international forums.
Significant investment by pharmaceutical companies exists in selected LAMI countries in economic transition. These countries may have the impetus and funding to pursue research in greater quantity and with better chance of publication. Thus, a variation among the LAMI countries almost certainly exists, with some highly prolific countries masking the effects of little to no research from the majority.
On the public health agenda, headache disorders are often overlooked, probably because they are not fatal. Therefore, significant gaps exist regionally, financially and intellectually in our current understanding of these disorders at a public health level. In order to address these gaps, ‘Lifting The Burden: the Global Campaign to Reduce the Burden of Headache Worldwide’ was launched in 2004 by the WHO in partnership with three international non-governmental organizations: the World Headache Alliance, the International Headache Society and the European Headache Federation. One of the campaign's objectives is to raise the priority given to the care of people with headache throughout the world, expressly including developing countries (3). The campaign argues that ‘in order that proposed solutions reflect the needs of patients in developing countries, and not only the needs perceived by the developed world, direct support must be provided for studies that aim to understand headache burden and health-care gaps in these countries’.
It is necessary for multiple organizations and individuals to participate in recognizing the burden of headache disorders worldwide. This includes international organizations such as WHO, non-governmental organizations, and editors and reviewers of medical journals. The tasks must be (i) to examine the existing research capacity in headache disorders, (ii) to support researchers and journals from LAMI countries, and (iii) to enhance dissemination of research publications from LAMI countries. This would help—in fact, it is crucial—in addressing the significant gaps in headache care from a global perspective, and in strengthening existing health systems so that they better recognize headache disorders worldwide.
Competing interests
None to declare.
Acknowledgements
The authors thank Mr Tomas Allen (librarian, World Health Organization, Geneva, Switzerland) for his assistance in identifying international online search engines, essential for this project, and Dr Afarin Rahimi Movaghar (Tehran University of Medical Sciences, Tehran, Iran) for assistance in obtaining articles from the IranMedex database.
Footnotes
Appendix
List of databases searched (in alphabetical order) for the review of research in primary headache disorders from low- and middle-income countries (n = 67)
| Abledata |
| African HealthLine |
| African Index Medicus |
| African Journals OnLine |
| African Women's Bibliographic Database |
| Bibliographic Databases of Theses in Bamako, Mali (AHILA) |
| Bioethics Literature Database (BELIT) |
| Bioline International |
| British Education Index |
| Canary Databse |
| CCMed |
| Centre for Reviews and Dissemination (CRD) |
| Child Health and Nutrition Research Initiative (CHNRI) |
| Center for International Rehabilitation Research Information and Exchange (CIRRIE) |
| Combined Health Information Database (CHID) |
| Database of Promoting Health Effectiveness Reviews (DoPHER) |
| Database of African Theses and Dissertations |
| Development Policy Review Network |
| Directory of Published Conference Proceedings |
| Disablity INFormation Resources (DINF) English Index |
| Diversity Health Institute Clearinghouse |
| Economic Papers |
| Embase |
| Education-line |
| Education Resources Information Center (ERIC) |
| Euroethics |
| European Health for All Database (HFA-DB) |
| Findarticles |
| Health Disparities Community Solutions Database |
| Health Literature, Library and Information Services (HELLIS) |
| Health Research and Development Information Network (Philippines) |
| Health Sciences Bibiliographies of Nepal Databases |
| Hungarian Medical Database |
| IFPMA Clinical Trials Portal |
| Index Medicus for the South-East Asian Region |
| IndMed |
| INRUD Drug Use Bibliography |
| Institute of Tropical Medicine (ITM) |
| IranMedex |
| Japan Science and Technology Information Aggregator |
| KIT (Netherlands) |
| KoreaMed |
| Latin American and Caribbean Center on Health Sciences Information (LILACS) |
| Multilingual Library – eurasiahealth |
| NARIC |
| ODS |
| ONESOURCE |
| OpenMED |
| OSTMED |
| Physiotherapy Evidence Database (PEDro) |
| Pharm-line |
| Popline |
| PubMed – National Library of Medicine |
| Regional Database of Arabic Medical Books |
| Rehabilitation Database Index |
| Research and Development Resources Base |
| Science Research Portal |
| Sharing Point |
| Sport & Leisure Index |
| Social Care Online |
| Social Psychology Network |
| Social Science Information Gateway |
| Synergy HIV/AIDS |
| Topics in Medical Education |
| TroPHI |
| Turkish Medicine |
| Violence Literature Database Search |
